
Abstract
ST elevations on the electrocardiogram (ECG) can be caused by a number of conditions, including ST-elevation myocardial infarction (STEMI), pericarditis, Takotsubo cardiomyopathy, and coronary spasm. A holistic approach, incorporating clinical examination and history, is required to arrive at the correct diagnosis rather than anchoring on ST elevation on ECG alone.
Clinical Vignette
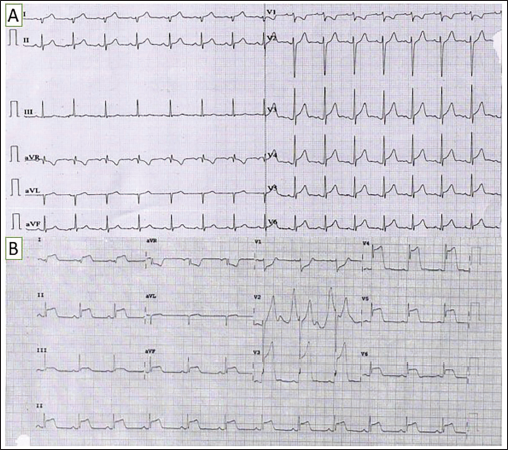
A 19-year-old male, with no known comorbidities, came to the hospital with central chest pain radiating to the left shoulder of 1 h duration. He did not give a history of sweating, palpitations, fever, cough, syncope, or shortness of breath. On examination, his blood pressure was 110/70 mm Hg, and his pulse was 86/min. The electrocardiogram (ECG) at presentation is shown in Figure 1A. Troponin was negative. Initial echocardiography did not reveal any wall motion abnormality. He was reassured and discharged home. He came back 24 h later with persistent chest pain; ECG is shown in Figure 1B. What is the probable diagnosis and the further line of management?
(A) 12-lead Electrocardiogram (ECG) at Presentation. (B) ECG Repeated 24 h Later.
Explanation
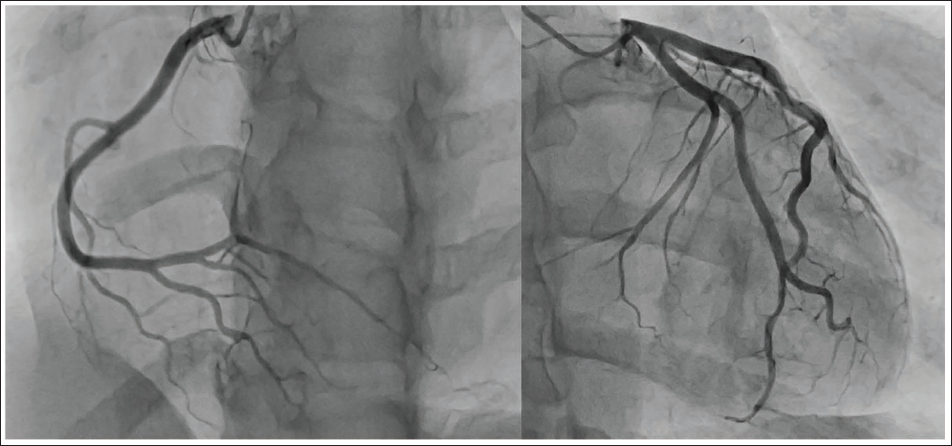
The ECG at presentation (Figure 1A) shows sinus rhythm, with subtle J-point elevation in leads V3-V6. The chest pain was atypical on a clinical background of low cardiovascular risk; there were no dynamic changes in the repeat ECG, and troponin was negative; thus, the patient was discharged. The patient came back 24 h later with persistent chest pain. The repeat ECG (Figure 1B) showed diffuse gross ST elevation (maximum being 7 mm in leads V3-V4) in the inferolateral leads and precordial leads V3-V6. There were ST depressions in the leads aVR and V1, with bizarre T waves in lead V2 resembling hyperacute T waves. Such stark ST elevations resembling the tombstone pattern often suggest an ominous diagnosis of an acute ST-elevation myocardial infarction (STEMI). 1 The repeat troponin level was also elevated this time (troponin I 100 pg/mL, reference <19 pg/mL). However, echocardiography did not reveal any obvious wall motion abnormality or valvular abnormality. In view of ongoing chest pain, elevated troponin, and ECG changes, the patient was taken up for an urgent coronary angiography, which turned out to be normal (Figure 2).
Coronary Angiography Showing Normal Coronaries.
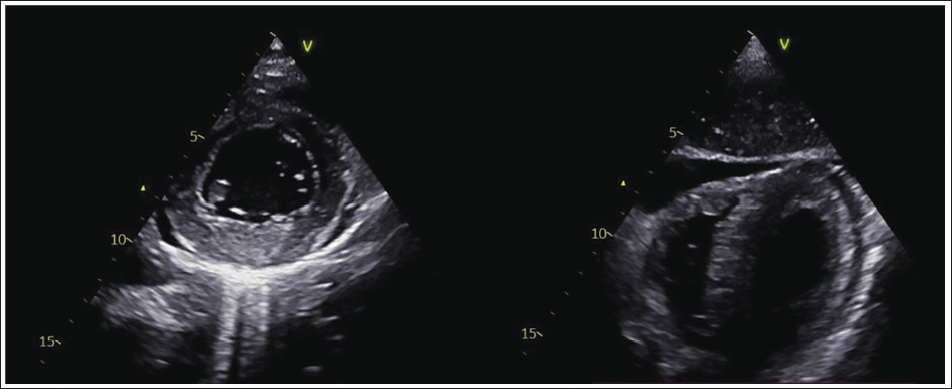
The patient was referred to our hospital for further workup of myocardial infarction with no obstructive coronary artery disease. However, a closer look at the presenting ECGs suggests that the diagnosis of ischemia is unlikely. The ST elevations are concave upwards rather than the convex elevations seen in STEMI. The pattern of involvement does not conform to any coronary artery block pattern. Moreover, the reciprocal changes in the form of ST depression are conspicuously absent. These features strongly suggest against a diagnosis of acute ischemia caused by coronary spasm or acute obstruction. The clinical picture of pleuritic-type central chest pain in a young adult with diffuse ST-T wave changes points toward a diagnosis of acute pericarditis. This was confirmed with the presence of pericardial rub and a mild pericardial effusion on bedside echocardiography (Figure 3). There were no wall motion abnormalities noted on echocardiography.
The most sensitive ECG finding in pericarditis is diffuse concave ST elevations and ST depression in leads V1 and aVR due to a repolarization abnormality caused by pericardial inflammation. It is found in 60%-70% of patients. 2 The most specific ECG finding is Spodick’s sign—PR segment depression—which is found in 30% of the cases due to the sup-epicardial atrial injury. 3 Although uncommon, gross ST elevations may sometimes be seen in acute pericarditis, as in the present case. The most common cause of acute pericarditis is viral, and aggressive etiological workup is not recommended in the absence of high-risk features and systemic inflammatory disease.
The other possible differential diagnoses of these ECG changes include takotsubo cardiomyopathy and ECG artefacts. Takotsubo syndrome may present with ST elevation in the anterior leads and with a prolonged QT interval. 4 It is often associated with ST depression in lead aVR and T wave inversions in multiple leads. Absence of any LV dysfunction ruled out takotsubo cardiomyopathy in this case. The bizarre T waves in lead V2 and diffuse ST elevations raise the possibility of an artifact with electromechanical association. However, the presence of dynamic changes in multiple ECGs at different times makes artifacts very unlikely. Moreover, the ECG in Figure 1B has ST elevation in all three limb leads—I, II, and III—without the classical sparing of one of the limb leads associated with synchronized pulse-tapping artifact. 5
Beside Echocardiography in Parasternal Short Axis View and Subcostal View Showing Mild Pericardial Effusion. No Regional Wall Motion Abnormalities Were Noted.
The patient was treated for acute pericarditis with ibuprofen, leading to significant clinical improvement along with further progression of ECG changes toward T wave inversions and complete resolution of pericardial effusion on echocardiography. There was no evidence of constriction or recurrence on follow-up over the past 6 months. This report highlights the importance of not anchoring to a diagnosis based solely on the ECG finding of ST elevation and having a holistic approach toward a clinical diagnosis. Further, it is important to recognize the differences in ST elevations of STEMI and acute pericarditis. This may prevent unnecessary catheterization, anticoagulation, and hospital admission, as in the given case.
Data Availability Statement
All data are incorporated into the article and its online supplementary material.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable as it is an anonymous case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Obtained from the patient in line with COPE guidance.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.