
Abstract
Valvular aortic stenosis (AS) is a progressive disease that affects 2% of the population aged 65 years or older. The major cause of valvular AS in adults is calcification and fibrosis of a previously normal tricuspid valve or a congenital bicuspid valve, with rheumatic AS being rare in the United States. Once established, the rate of progression of valvular AS is quite variable and impossible to predict for any particular patient. Symptoms of AS are generally insidious at onset, though development of any of the three cardinal symptoms of angina, syncope, or heart failure portends a poor prognosis. Management of symptomatic AS remains primarily surgical, though transcatheter aortic valve replacement (TAVR) is becoming an accepted alternative to surgical aortic valve replacement (SAVR) for patients at high or prohibitive operative risk.
Keywords
Introduction
Aortic stenosis (AS) is a hemodynamically significant narrowing of the outlet of the left ventricle with multiple potential etiologies, whereas aortic sclerosis is a thickening or calcification of the aortic valve without obstruction to left ventricular outflow. Depending on the level of the obstruction, AS is classified as valvular, sub-valvular, or supra-valvular. This article reviews the etiology, pathophysiology, diagnosis, and management of valvular AS in adults.
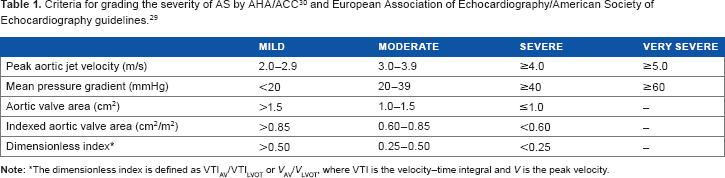
The prevalence of valvular AS in the population aged 65 years or older is approximately 2%, while another 25-30% have aortic sclerosis.1,2 A normal aortic valve area is approximately 3-4 cm2, and symptoms of AS tend to develop when the aortic valve area is 1 cm2 or less. The severity of AS, which will be discussed in detail later in this article, is graded by the criteria listed in Table 1. While congenital malformation of the aortic valve and rheumatic heart disease predispose to aortic valve calcification and stenosis, senile calcification of a previously normal trileaflet valve is an important and frequent cause of valvular AS.
The normal aortic valve is a trileaflet structure located at the junction between the left ventricular outflow tract and the aortic root. The leaflets are composed of three distinct layers, which from the aortic to ventricular surface are the fibrosa, spongiosa, and ventricularis. This leaflet structure is covered on both the ventricular and aortic surfaces by endothelium in continuity with both the ventricular endocardium and the aortic endothelium. Each layer of the aortic valve has a distinct structure and function: the fibrosa contains circumferentially oriented collagen fibers, which provide most of the strength of the leaflets; the spongiosa is found at the bases of the leaflets, contains mucopolysaccharides, and functions to resist compressive forces and facilitate movements between the fibrosa and ventricularis during leaflet motion; and the ventricularis contains radially oriented elastin and contributes to the flexibility of the leaflets. Valve interstitial cells are found in each of these layers and have distinct sub-populations that regulate homeostasis within the valve leaflets.3–5 The entire right coronary leaflet and most of the left coronary leaflet arise from ventricular myocardium, while part of the left coronary leaflet and the majority of the non-coronary leaflet are in continuity with the anterior leaflet of the mitral valve. Of particular relevance to any discussion of aortic valve pathology and its invasive treatment is the fact that there is no singular “aortic annulus.” Rather, there are three rings near the aortic valve. From most ventricular to most aortic in location, these are: the ring formed by the basal attachments of the aortic valve leaflets, the anatomic ventriculoarterial junction, and the sinotubular junction. The aortic valve leaflets are attached in a “crown-like” ring spanning the distance between the basal attachments and the sinotubular junction, and it is this ring that is generally referred to as the surgical annulus. The coronary arteries usually arise below the sinotubular junction, but occasionally arise above. Finally, and of major clinical importance, the left bundle branch runs just inferior to and between the right coronary cusp and the non-coronary cusp of the aortic valve. 6
Development of AS from a previously normal valve progresses over decades and begins with subclinical inflammation, advances through a stage of fibrosis and thickening of the valve, and eventually results in valvular calcification. Inflammation may develop as a result of damage to the valvular endothelium due to abnormal flow in a tricuspid or congenitally malformed aortic valve, due to chronic inflammation resulting from rheumatic heart disease, or from any of a number of other causes. Regardless of predisposing or initiating factors, the vast majority of stenotic aortic valves in adults are heavily calcified by the time they cause symptoms of AS. As the aortic valve becomes progressively calcified, the leaflets become less mobile, the aortic valve orifice becomes increasingly stenotic, and the normal flow of blood from the heart is progressively obstructed.
While the development of AS was once thought to be a passive process, we now realize that the aortic valve is a dynamic environment involving a complex interplay between valvular endothelial cells, valve interstitial cells, inflammatory cells, and the extracellular matrix.3–5 However, the pathophysiological mechanisms underlying the development and progression of AS remain poorly understood. There is marked similarity between the histopathological features of AS and those of atherogenesis, including initial endothelial damage, the deposition and oxidization of lipid-rich particles at these vulnerable sites, neoangiogenesis, chronic inflammation, and eventual calcification. 4 Over the last two decades, studies have shown an association between aortic valve calcification and traditional risk factors for atherosclerotic cardiovascular disease, including age, male gender, smoking, hypertension, low-density lipoprotein cholesterol (LDL-C) levels, and diabetes mellitus.2,7 Furthermore, the apolipoprotein E allele, apoE4, which has been shown to be associated with an increased risk for coronary heart disease, is also associated with the development of AS. 8 In addition, there is evidence that certain polymorphisms in the lipoprotein(a) gene may play a causal role in calcification and stenosis of the aortic valve. 9 Several studies have also suggested a role for nitric oxide resistance and reactive oxygen species.10–12 However, three prospective, randomized, controlled studies have shown the failure of lipid-lowering therapy to halt or slow the progression of AS and associated outcomes, and a retrospective case–control study suggested that high-dose atorvastatin did not prevent the development of calcific AS.13–16 Thus, there is growing evidence that atherosclerosis and AS, although sharing some pathophysiological features, have important differences in pathogenesis with considerable implications for treatment.
Therefore, a broad search for the causative factors in AS is underway. The mechanisms of progressive aortic valve calcification are an appealing target, because elucidation of these would likely provide targets for treatments aimed at preventing the progression of AS or even reversing the process. There is some evidence that valve interstitial cells and valve endothelial cells can be transformed into osteoblast-like cells and thereafter likely contribute to ongoing valvular calcification.3,5 Furthermore, mutations in NOTCH1, a signaling protein involved in regulation of osteoblasts, have been proposed to result in a bicuspid aortic valve and calcific AS. 17 Finally, broad genomic screens 18 and more focused genetic studies19–21 offer another angle of attack to determine the critical pathways by which normal aortic valves progress to severe AS.
Congenital abnormalities of the aortic valve frequently predispose to AS. A bicuspid aortic valve is the most common congenital abnormality associated with AS and is found in 1-2% of the general population. 22 One single-center study of 932 consecutive patients who underwent aortic valve replacement for AS without mitral stenosis (thus excluding most rheumatic disease) found definite congenital abnormalities in 54% of the aortic valves, with 5% being unicuspid valves and the remainder bicuspid. 23 In the same study, the average age of valve replacement in those with a bicuspid valve was 67 ± 11 years, compared with 51 ± 14 years in those with unicuspid valves and 74 ± 8 years in those with tricuspid valves. 23 However, the exact prevalence of congenital aortic valve abnormalities in patients undergoing aortic valve replacement for AS varies depending on the inclusion criteria.24–26 Importantly, a bicuspid valve can be associated with coarctation of the aorta, ascending aortic aneurysm, aortic dissection, infective endocarditis, Turner's syndrome (the absence of one × chromosome), a ventricular septal defect, and Shone's syndrome (supra-valvular mitral ring, parachute mitral valve, subaortic stenosis, and aortic coarctation).22,27
Rheumatic heart disease is rare in the United States but remains an important cause of AS in developing countries. Rheumatic AS is characterized by fusion of the valve commissures because of an inflammatory response, which predisposes to further valvular injury and eventually results in valve fibrosis and calcification. Furthermore, rheumatic AS is almost always seen in conjunction with rheumatic mitral stenosis as the mitral valve is more frequently affected by rheumatic heart disease than the aortic valve.
Regardless of the etiology, valvular AS results in a fixed obstruction to left ventricular outflow. By Ohm's law (
Clinical Manifestations
The three classic symptoms of AS are exertional angina, syncope, and heart failure. 28 However, symptoms are frequently insidious at the onset and can be highly variable among patients with similar degrees of valve stenosis. Many patients note a subtle decrease in exercise tolerance as the first symptom of AS. Furthermore, AS tends to be quite advanced by the time it results in clinical symptoms. In the original report by Ross and Braunwald, the mean survival after the onset of angina, syncope, and heart failure was five, three, and two years, respectively.
Angina results from an imbalance in myocardial oxygen supply and demand. Angina in the setting of aortic valve stenosis may be secondary to the development of concomitant coronary artery disease but may also occur in the absence of fixed atherosclerotic disease. Increased myocardial oxygen demand is a result of hypertrophy of the left ventricle and the increased afterload conferred by the fixed obstruction to left ventricular outflow. Decreased myocardial oxygen supply is a result of both reduced mean arterial pressure and decreased coronary blood flow. As the severity of valvular obstruction increases, the systolic ejection period is lengthened, which necessarily results in a decrease in the time spent in diastole at a given heart rate. As coronary perfusion occurs primarily during diastole, coronary blood flow decreases. In addition, mean arterial pressure declines as a result of fixed obstruction to left ventricular outflow, which further decreases coronary blood flow. Therefore, increased myocardial oxygen demand and decreased myocardial oxygen supply result in characteristic angina.
Syncope is a consequence of the inability of the heart to increase cardiac output to meet the demands of the body. This can be evident as an exaggerated orthostasis, whereby changing from a sitting to a standing position results in venous pooling of blood, which decreases preload and therefore decreases cardiac output. Normally, heart rate and contractility increase to raise cardiac output and thereby maintain cerebral perfusion until contraction of the venous compartment, and thus restoration of preload, can occur. However, in the setting of significant AS, the fixed outflow obstruction limits the increase in cardiac output, which can result in cerebral hypoperfusion and syncope. Similarly, AS can cause syncope during exertion, as the outflow obstruction limits the increase in cardiac output that is required to compensate for the vasodilation and higher blood flow to exercising skeletal muscle.
Heart failure is a late manifestation of AS and is associated with a poor prognosis. As valvular obstruction worsens, the compensatory left ventricular hypertrophy that develops to normalize wall stress also results in a less compliant ventricle and therefore increases left ventricular end-diastolic pressure. This increased pressure is transmitted to the left atrium, the pulmonary vasculature, and eventually the right side of the heart, and these elevated pressures are clinically manifested as exertional dyspnea. In addition, progressive hypertrophy and severe obstruction to left ventricular outflow can lead to left ventricular systolic dysfunction. Therefore, symptoms of heart failure because of AS may be left-sided, including rest or exertional dyspnea, orthopnea, and paroxysmal nocturnal dyspnea, or right-sided, including anorexia, abdominal swelling, and peripheral edema.
Clinical Assessment
The diagnosis of AS begins with a physical examination. The classic murmur is a crescendo–decrescendo murmur heard best at the right upper sternal border, with a peak that shifts later in systole as the severity of AS increases. This murmur can be differentiated from that of a dynamic outflow tract obstruction (eg, hypertrophic obstructive cardiomyopathy) in that the murmur of AS will soften with Valsalva as the flow across the valve decreases, whereas the murmur of a dynamic outflow tract obstruction will increase as preload decreases. A soft or absent aortic component of the second heart sound (A2) may also be appreciated and is a marker of severity. Furthermore, there may be a delayed and blunted carotid upstroke (
After the physical examination, the next step in the evaluation of AS is a transthoracic echocardiogram. This imaging modality can confirm the diagnosis of AS, help to determine the severity of valvular obstruction, exclude alternative diagnoses, provide information on the etiology, and assess comorbid conditions, including aortic root pathology and aortic insufficiency. Echocardiographic imaging of the stenotic aortic valve almost always shows thickening and calcification of the aortic valve, though this is not specific for any one etiology and rather is more frequently the final common pathologic result. Imaging may show a congenital bicuspid aortic valve or fusion of the commissures to suggest rheumatic AS. A mitral valve with the characteristic “hockey-stick” appearance of rheumatic mitral stenosis combined with AS suggests combined aortic and mitral valve disease as a long-term consequence of rheumatic fever. Echocardiographic assessment of the aortic valve is also important to determine the degree of associated aortic regurgitation, which may complicate management. Furthermore, imaging of the aortic root and ascending aorta may reveal aortic dilatation as may be seen in conjunction with a congenital bicuspid valve.
The severity of AS is typically initially assessed by echocardiographic features.29,30 Complete interrogation of the aortic valve includes assessment of the maximum transvalvular velocity, determination of the mean transvalvular pressure gradient, calculation of the aortic valve area by the continuity equation (ALVOT
When non-invasive assessment of the aortic valve is inconclusive in a symptomatic patient or there is a discrepancy between symptoms and the severity of findings by non-invasive studies, the gold standard is left and right heart catheterization. 30 A right heart catheterization is performed with a balloon-tipped Swan-Ganz catheter, and cardiac output is determined by either thermodilution or the Fick equation. Left heart catheterization is then performed, usually by retrograde catheterization of the left ventricle. The aortic transvalvular gradient is assessed by simultaneous measurement of left ventricular and ascending aortic pressures, either with a single dual-lumen catheter or with two separate catheters. The mean aortic transvalvular gradient is determined and averaged over several beats, and the aortic valve area is calculated by the Gorlin equation 31 :

where AVA is the aortic valve area in cm2, CO is the cardiac output in L/minute,
The single largest confounder of the assessment of AS is concomitant heart failure, which can lead to lower aortic valve velocities and gradients despite severe or critical valvular AS and therefore underestimation of the severity of AS. Suspicion for this “low-flow, low-gradient” (LF–LG) severe AS is raised when an echocardiogram shows a calcified aortic valve with reduced opening, a calculated aortic valve area ≤1.0 cm2 (or ≤0.6 cm2/m2), a mean gradient <40 mmHg or a peak velocity <4.0 m/s, and a left ventricular ejection fraction (LVEF) <50%. 30 In this setting, the question is whether the poor contractile function is a consequence of severe AS, in which case valve replacement is indicated, or if the low gradients and reduced valve area are a consequence of a low-flow state because of other myocardial disease (eg, coronary artery disease, idiopathic cardiomyopathy) in the absence of severe AS, in which case valve replacement is contraindicated. A low-dose dobutamine stress test (2.5-20 mcg/kg/minute), which is done either in the echocardiography laboratory or in the catheterization laboratory, can be helpful to differentiate between LF–LG severe AS and pseudo-severe AS (Class IIa, Level of Evidence B).30,32 Patients with LF–LG severe AS will generally have a mean gradient of ≥40 mmHg, a final aortic valve area of <1.0 cm2, and an increase in aortic valve area of ≤0.3 cm2 with dobutamine stress, whereas those with pseudo-severe stenosis will have an increase in aortic valve area and LVEF with indices of AS failing to meet criteria for severe stenosis. 29 Furthermore, in those patients with LF–LG severe AS, an increase in LVEF or LV stroke volume of ≤20% with dobutamine stress is termed “no flow reserve” or “no contractile reserve.” Such patients have a higher prevalence of concomitant coronary artery disease and a worse prognosis than those with flow reserve. 33
Recently, the phenomenon of LF–LG valvular AS with a preserved LVEF (“paradoxical” LF–LG AS) has been recognized. In this case, “low-flow” is defined by a stroke volume indexed to body surface area of ≤35 mL/m2. 33 Such patients have a smaller LV cavity size and a greater LV relative wall thickness with reduced myocardial contractility. They are more frequently female, older, and have less compliant arterial trees. Furthermore, they have worse survival than similar patients with a preserved LVEF and normal flow.34,35 The “paradoxical” LF–LG setting likely represents an advanced stage of cardiomyopathy and aortic valve disease, and the “paradoxical” nature is likely a consequence of the finding that the LVEF does not necessarily correlate with myocardial contractile function in thickened, small hearts. 33
Several other comorbidities may confound the assessment of AS. 29 Uncontrolled systemic hypertension may alter the LVEF and aortic transvalvular flow; hence, hypertension should be well controlled during the diagnostic study. Concomitant aortic insufficiency is present in about 80% of patients with AS and can lead to higher than expected gradients across the valve because of increased transvalvular flow. In addition, other high-output states (severe anemia, arteriovenous fistula, hemodialysis, and hyperthyroidism) will also increase the flow across the aortic valve and thereby confound measurements of stenosis severity. Finally, underestimation of transvalvular gradients frequently occurs when the ultrasound probe is not parallel to the direction of flow, and can lead to underestimation of the severity of AS.
Management
Medical Therapy
Once established, the rate of progression of AS varies considerably from one patient to the next and is unpredictable. 36 However, it is clear that the vast majority of adverse cardiac events occur in symptomatic patients; hence, the general strategy is one of watchful waiting with serial echocardiograms and clinical visits to assess the development of symptoms related to AS. Therefore, the American Heart Association (AHA) and American College of Cardiology (ACC) guidelines recommend that asymptomatic patients with mild, moderate, and severe AS have a transthoracic echocardiogram every 3-5 years, every 1-2 years, and every 6-12 months, respectively. Furthermore, a repeat echocardiogram is indicated if there is a change in symptoms or physical examination to suggest worsening of stenosis. In addition, exercise stress testing can be performed in the asymptomatic patient with severe AS when the history is unclear to assess exercise-induced symptoms or an abnormal blood pressure response, though is absolutely contraindicated in those with symptomatic severe AS. 30
Severe AS is primarily a mechanical problem (ie, a fixed obstruction to flow), and therefore, definitive management is directed at relief of the obstruction by surgical or transcatheter therapies. Medically managed symptomatic AS has an extremely poor prognosis, with a 5-year mortality of 50-60% and a 10-year mortality approaching 90%.37,38 There are no medical therapies that can slow the progression of AS. Despite the purported role of atherogenesis in the development and progression of calcific AS, statin therapy has not been shown to slow or halt worsening of valvular AS.13,14 However, patients with mild or moderate AS and a depressed LVEF should be treated with standard evidence-based heart failure therapies, which may include angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, and aldosterone receptor antagonists. In addition, patients with mild or moderate AS should have their comorbid conditions, including hypertension, managed appropriately. 30
Owing to the inefficacy of medical therapy in AS, the non-operative management of severe AS is directed at optimizing comorbidities while avoiding medications that will adversely alter hemodynamics. Medications that reduce preload, including nitroglycerin, and that decrease afterload, including ACE inhibitors, ARBs, hydralazine, and non-selective beta-blockers, are contraindicated in severe AS. As the severely stenotic aortic valve limits the compensatory increase in cardiac output, use of these medications can lead to a downward hemodynamic spiral in which decreased preload or afterload results in reduced mean arterial pressure that worsens coronary perfusion. This in turn leads to myocardial ischemia, which results in a decreased cardiac output and therefore a further reduction in mean arterial pressure. Once this spiral is initiated, it can be difficult or impossible to restore the delicate hemodynamic balance, and significant adverse events including death may occur.
Despite this classic teaching, there may be select groups of patients for whom medical therapy can offer some benefit. A recent study prospectively evaluated the effects of sodium nitroprusside on 18 consecutive, symptomatic, LF–LG severe AS patients with hypertension and a preserved LVEF (mean aortic transvalvular pressure <40 mmHg, aortic valve area <1.0 cm2, LVEF >50%, and aortic systolic pressure >140 mmHg) during left and right heart catheterization.
39
Nitroprusside infusion decreased aortic, LV end-diastolic, and pulmonary artery pressures, and led to a statistically significant increase in the mean aortic transvalvular gradient (27 ± 5 to 29 ± 6 mmHg,
In addition, there may be a benefit of intravenous vasodilators in the management of severe AS leading to acute decompensated heart failure (ADHF). Khot et al evaluated the effects of sodium nitroprusside infusion,
40
a potent arterial vasodilator and a common therapy for ADHF in patients without severe AS, in patients in the intensive care unit with a depressed LVEF (≤35%), severe AS (aortic valve area ≤1.0 cm2), and a decreased cardiac index (≤2.2 L/minute/m2) without hypotension (mean arterial pressure <60 mmHg) or a need for intravenous inotropes or vasopressor support. It is well known that relieving the profound vasoconstriction characteristic of ADHF with arterial vasodilators results in improved forward flow and improved systemic hemodynamics, but fears relating to the inability of the heart with severe AS to augment cardiac output to compensate for a decrease in afterload led to this therapy being avoided when severe AS was comorbid. However, Khot et al showed that intravenous nitroprusside resulted in significant improvements in cardiac index (baseline 1.60 ± 0.35 L/minute/m2) in 6 hours (2.22 ± 0.44 L/minute/m2,
Surgical and Transcatheter Therapies
The most simple but least effective of the mechanical treatments for severe AS is balloon aortic valvotomy (BAV). BAV is a transcatheter procedure by which a balloon is passed in a retrograde fashion through a severely stenotic aortic valve. The balloon is positioned within the valve orifice, and subsequent balloon inflation results in a fracturing of the calcific deposits on the aortic valve, improved leaflet mobility, and a modest improvement in aortic valve area, with a concomitant improvement in symptoms. However, the duration of this benefit is generally limited to a few months and the procedure can be associated with complications including stroke, annulus rupture, and vascular access injury.30,41 Therefore, BAV is used for palliation of those patients who cannot have aortic valve replacement because of serious comorbid conditions or as a bridge to definitive aortic valve replacement in patients with severe AS and hemodynamic instability (Class IIb, Level of Evidence C). 30
The only definitive treatment for severe AS is surgical or transcatheter aortic valve replacement (TAVR). In general, aortic valve replacement is indicated in symptomatic patients with severe AS, asymptomatic patients with severe AS who are undergoing cardiac surgery for another reason, and asymptomatic patients with severe AS and an LVEF ≤ 50% (Table 2). Surgical aortic valve replacement (SAVR) remains the gold standard, but TAVR is an increasingly useful and proven treatment in carefully selected patient populations.
ACC/AHA indications for aortic valve replacement in AS (adapted from Nishimura et al. 30 ).

Several types of prosthetic aortic valves are available for surgical implantation, each with their own distinctive advantages and disadvantages. 42 The original aortic valve is excised prior to implantation of the replacement valve, and the replacement is sewn in at the level of the aortic annulus. Of note, most prosthetic aortic valves will have an effective orifice area (EOA) less than that of the native valve because of the space occupied by the structural components of the new valve. Mechanical valves, usually bileaflet or tilting-disk (and until 2007, ball cage), are attractive because of excellent long-term durability and a favorable hemodynamic profile, but require lifelong anticoagulation with warfarin. In contrast, bioprosthetic valves, which consist of three porcine or bovine tissue leaflets mounted on a supporting stent, sacrifice some EOA because of the stent but do not require anticoagulation beyond three months post-operatively. Stentless bioprosthetic valves were developed to increase the EOA, and are especially useful in patients with a small aortic root. Both stented and stentless bioprosthetic valves are less durable than mechanical valves, generally lasting 10-15 years after implantation. Homograft aortic valves are cryopreserved and sterilized cadaveric tissues consisting of the aortic root with the valve in situ, and require excision of the aortic root and re-implantation of the coronary arteries but have a normal EOA. Similar to bioprosthetic valves, homografts do not require long-term anticoagulation. Finally, the Ross procedure, which consists of relocation of the native pulmonary valve into the aortic position, is an option for children and young adults requiring SAVR because of its excellent durability and longevity as well as the lack of need for anticoagulation, but is a much more complicated surgery. The type of aortic valve implanted is tailored to the individual patient based on these and other factors.
SAVR is a definitive and proven therapy for severe AS with a long track record, but requires a sternotomy or thoracotomy and cardiopulmonary bypass. However, SAVR is well tolerated in appropriately selected patients. Most patients undergoing SAVR will spend about a week in the hospital postoperatively, have significant functional recovery within a few months, and experience most of their expected improvement in functional status and overall wellness by about six months, though this can take up to one year. The mortality benefit of SAVR in unselected patients with severe AS is striking, with a three-year survival of 87% in those undergoing SAVR and 12% in those managed medically. 43 Furthermore, patients with any degree of LV systolic dysfunction and severe AS with an acceptable surgical risk benefit from SAVR though have a higher mortality than those with a preserved LVEF. 44 Patients with LF–LG severe AS derive significant mortality benefit from SAVR when compared to medical therapy,33,45,46 though those with flow reserve by dobutamine stress testing have significantly better outcomes than those without reserve. 47 This difference is largely related to a significantly higher operative mortality in those patients with LF–LG severe AS without flow reserve (32-33% vs 5-7%).46,48–50 Finally, patients with “paradoxical” LF–LG severe AS (LVEF ≥50%) benefit from SAVR as well.34,35,51,52
The ability to perform TAVR is a relatively new advance in the treatment of severe AS. Optimal assessment of patients with AS with regard to SAVR or TAVR requires a “heart valve team” approach to determine the appropriate treatment strategy. Heart valve team members often include the patient's primary cardiologist, cardiac imaging specialists, an interventional cardiologist, a cardiac surgeon, nurses, and technologists. 30 TAVR is indicated in patients who meet indications for aortic valve replacement but who have a high or prohibitive surgical risk and an expected post-TAVR survival of greater than one year. 30
The evaluation of a patient with severe AS who may be a candidate for TAVR starts with referral to a heart valve team. The patient then is evaluated by an interventional cardiologist and two cardiac surgeons who come to a consensus regarding surgical risk. Those who have a Society of Thoracic Surgeons (STS) 30 day risk score 53 of ≥10% or comorbidities that are associated with a predicted risk of death of ≥15% in the first 30 days after surgery are considered to be at “high risk,” whereas those with a predicted probability of ≥50% of death or serious irreversible morbidity in the first 30 days after surgery are considered to be at “extreme risk.” Other comorbidities not assessed by the standard STS risk score can also influence surgical risk, including severe ascending aortic calcification (porcelain aorta), liver disease, extreme frailty, chest wall deformities, and prior mediastinal radiation therapy, among others.
If the patient is deemed to be a likely candidate for TAVR, the next step is a contrast-enhanced computed tomography (CT) scan of the chest, abdomen, and pelvis to assess the aortic valve annulus size and potential vascular access, including the diameter of the femoral and iliac arteries. Coronary angiography is performed to determine the presence of obstructive coronary artery disease, with percutaneous coronary intervention performed if indicated. Pulmonary function testing and carotid ultrasound are also frequently performed for operative risk assessment.
The TAVR procedure is performed in a hybrid operating room with flat panel digital imaging capabilities. General anesthesia is often utilized for the procedure but TAVR can also be performed with intravenous sedation as with other invasive procedures in the catheterization laboratory. There are two FDA-approved transcatheter valves available, the Edwards SAPIEN valve (Edwards Lifesciences Corporation, Irvine, CA) and the Medtronic CoreValve (Medtronic, Minneapolis, MN). The Edwards SAPIEN valve is a trileaflet bovine pericardial valve with a stainless steel support frame that is crimped onto a balloon catheter. It requires a 22 or 24 French sheath, depending on the valve size (23 or 26 mm, respectively), and can be inserted via transfemoral, transapical, or direct aortic access. This valve is inserted into the aortic valve annulus, expanded by balloon inflation, and displaces the native aortic valve radially. The Medtronic CoreValve is a trileaflet porcine pericardial valve with a self-expanding nitinol support frame that is implanted by slowly withdrawing a protective sleeve from the collapsed valve. It requires an 18 French delivery sheath, is available in 23, 26, 29, and 31 mm sizes, and can be inserted via transfemoral, subclavian, or direct aortic access. This valve has a much larger supra-annular structure than the Edwards SAPIEN valve, which functions to orient the CoreValve with the aortic root. In addition, while the lower part of the valve sits in the aortic annulus, the valve function is supra-annular, increasing the EOA above that of the Edwards SAPIEN valve or surgical valves. Currently, the Edwards SAPIEN valve is FDA-approved for both high-risk and extreme-risk groups, whereas the CoreValve is FDA-approved for the extreme-risk group.
The efficacy of TAVR in high- and extreme-risk patient groups was first evaluated in the prospective, multicenter, randomized, controlled Placement of Aortic Transcatheter Valves (PARTNER) trial. In the initial study, 358 patients at extreme risk for SAVR were randomized to transfemoral TAVR with the Edwards SAPIEN valve or standard medical therapy, including BAV. At one year, patients in the TAVR arm had a lower rate of death from any cause (30.7 vs 50.7%, hazard ratio [HR] 0.55, 95% confidence interval [CI] 0.40-0.74,
The results of the CoreValve US Pivotal Trial in extreme-risk patients have also been published
56
and led to the recent FDA approval of the CoreValve for this population. In this non-randomized trial, enrolled patients were assigned to TAVR and compared to an “objective performance goal” of an all-cause mortality or major stroke rate of 43%, which was constructed from a meta-analysis of seven BAV studies and the standard medical therapy arm of the extreme-risk PARTNER trial. In all, 489 patients were analyzed in the as-treated iliofemoral population, and at 12 months the composite of all-cause mortality or major stroke occurred in 26.0% (upper two-sided 95% CI 29.9%,
The PARTNER trial also studied TAVR with the Edwards SAPIEN valve compared to SAVR in high-risk patients. A total of 699 patients at 25 centers were randomized to TAVR via a transfemoral or transapical approach and SAVR. There was a trend toward decreased all-cause mortality in the TAVR arm at 30 days (3.4 vs 6.5%,
Similarly, a recent study compared TAVR with the CoreValve to SAVR in 795 high-risk patients with severe AS.
60
In the as-treated analysis of 747 patients, the primary endpoint of all-cause mortality at one year was met in 14.2% of patients in the TAVR group and 19.1% of patients in the SAVR group (
In summary, the current evidence shows that TAVR improves all-cause mortality, cardiac death, and symptoms in patients who are at extreme risk for SAVR, though at the cost of a non-negligible increase in strokes as well as a significant risk of major vascular complications. Furthermore, while TAVR with the Edwards SAPIEN valve in extreme-risk patients results in an absolute decrease in all-cause mortality of 24.7% at two years, the TAVR group still had an absolute all-cause mortality rate of 43.3%. This serves as a reminder of the very poor prognosis of some extreme-risk patients regardless of treatment, and suggests that further refinement of the patient population that stands to benefit from TAVR is necessary. Conversely, in high-risk patients, TAVR with the Edwards Sapien valve is non-inferior to SAVR and TAVR with the Medtronic CoreValve is superior to SAVR with regard to all-cause mortality. However, TAVR with either device comes with an increased risk of major vascular complications while SAVR is associated with an increased risk of major bleeding and new-onset atrial fibrillation. At this time, there is no evidence to support the use of TAVR in patients at less than high risk for SAVR although clinical trials of intermediate risk patients (STS risk score of 4-10%) are currently underway in the United States. Furthermore, patients with bicuspid and non-calcified aortic valves have been excluded from all of the major TAVR trials, and therefore outcomes in such patients remain to be investigated. Finally, research is ongoing to assess TAVR use in other high- to extreme-risk cohorts, including those with prior SAVR (TAV-in-SAV), end-stage renal disease, LF–LG severe AS, and severe concomitant mitral or tricuspid pathology.
Future Directions
To this point, there has only been one randomized, direct comparison between the Edwards SAPIEN valve and the Medtronic CoreValve. The Comparison of Transcatheter Heart Valves in High Risk Patients with Severe Aortic Stenosis: Medtronic CoreValve vs Edwards SAPIEN XT (CHOICE) trial showed a higher rate of device success with the SAPIEN XT compared to the CoreValve, but this outcome was driven largely by angiographically assessed aortic insufficiency at the conclusion of the procedure. 61 There are several problems with the way this outcome was assessed; hence, the CHOICE trial is far from definitive. Therefore, direct, randomized comparisons between transcatheter valves are needed.
Several clinical trials of new transcatheter aortic valves, including second- and third-generation Edwards valves, a second-generation Medtronic CoreValve, the Portico valve (St. Jude Medical, Minneapolis, MN), and the Lotus valve (Boston Scientific, Natick, MA), are either currently enrolling or will begin enrollment soon. These valves incorporate features including reduced delivery catheter diameter, anticalcification leaflet treatment, and improved repositioning capabilities, and thereby hope to improve on the safety, efficacy, and durability of TAVR.
Author Contributions
Conceived the concept: MJC, JRR. Wrote the first draft of the manuscript: MJC. Contributed to the writing of the manuscript: JRR. Agree with manuscript results and conclusions: MJC, JRR. Jointly developed the structure and arguments for the paper: MJC, JRR. Made critical revisions and approved final version: MJC, JRR. Both authors reviewed and approved of the final manuscript.