
Abstract
Dilated cardiomyopathy (DCM) is increasingly indicated as a cause of cardioembolic syndrome, in particular, cardioembolic ischemia stroke. However, the potential risk factors for stroke among DCM patients remain under investigated. DCM patients hospitalized from June 2011 to June 2016 were included. The cases were defined as the group of DCM patients with stroke compared with those without stroke. Clinical characteristic data were collected and compared between the two groups including demographic data, complicated diseases, echocardiography index, and laboratory parameters and estimated glomerular filtration rate (eGFR). A multivariate logistic regression analysis model adjusted by sex and age was used to explore the related risk factors for stroke in DCM patients. A total of 779 hospitalized patients with DCM were included. Of these, 55 (7.1%) had experienced a stroke. Significantly lower eGFR levels (68.03 ± 26.22 vs 79.88 ± 24.25 mL/min/1.73 m2, P = .001) and larger left atrial diameters (45.32 ± 7.79 vs 43.25 ± 7.11 mm, P = .04) were found in the group of patients having DCM with stroke compared to those without stroke. When the eGFR was categorized as eGFR >60, 30<eGFR≤ 60 and eGFR ≤ 30, there were more patients with 30<eGFR≤ 60 (30.9% vs 17.7%) and eGFR≤ 30 (9.1% vs 3.3%) in the ischemic stroke group (P = 0.003). A multivariate logistic regression analysis model adjusted by sex and age showed that 30 <eGFR≤60 (odds ratio [OR]: 2.07, 95% confidence interval [CI]: [1.05-4.07], P = .035) and eGFR≤30 (OR: 4.04, 95% CI: [1.41-11.62], P = .009) were statistically associated with ischemic stroke in patients with DCM. It is concluded that decreased eGFR is significantly associated with an increased risk of ischemic stroke in patients with DCM.
Introduction
Ischemic stroke events related to cardiovascular disease usually result from cardioembolism of the large cerebral artery and tend to be more frequently fatal or associated with more serious disability than strokes from other causes. Recently, several case reports demonstrated that patients with dilated cardiomyopathy (DCM) developed cardiogenic cerebral infarction. 1 –3 Increasing attention has been focused on the pathogenesis of thrombosis among these patients. One explanation might be that atrial fibrillation (AF) is a complication of DCM, which is a known risk factor for ischemic stroke. 4 The other possibility is that patients with DCM are susceptible to left ventricular thrombosis due to blood clots caused by myocardial systolic dysfunction. It has been reported that the prevalence of left ventricular thrombosis in patients with DCM is 11% to 44%. 5
Investigations have been limited in DCM cohorts to identify the clinical characteristics of patients with DCM diagnosed with ischemic stroke and the potential risk factors for ischemic stroke. Chronic kidney dysfunction has been previously identified as an independent risk factor for ischemic stroke in patients with AF, and the R2CHA2DS2-VASc score has been developed as a modified scoring system to evaluate the risk of systemic embolism and stroke in patients with AF. 6 Low estimated glomerular filtration rate (eGFR) is also associated with intracranial arterial stenosis. 7 Additionally, among patients with hypertrophic cardiomyopathy (HCM), several risk factors for ischemic stroke have been reported, including elderly age, maximal left ventricular wall thickness, left atrial size, and complications including AF, heart failure, or vascular disease. 8
However, eGFR levels have not yet been described in patients having DCM with stroke. It is not clear whether patients having DCM with decreased eGFR have increased risk of ischemic stroke. The present study was performed to collect clinical characteristics of hospitalized patients with DCM and to explore whether eGFR is associated with the risk of ischemic stroke among these patients.
Patients and Methods
Study Population
This study protocol was approved by the ethics committee of the Second Affiliated Hospital of Nanchang University. Informed consents were obtained from all patients. A total of 2425 patients diagnosed with DCM were consecutively hospitalized in the second Affiliated Hospital of Nanchang University from June 2011 to June 2016. Patients who met the following criteria were eligible: (1) Diagnosis was made according to the guidelines for the management of DCM, 9 which is characterized by left ventricular ejection fraction (LVEF) ≤45% or left ventricular short axis reduction (LVSF) <25%, with left ventricular diastolic dimension (LVDd) > 55 mm in the echocardiograms. (2) Patients were excluded if they had the following complications: ischemic cardiomyopathy, arrhythmogenic cardiomyopathy, rheumatic heart disease, congenital heart disease, pulmonary heart disease, drug-induced cardiomyopathy, and perinatal cardiomyopathy. For patients with recurrent admission, only data during the first hospitalization were collected for analysis. Two experienced cardiologists individually reviewed each patient’s medical records to confirm study eligibility.
Clinical Data Extraction
All clinical patient data were extracted from medical records in our hospital information system, including demographic data, complicated diseases, echocardiography index, and laboratory parameters. Patients were considered to have had ischemic stroke if cerebral infarction, lacunar infarction, or transient ischemic attack was included in their medical records. These could be previous conditions or newly diagnosed during hospitalization. The eGFR was calculated using the new Chronic Kidney Disease Epidemiology Collaboration equation: eGFR = a × (serum creatinine/b)c × 0.993 age. All clinical data were measured on admission. Patients were divided into 2 groups, those with and those without stroke.
Statistical Analysis
For the statistical analyses, all continuous data were represented by the mean ± standard deviation. The comparison of continuous data between 2 groups was performed by Student t tests. Categorical variables are presented as n (%) and were analyzed using the χ2 test. Univariate and logistic regression analyses were used to analyze the related factors of DCM combined with ischemic stroke. After performing the univariate regression analyses, variables with a P value <.05 or potential clinic significance were selected as candidates for entry into the multivariate model. All data were collected and tabulated using Microsoft Excel (Microsoft Inc, California) in a database format. Statistical analyses were performed using IBM SPSS Version 23.0 (IBM Inc, Chicago, Illinois). Two-sided P values < .05 were considered to be statistically significant.
Results
Among 2425 hospitalized patients with DCM, 779 patients were eligible and reviewed in this study. Of these, 55 (7.1%) patients had a diagnosis of ischemic stroke.
Clinical Characteristics
As shown in Table 1, there was no significant difference between the 2 groups among a series of variables including age, sex, homocysteine, and the incidence of combined diseases such as hypertension, diabetes, or AF.
Comparison of Clinical Characteristic Data Between Patients Having Atrial Fibrillation With and Without Stroke.

Abbreviations: EF, ejection fraction; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; LAD, left atrial diameter; LVEDD, left ventricular end-diastolic diameter; LVESD, left ventricular end-systolic diameter; LVSF, left ventricular fractional shortening; RAD, right atrial diameter; RSD, right ventricular diameter.
a Statistical difference was observed between the 2 groups.
Compared to patients having DCM without stoke, the measurement of left atrial diameter (LAD) was statistically larger in those with stroke (45.32 ± 7.79 vs 43.25 ± 7.11 mm, P = .04). Despite no significant difference in serum creatinine, statistically lower eGFR was observed in patients having DCM with stroke (68.03 ± 26.22 vs 79.88± 24.25 mL/min/1.73 m2, P = .001). When the eGFR was categorized as eGFR > 60, 30 < eGFR ≤ 60, and eGFR ≤30, there were more patients with 30 <eGFR ≤ 60 (30.9% vs 17.7%) and eGFR ≤30 (9.1% vs 3.3%) in the ischemic stroke group (P = .003) as shown in Figure 1.

The proportion of patients with or without stroke among 3 estimated glomerular filtration rate (eGFR) categories.
Multivariate Analysis on Risk Factors for Ischemic Stroke
Variables included sex, age, LAD, eGFR, hypertension, diabetes, and AF. For categorized eGFR, eGFR >60 was considered the reference. On multivariate regression analysis, 30 <eGFR≤60 (odds ratio [OR]: 2.07, 95% confidence interval [CI]: [1.05-4.07], P = .035) and eGFR≤30 (OR: 4.04, 95% CI: [1.41-11.62], P = .009) were statistically associated with ischemic stroke in patients with DCM, as shown in Table 2.
Multivariate Analysis of Factors Related to DCM Combined With Ischemic Stroke.
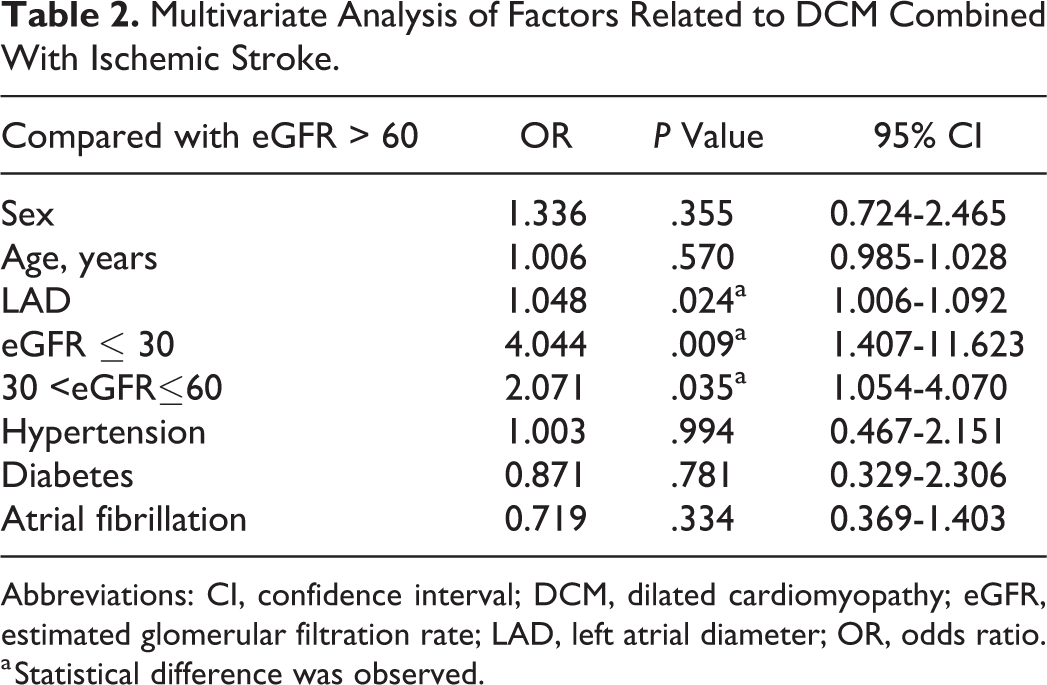
Abbreviations: CI, confidence interval; DCM, dilated cardiomyopathy; eGFR, estimated glomerular filtration rate; LAD, left atrial diameter; OR, odds ratio.
a Statistical difference was observed.
Discussion
Previous studies have indicated that patients with DCM are susceptible to cardiogenic cerebral infarction. 10,11 In this study, we presented the clinical characteristics of patients having DCM, with or without ischemic stroke. Our findings first indicated reduced eGFR levels were closely associated with an increased rate of ischemic stroke among patients with DCM.
The pathogenesis of thromboembolic events in patients with DCM is multifactorial. The risk of thromboembolic complications presenting in idiopathic DCM might be related to blood stasis and altered myocardial kinetics, which might be associated with an enlarged ventricle, subdued ventricular wall motion, decreased cardiac output, arrhythmia, and a higher level of platelet activity. 10,12,13 These pathophysiological substrates may place patients with DCM at high risk of embolic events.
Well-known risk factors for ischemic stroke include smoking, alcohol consumption, age, sex, hyperlipidemia, abnormal glucose metabolism, hypertension, AF, heart valve disease, ischemic heart disease, carotid atherosclerosis, and hyperhomocysteinemia. 14 –17 In this study, 55 (7.1%) hospitalized patients with DCM had experienced ischemic stroke. By comparing the clinical characteristic data of the 55 patients with stroke and the 724 patients without stroke, no significant difference was found between the 2 groups for a series of variables, including age, sex, serum creatinine, hypertension, diabetes mellitus, AF, right atrial diameter, left ventricular diameter, and homocysteine. However, larger LAD was more prevalent in patients having DCM with stroke than in those without stroke, which is similar to the findings that LAD is a risk factor for thromboembolic events in patients with HCM. 8
It has been previously demonstrated that left atrial enlargement is an independent predictor of cardiovascular events in patients with chronic kidney disease. 18 In our study, despite there being no significant difference in LVEF, larger LAD and reduced eGFR can be observed in the ischemic stroke group. The causal link between LAD and eGFR remains uncertain. Both LA enlargement and reduced eGFR might be consequential for increased activation of the renin–angiotensin–aldosterone pathway, leading to high risk of ischemic stroke from damage to the vascular endothelia.
The presence of thrombus, as interpreted by echocardiograms, has been reported to be associated with a 3-fold increased risk of stroke or TIA among patients with DCM. 10 However, it remains under investigation whether renal function is related to the increased risk of ischemic stroke in this population. Our findings illustrated that eGFR level was significantly lower in patients with DCM having ischemic stroke. When patients were classified into 3 subgroups based on eGFR >60, 30< eGFR ≤60, and eGFR <30, there were more patients diagnosed with stroke in the latter 2 subgroups. Additional multivariate logistic analysis determined that approximately 2-fold and 4-fold incidence of stroke can be found in patients having DCM with 30 < eGFR ≤60 and eGFR ≤30, respectively.
As shown in previous studies, abnormal eGFR levels (eGFR ≤ 60) are an independent risk of the first occurrence of stroke in the general population, particularly in patients with AF. 19 A recent epidemiological investigation has found that, by 2013, cardiovascular deaths attributed to reduced GFR outnumbered deaths related to end-stage renal disease worldwide. 20 Although our findings cannot demonstrate that low eGFR levels are risk factors for DCM with ischemic stroke, we conclude that patients having DCM with ischemic stroke may be associated with low levels of eGFR. The underlying mechanism needs to be further investigated. We hypothesize that reduced eGFR in patients with DCM can promote the formation of thrombosis through excessive oxidative stress on the vascular endothelium and activating the renin–angiotensin system. 21,22
The present study found that 7.1% of patients with DCM had a diagnosis of ischemic stroke. This might be an underestimate due to the absence of magnetic resonance imaging or computed tomography (CT) examination of patients with asymptomatic stroke. As reported previously, silent cerebral infarction can be found in patients with DCM. 23 Thus, it is suggested that patients having DCM with abnormal eGFR be routinely evaluated by magnetic resonance imaging or CT examination to screen the silent ischemic stroke.
The risk of ischemic stroke in patients with AF has been demonstrated in detail previously, and stroke prevention with anticoagulation therapy is clearly recommended. 24 However, there is limited evidence for the use of anticoagulation therapy to prevent stroke events among patients with DCM having sinus rhythm. The present study has shown that reduced eGFR and larger LAD are possibly associated with increased incidence of ischemic stroke in patients with DCM. Therefore, we hypothesize that patients having DCM with reduced eGFR and increased LAD might benefit from anticoagulation therapy to prevent stroke events. A large-scale prospective trial is warranted to provide robust evidence for this hypothesis. Clinicians should be careful to identify patients having DCM with high risk of ischemic stroke and treat them appropriately.
Limitations
This is a retrospective cohort study with several inherent limitations. First, since the study population was drawn from a single center, relative selection biases may be introduced. The relation between abnormal eGFR and the risk of ischemic stroke might be overestimated. Second, cranial MRI or CT cannot be measured in every patient with DCM. The incidence of ischemic stroke might be underestimated since some patients with silent ischemic stroke cannot be detected. Finally, the sample size was relatively small for a multivariable regression analysis. Since patients having DCM with abnormal eGFR are at high risk of ischemic stroke, it remains uncertain whether it is reasonable to prescribe oral anticoagulants to patients having DCM without AF. Studies with very large sample sizes are needed to provide further evidence for the use of anticoagulant therapy in patients with DCM to prevent ischemic stroke.
Footnotes
Authors’ Note
Yuqing Deng and Zhiqing Chen are contributed equally to this work. HK conceived and designed the study. Acquisition and analysis of data were performed by DYQ, CZQ, HLL, XZY, HJZ, MJY, and YJH. DYQ and XQM drafted the manuscript. HK, XQM, HJX, and LJX reviewed and edited this article. The final approval of the version to be submitted was confirmed by all the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [grant number 81530013 and 81600243], National Key Research and Development Foundation [grant number 2017YFC1307804] and Natural Science Foundation of Jiangxi[grant number 210171ACB20033 and 2161BAB215238].