
Abstract
Methamphetamine has become a drug of widespread use in young abusers in Iran. It may induce hypertension, vasospasm, and direct vascular toxicity. Harmful consequences are common, including cardiac and cerebrovascular accidents. This is a report of a 37-year-old man with a 3-year history of drug use that presented to the emergency department within 30 min of the onset of syncope followed by speech difficulty and right-sided weakness. The patient had an extensive ischemic stroke because of left ventricular apical thrombus without any other significant risk factors such as hypertension, alcohol abuse, or ischemic heart disease.
Case Report
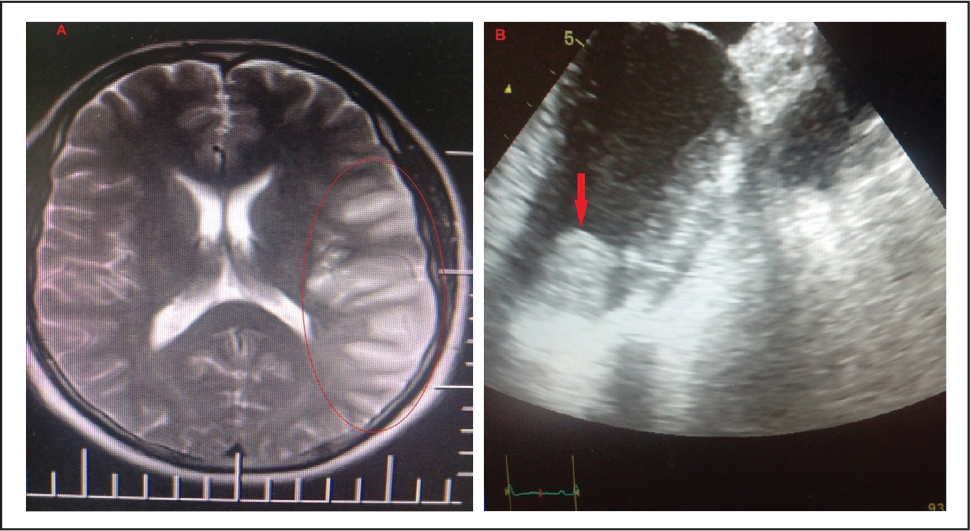
A 37-year-old male with a history of methamphetamine (MA) abuse presented with acute onset syncope, speech difficulty, and right-sided weakness. The patient’s history was taken from his wife because he was unable to speak. The patient snorted MA for 3 years. He had no major cardiovascular risk factors except for 3 pack-years of smoking. His family history was unremarkable for cardiovascular diseases. Physical exam revealed Broca’s aphasia, right facial palsy, and ipsilateral hemiplegia. He suffered from a major and immediate impairment of cognitive domains with retrograde memory being the most impaired. On admission, his blood pressure was 100/60 mmHg, the heart rate was 90 beats/min, the respiratory rate was 18 breaths/min, and his body temperature was 36.5° C. Cardiovascular, respiratory, and abdominal examinations were normal. His electrolytes, liver function, renal function, and troponin level were normal. The urine toxicology screen was positive for MA. An electrocardiogram showed a normal sinus rhythm, nonspecific ST segment, and T wave changes in precordial leads. Magnetic resonance diffusion weighted image showed extensive ischemia of the territory supplied by the left middle cerebral artery (Figure 1[A]). Treatment was started with heparin drip. On day 2 of admission, a transthoracic echocardiogram showed a hypoechoic and hypermobile mass of about 24 × 18 mm in size in the apex of the left ventricle, consistent with a left ventricular thrombus (Figure 1[B]). The ejection fraction was estimated to be 30% with grade 2 diastolic dysfunction. There was mild mitral and tricuspid regurgitation with a normal valve structure. He had a normal coronary angiogram. Several days after admission, despite being medically stable, his short-term memory remained impaired, and he had difficulty recalling any recent events and visitors since his admission. He had some insight into his own short-term memory loss. Treatment was initiated for heart failure including carvedilol and furosemide. Following 3 weeks of pharmacotherapy, the patient was discharged from the hospital on warfarin, carvedilol, and furosemide. He returned to work within 10 months. Outpatient follow-up visits were scheduled at 1, 2, 3, 6, 12, and 16 months. He recovered with only a mild expressive aphasia and mild right-hand weakness within 6 months. Clinical improvements were noted during all follow-up visits. He fully recovered after 12 months.
(A) Brain Imaging Study Showing Extensive Ischemia of the Left Frontotemporal Area (B) A Thrombus Visible at the Apex of the Left Ventricle (Pointed by Red Arrow)
Discussion
MA use is a major public health concern in Iran. An estimated 34.2 million people worldwide or 0.7% of the population aged 15 to 64 years have used MAs in the past 1 year. 1 MA, also known as crank, ice, crystal meth, speed, and glass, is a highly addictive stimulant that can be smoked, snorted, swallowed, or injected. Two aspects need to be discussed in this case: left ventricle thrombus formation and ischemic stroke. MAs can cause vasoconstriction and spasm, increase blood pressure, induce arrhythmia, and cause cardiomyopathy. The pathophysiology of MA cardiotoxicity is not fully understood, but it is thought to be mediated by catecholamine-induced myocarditis followed by myocardial fibrosis 2 and scar formation. 3 Cardiovascular complications are the second leading cause of death in MA users (14%) after drug toxicity. 4 MA users consistently have a higher severity of the disease compared to controls with non-MA cardiomyopathy. 5 A left ventricular thrombus may complicate left ventricular systolic function and lead to thromboembolic events such as stroke. Cardiac function improves significantly after discontinuing the MA use when combined with appropriate medical treatment. Our patient received anticoagulation and heart failure therapy, and follow-up imaging showed resolution of the thrombus and improvement of the left ventricular function after 12 months. The physician should be aware for cardiac complications of MA use and look for left ventricular thrombi in patients with cerebrovascular accidents. Acute stroke is a medical emergency. Ischemic stroke represents the loss of brain function caused by a decreased blood flow and consequently reduced oxygen supply to the affected brain tissue. 6 Both ischemic and hemorrhagic stroke have been reported because of MA abuse. MA use leads to ischemic stroke through stimulating the sympathetic nervous system causing vasoconstriction. The most commonly reported vascular complication of MA abuse is cerebrovascular hemorrhage. 7 Hemorrhagic strokes may also occur as a result of vessel wall rupture. 7 Intracardiac thrombi are reported in up to 33% of MA abusers, which can also lead to coronary occlusions.8, 9 Patient would be presented with peripheral vascular thrombus. 10 Our patient had an ischemic stroke because of cardiomyopathy and an apical thrombus without any other significant risk factors such as hypertension or ischemic heart disease.
Conclusion
This was a report of a patient suffering from a thromboembolic stroke, LV thrombus, and LV dysfunction (EF < 30%) in the setting of MA abuse. Drug abuse represents a major social and public health problem and is a risk factor for ischemic stroke. Drug abstinence is the mainstay of therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.