
Abstract
Persistent chest pain is an uncommon entity in adolescent population, with majority of cases having no discernible cardiac etiology. We report a young boy presenting with chest discomfort due to underlying large pericardial hydatid cyst. Initial diagnostic confirmation was based on classic echocardiographic features, including presence of sonographic water lily sign. Patient subsequently underwent successful surgical excision of cyst under cardiopulmonary bypass, along with perioperative antihelminthic and anti-inflammatory drug therapy. Patient continues to remain symptom free on follow-up, with no recurrence in cyst formation. This case highlights the high index of suspicion needed in diagnosing such atypical cardiac cysts, especially in patients from endemic zones.
Introduction
Pericardial cysts are extremely uncommon in younger population, with majority of cases seen post third decade of life. 1 Vast majority of these cysts remain asymptomatic for prolonged periods, owing to benign nature in the more common congenital cysts. 2 However, the lesser common acquired inflammatory cysts can lead to symptoms that range from fever, cough to chest pain, dyspnea, and acute life-threatening events. We report an acquired case of a large pericardial cyst that manifested with persistent chest pain and low-grade fever.
Clinical Summary
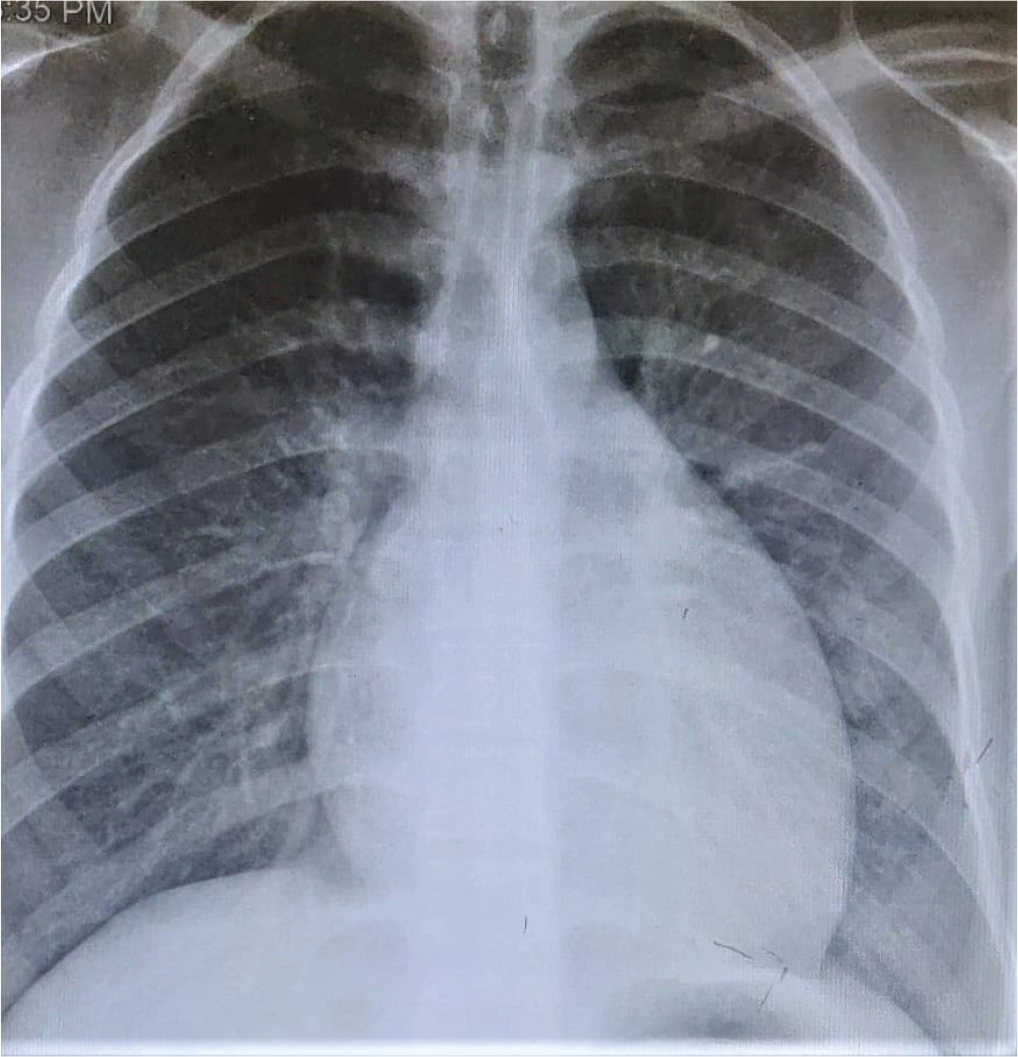
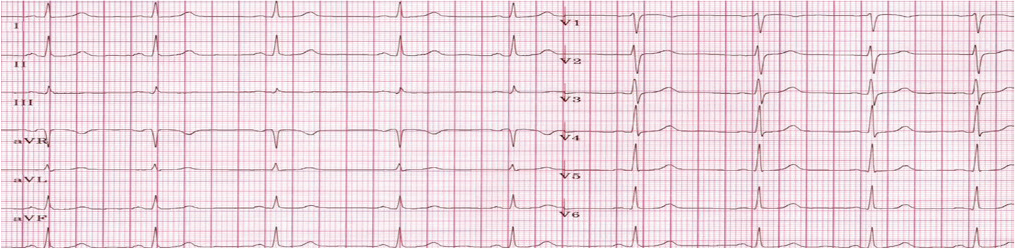
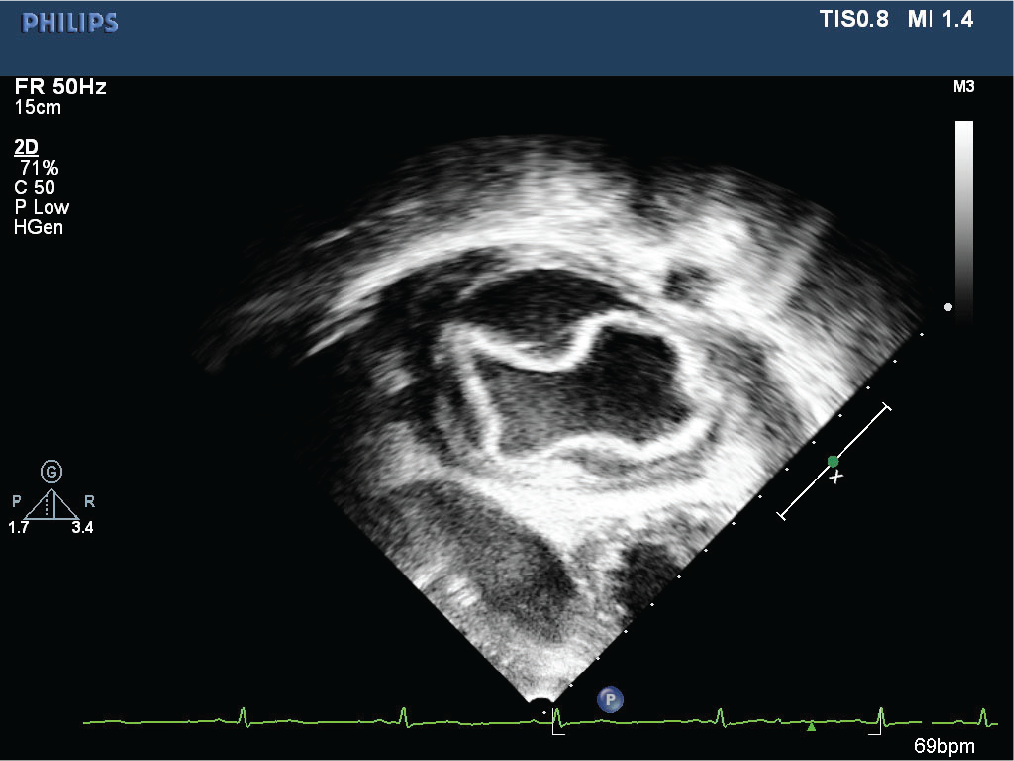
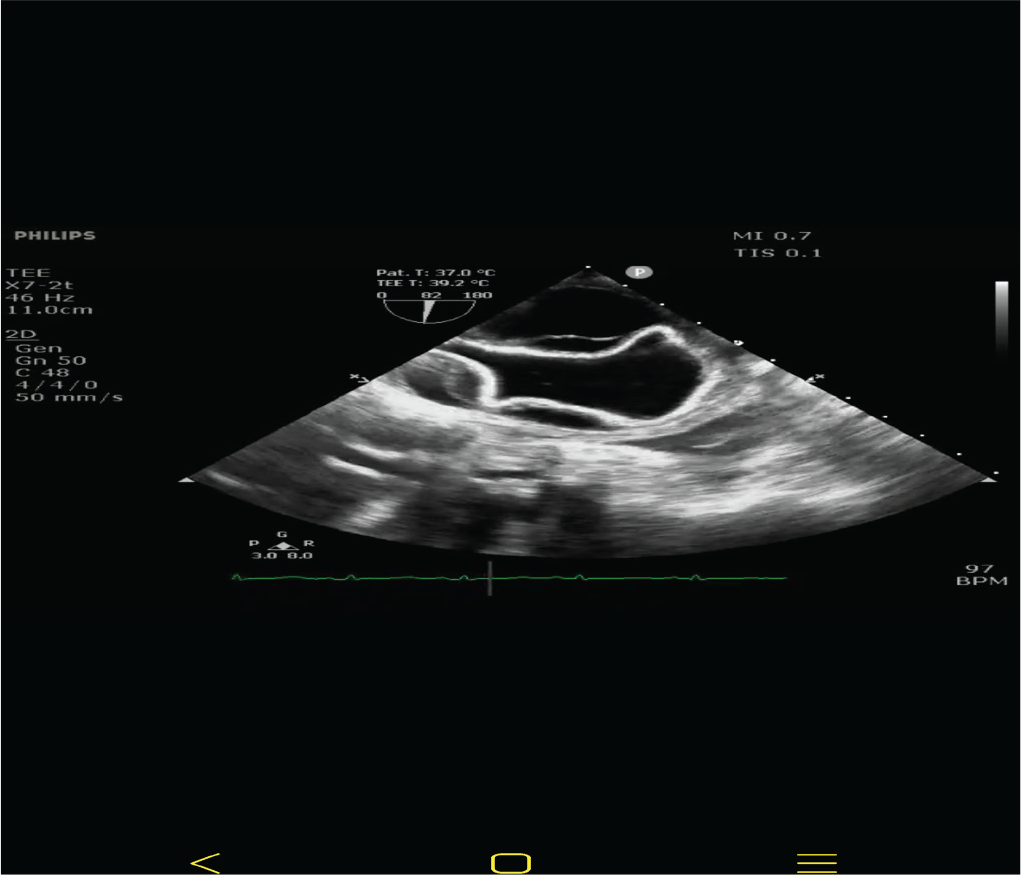
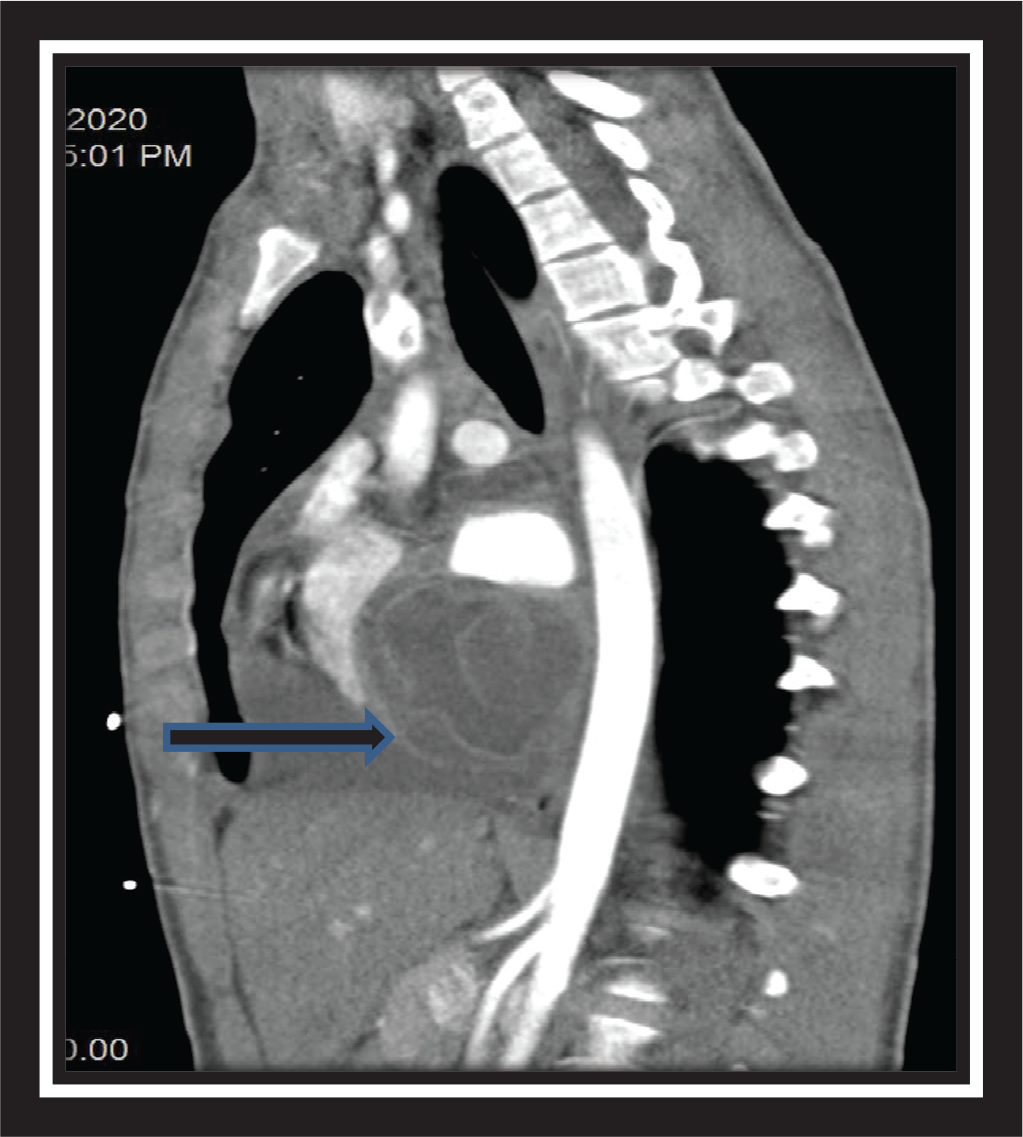
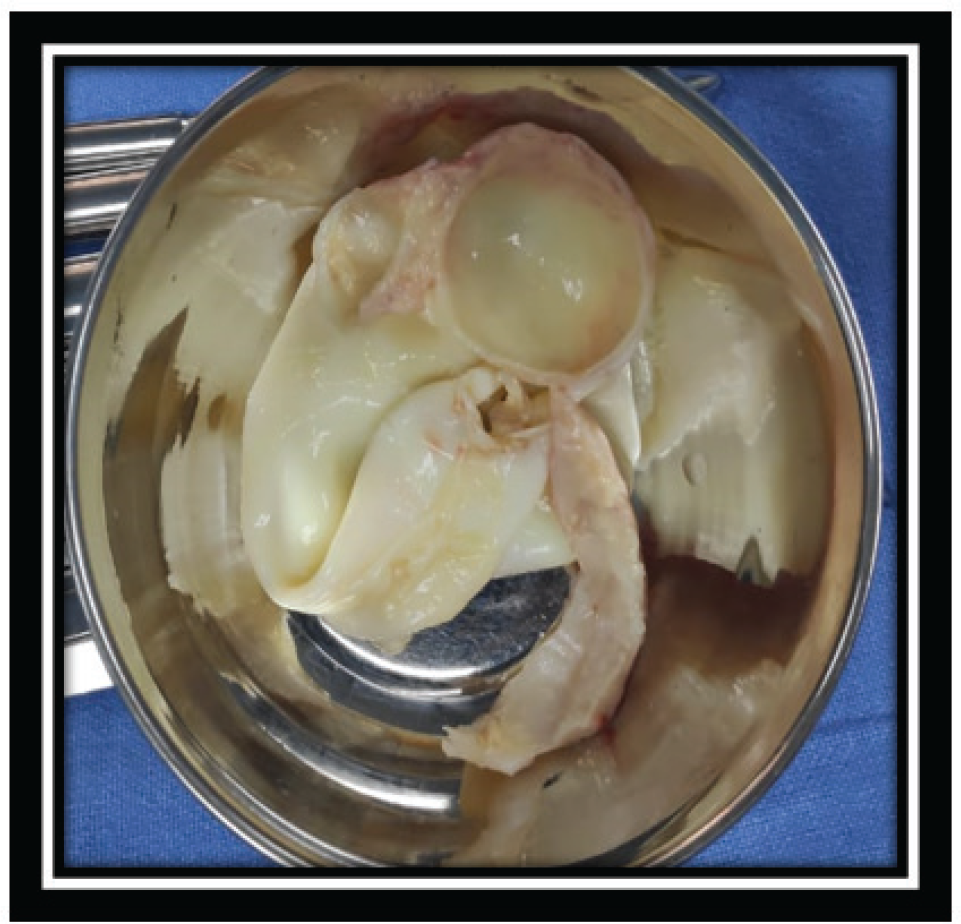
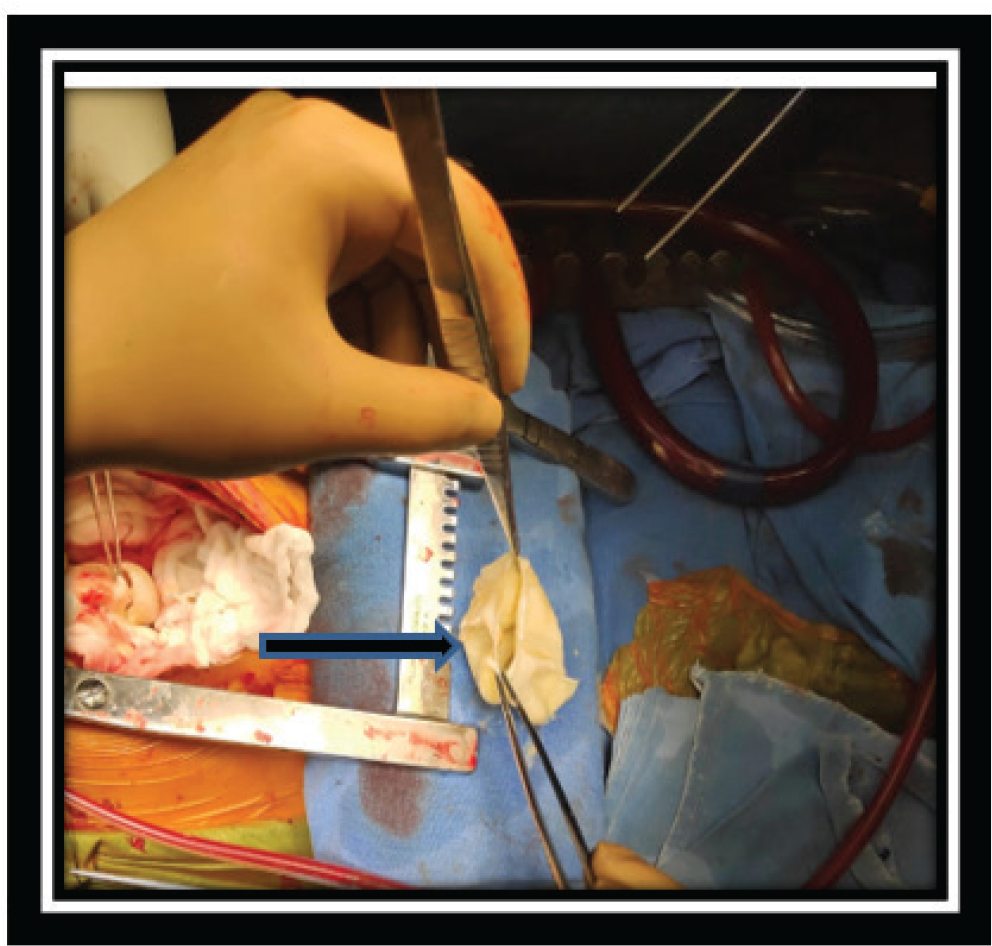
A 17-year-old boy was referred from Srinagar, Kashmir with complaints of low-grade fever with dull precordial and retrosternal chest discomfort of 2 weeks duration. Initial evaluation at a local center was suggestive of borderline cardiomegaly on chest radiographs and a normal electrocardiogram, mandating further cardiac evaluation (Figures 1 and 2). On initial evaluation, patient was well built, afebrile, and hemodynamically stable with normal cardio respiratory examination. Peripheral pulses were well felt and blood pressure was normal in all limbs. Initial transthoracic echocardiogram showed a large cystic mass of 7.3 cm × 3.2 cm in posterior pericardial space, abutting both atria posteriorly. In addition, there was moderate circumferential pericardial effusion with normal cardiac function. Detailed echo evaluation showed a large univesicular echolucent cyst, with a floating and collapsing internal membranous structure representing endocyst (Figures 3 and 4). These echo findings such as classical water lily sign were diagnostic of cardiac echinococcosis. Diagnosis was further confirmed by contrast enhanced computed tomography (CT) chest that showed a massive 9 cm × 6 cm × 6 cm purely cystic lesion arising from pericardium with a detached floating hyperdense membrane in inferior pericardial space beneath right atrium and right ventricle, causing minimal compression of inferior vena cava and coronary sinus (Figure 5). Blood workup showed supportive eosinophilia (24%). No similar cysts were detected in pulmonary and abdominal imaging. Detailed ocular examination was normal. Central nervous system imaging was avoided due to lack of suggestive symptoms and financial constraints regarding advanced imaging. In view of symptomatic status of patient and a large cyst abutting adjacent venous drainage, surgical excision was planned with backup of cardiopulmonary bypass, if needed. Patient received preoperative antihelmithic therapy with steroid for 48 h and subsequently underwent surgical excision. Inspection on surgical table revealed a large pericardial cyst which was adherent to the interatrial septum and difficult to mobilize. In view of this, cardiopulmonary bypass was initiated. After instituting aorto-bicaval cannulation and cardioplegia, cyst was inspected and transparent watery cyst fluid aspirated. Cyst was injected with 20% hypertonic saline as a scolicidal agent, followed by reaspiration and thorough curettage. Due to underlying dense adhesions, pericyst was left attached to pericardium, while a large whitish smooth surfaced endocyst was removed en masse (Figures 6 and 7). In addition, patient was also started on perioperative antihelminthic therapy with oral albendazole 400 mg twice daily and oral praziquantel 1,500 mg per day, along with anti-inflammatory cover initially with intravenous hydrocortisone followed by oral indomethacin. Post-operative echocardiograms showed no residual cysts with normal cardiac function and trace effusion. Patient remained symptom free and was discharged on oral antihelminthic therapy for 3 months. Histopathological examination of excised cyst was further confirmatory for hydatid cyst with presence of outer acellular laminated membrane, fibrocollagenous tissue, and moderate inflammatory infiltrate without any evidence of neoplasia or granulomas.
Patient continues to remain symptom free after completion of 3 months of antihelminthic therapy. There was no evidence of cyst recurrence on echocardiograms at 6 months follow-up.
Discussion
Cystic echinococcosis or hydatid disease occurs due to endoparasitic infestation by Echinococcus granulosus tapeworm. It is considered an endemic disease in populations having close interaction with livestock, as seen in high prevalent states like Kashmir, Uttar Pradesh, and Andhra Pradesh. 3 However, cardiac hydatid disease is extremely rare among these patients, seen in only 0.2% to 2% of all cases.4, 5 After gaining access to thoracic duct and venous circulation, granulosus larvae reach pulmonary capillaries, and disseminate across systemic supply. Rich coronary circulation accounts for left ventricle being the most common site of hydatid cysts in 55% to 60% of all cases, followed by right ventricle, interventricular septum, atria, and pericardium.6-8 Isolated pericardial hydatid cysts are extremely rare. Salati et al 9 in one of the largest retrospective 18 year-long study from Kashmir, reported isolated pericardial hydatid cysts in only 11 (1.4%) of all cases of cardiothoracic hydatid cysts, underscoring the rarity of such presentation. 9
Presentation of cardiac hydatid cysts is variable and depends on size, number, location, and integrity of individual cysts. Usually these lesions are uncommonly detected in children, owing to their slow growth over a period of time. Clinical presentation could be in the form of incidental detection on imaging studies, mechanical complications (due to pericardial effusion, valvar damage, and coronary compression), rhythm disturbances, or complications arising due to sudden rupture of cyst. 10 Sudden rupture of hydatid cyst can be life threatening manifesting as anaphylactic shock, cardiac tamponade, and even pulmonary embolism. 10
Diagnosis of cardiac hydatidosis is established by typical imaging findings on transthoracic echocardiography, transesophageal echocardiography, magnetic resonance imaging (MRI), and CT. Typical sonographic characteristics correlating with staging of hydatid cysts have been set forth by WHO, dividing hydatidosis into 6 different categories and 3 clinical subgroups. 11 In our patient, presence of water lily sign on echo reflected a degenerating cyst with a floating detached endocyst membrane. Such findings reflect a state of transitional cyst undergoing some degree of degeneration. Water lily sign represents collapsed membranes of cyst that may be seen floating on the surface of the cyst, and are diagnostic of hydatid cysts. 12 Contrast enhanced CT scans show hydatid cyst as cystic and hypodense structures with contrast agent accumulating in walls as was seen in our patient. On MRI in MRI-T2 images, cysts appear with a high signal intensity, whereas cysts in MRI-T1 images are presenting hypointense or show an intermediate signal intensity. 13
Peripheral blood eosinophilia as seen in our patient is a common occurrence seen in up to 25% of patients with cardiac echinococcosis. 7 Serological testing with ELISA as a screening test to detect antibodies against E. granulosus has high sensitivity albeit lower specificity, with usage limited by high false positivity in patients with systemic diseases. 7 Other methods are the indirect hemagglutination test and the latex agglutination test. Other less commonly performed tests include genotype analysis for echinococcosis and microscopic examination of aspirated fluid for protoscolices.
In our patient, treatment comprised of en masse surgical excision under cardiopulmonary bypass with perioperative medical therapy. Surgical excision can be complicated by dense adhesions making en masse removal difficult; however, as was done in our case, repeated irrigation with scolicidal agents to kill worms and a deep curettage to prevent leaving out daughter cysts is recommended.7, 8 Although there are no definitive treatment guidelines for managing cardiac hydatid cysts, surgical resection along with antihelminthic therapy is considered the treatment of choice.5, 7, 14 Owing to high risk of rupture during operative handling, presence of dense attachments to underlying structures and a high perioperative mortality of 4% to 10% cardiopulmonary bypass is often required in large cysts as has been previously reported. 14 Occasionally, large residual pericysts might need stabilization with pericardial or Dacron patch to prevent rupture. 7 Long duration antihelminthic therapy for a minimum of 3 months with oral benzimidazoles (albendazole at 15 mg/kg day) is recommended.7, 15 Additional praziquantel at 40 mg/kg/day in select cases with large cysts has also been advocated for better results.7, 15 Antihelminthic therapy does reduce size of cyst wall and has greater role in patients who refuse surgery, or are considered technically inoperable due to surgically inaccessible cysts. However, one has to be watchful of adverse effects associated with such tubulin polymerization inhibitors considering their teratogenic, hepatotoxic, and myelotoxic nature.
In our patient, there was no recurrence in symptoms or cyst on serial echocardiography up to 6 months. There were no systemic symptoms warranting further extensive evaluation. Although the exact risk of recurrence is not known, long-term follow-up is needed in these patients due to scattered reports of cyst recurrences as well as cardiac mortality in some. 14
Implications for Practice
This case highlights the high index of suspicion needed in diagnosing atypical cardiac mass lesions in younger population. Management decisions are complex and need to be individualized based on relevant surgical anatomy. However, a team approach involving cardiologists, cardiac surgeons, and infectious disease specialists often leads to highly successful treatment results.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.