
Abstract
The left main coronary artery (LMCA) supplies majority of the left ventricular myocardium and atherosclerotic obstruction is associated with significant myocardial jeopardy. Coronary artery bypass surgery (CABG) has been the gold standard for LMCA disease in the past. The LMCA has special characteristics anatomically, poses different challenges with regard to percutaneous coronary intervention (PCI), and is often associated with multivessel disease. However, advancements in technology have established PCI to be a standard, safe, and reasonable alternative to CABG with comparable outcomes. Contemporary PCI of LMCA disease includes proper selection of the patients and correct technique, and is aided by intravascular ultrasound, optical coherence tomography, and physiological assessment with fractional flow reserve. In this review article, we discuss the anatomy, plaque characteristics of LMCA, current evidence from registries and randomized trials comparing with CABG, technical aspects of stent implantation, adjuvant technologies, mechanical circulatory supports, and triumph of PCI.
Keywords
Introduction
The left main coronary artery (LMCA) usually arises from the left coronary sinus, bifurcates into the left anterior descending (LAD) artery and left circumflex artery (LCX) in a majority of individuals, and trifurcates into an additional ramus intermedius (RI) in few. 1 The left main disease most commonly occurs due to atherosclerosis, whereas other less common causes include vasospasm, arteritis, radiation, extrinsic compression, and so on. 2 Significant LMCA stenosis is defined as a >50% diameter stenosis, and the left main equivalent disease is defined severe (³70%) diameter stenosis of the proximal LAD and proximal left circumflex as judged by contrast angiography. Unprotected LMCA disease is defined as significant stenosis in the LMCA and there were no previous CABG or patent bypass grafts to the LAD or LCX arteries. The LMCA disease (i.e., > 50% stenosis) was found in 1477 (7.3%) of 20 137 patients in the Coronary Artery Surgery Study (CASS) registry. 3 In this registry, survival significantly improved with surgery compared with medical management in patients with asymptomatic LMCA disease, thus indicating CABG for all patients with >50% stenosis regardless of symptom status. However, percutaneous treatment of LMCA stenosis is made possible with the advances in interventional cardiology. The present review aims to address different techniques, trials, and the recent controversies regarding CABG versus PCI of LMCA disease.
Anatomy and Plaque Characteristics
The LMCA is divided into ostium, trunk, and bifurcation 4 (Figure 1). The distribution of LMCA lesions is approximately 1% ostial, predominantly occurring in young women, about two-thirds in the distal left main artery and remainder in the shaft. In >80% of the cases, it is associated with atherosclerosis in other vessels. The LMCA contains a higher elastic tissue component compared to the rest of the coronary tree 5 and when bifurcation is involved the carina is spared. The ostium of the LMCA lacks the tunica adventitia and is richer in smooth muscle cells and elastic tissue than any other portion of the LMCA and its branches. 6 In a study by Oviedo, it was found that continuous plaque from the LMCA into the proximal LAD artery was seen in 90%, from the LMCA into the LCX artery in 66.4% and from the LMCA into both the LAD and LCX arteries in 62%. Plaque localized to either LAD or LCX ostium and not involving distal LMCA was seen in only 9.3% of LAD arteries and 17.1% of LCX arteries. 7
LMCA Ostial, Shaft, and Distal Lesions
The left main disease is an interesting subset not only because of the above characteristics, but also because of the heterogeneity in survival. It is established from the survival studies that three-year survival in medically treated patients with >50% stenosis is 50%. 8 While these studies antedate current advanced pharmacotherapy, such as beta blockers, statins, antiplatelet therapies which might be associated with better outcomes, current guidelines recommend revascularization for > 50% LM stenosis. 9
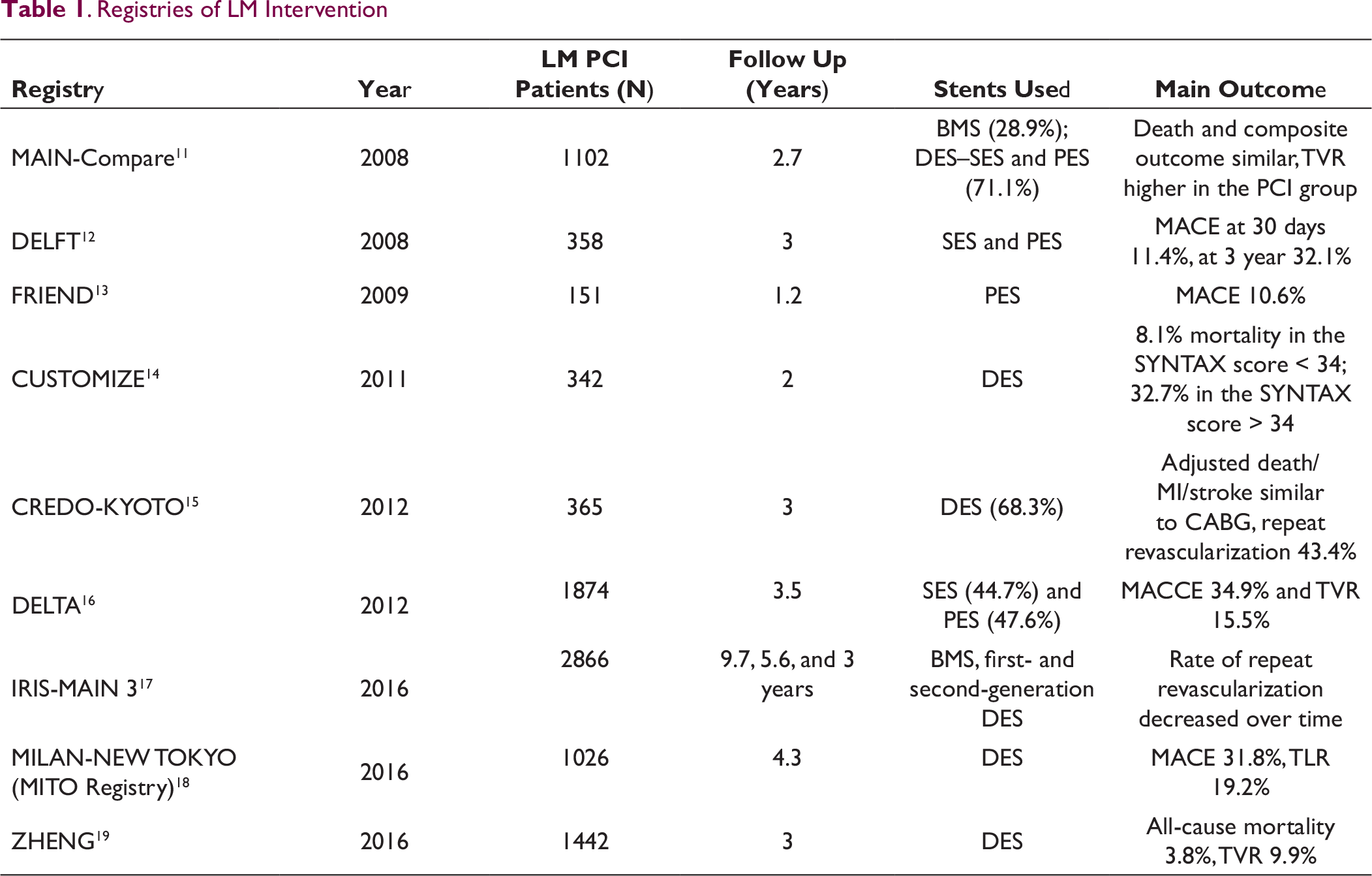
. Registries of LM Intervention
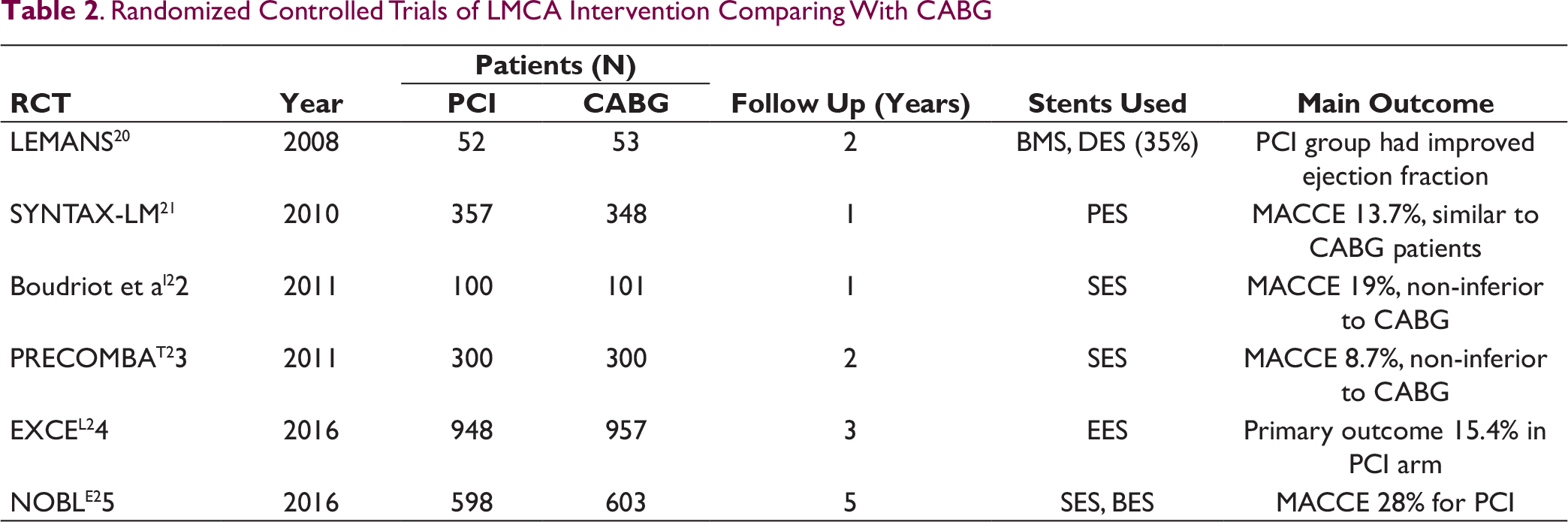
. Randomized Controlled Trials of LMCA Intervention Comparing With CABG
Trial Evidence for LM Stenting
Initial experience with LM stenting in the form of case reports and registries (Table 1) has paved way for randomized trials comparing LMCA interventions to CABG (Table 2). Data from registries are heterogeneous with variable demographics, differing stent usage, deployment techniques and different outcomes. Nevertheless, these data have provided an insight into the safety and feasibility of intervention for LMCA disease and demonstrated it to be comparable to the results of CABG.
At present, combined data from the above six trials of 2355 patients randomized to LM PCI and 2362 patients randomized to CABG suggest non-inferiority of PCI with regard to survival. However, higher repeat revascularizations in the PCI group remain a concern when compared to CABG. It may be concluded that PCI works best for Ostial and shaft lesions and in patients with SYNTAX score < 33. In LM bifurcations, and in those with SYNTAX score > 33, CABG may be preferred although an individualized approach may be prudent. Several randomized and large observational studies are ongoing to further clarify the safety and efficacy of LMCA intervention. 26
Technical Considerations in LM Stenting
When performing LMCA interventions, the following technical considerations are important.
Assessment of LM Disease
Traditionally and in most centers in our country, angiography is the modality to assess the LM stenosis, which is highly reproducible and accurate when the stenosis is ≥70%. However, in intermediate stenoses (30–70%), it is associated with significant inter-observer variability. In such lesions, further detailed assessment of anatomic severity and hemodynamic significance of the lesions is obtained by intracoronary imaging with intravascular ultrasound (IVUS), optical coherence tomography (OCT), or by using fractional flow reserve (FFR).
Role of Coronary Imaging for LM Stenting
In view of the forgoing discussion, it becomes important, rather mandatory to perform imaging studies in LMCA intervention. LMCA imaging is performed to assess the significance of the LM lesion, thus establishing the need for intervention, to measure the vessel diameter, to understand plaque morphology thereby assessing the need for debulking, to determine the extent of the atherosclerosis—whether distal bifurcation and ostia of LAD and LCX are involved—and finally to optimize the stent expansion and identify complications such as dissections, thrombus, and intracoronary hematomas.
The results from the multicenter LITRO study indicated that LMCA intervention may be safely deferred if the minimal lumen area by IVUS is > 6 mm2. In this study comprising of 354 patients, LMCA intervention was deferred in 179 of 186 patients and undertaken 152 of 168 patients based on the minimal lumen area cut-off value of 6 mm2. During 2-year follow-up, no difference was observed with regard to cardiac death or events. 27 It is important to perform IVUS pull back from LAD and LCX into LMCA to assess the plaque burden at the ostia of these branches and also to disengage the guide catheter to assess the plaque burden at LM ostium. An MLA < 3.7 mm2 or plaque burden > 56% in the LCX ostium is a predictor of the need for a second stent after provisional stenting of the main vessel and LM ostium should be stented if the plaque burden is > 50% at the ostium. Further IVUS also helps to assess the degree and depth of calcification and guides to decide for debulking strategy such as rotablation.
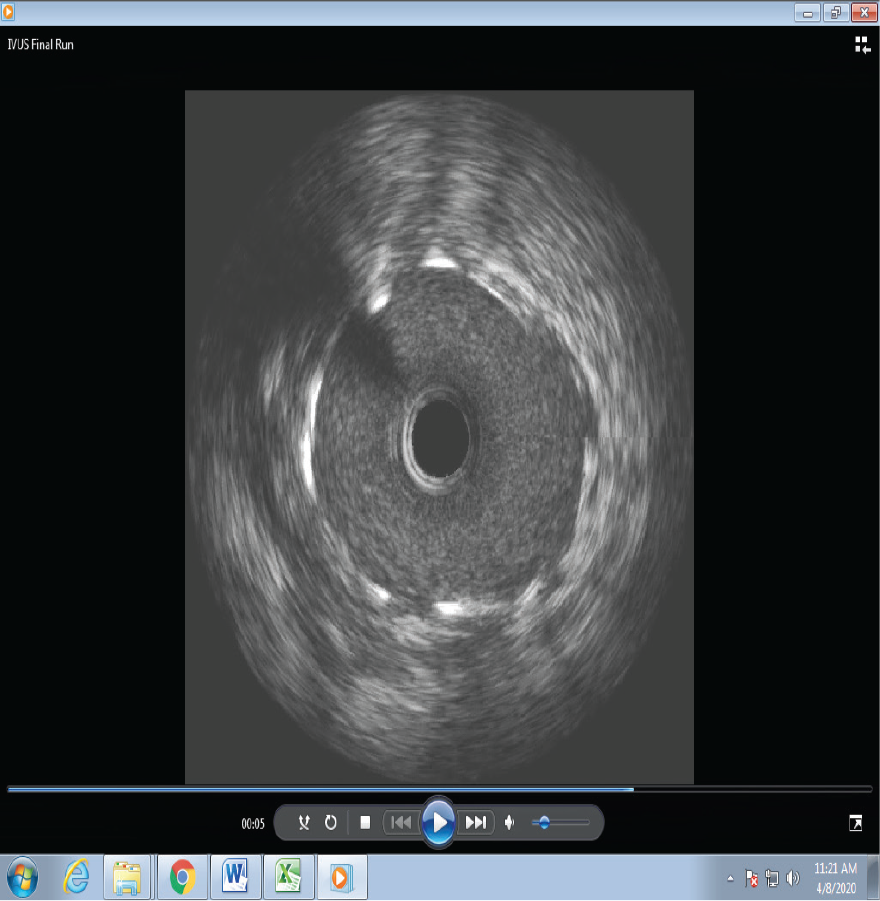
Poststent IVUS run will help to detect stent under expansion and mal apposition (Figure 2). Poststent minimal stent area to predict angiographic restenosis have been proposed by Kang et al., which include 5.0 mm2 for the LCX ostium, 6.3 mm2 for the LAD ostium, 7.2 mm2 for the polygon of confluence, and 8.2 mm2 for the proximal LM above the polygon of confluence. 28
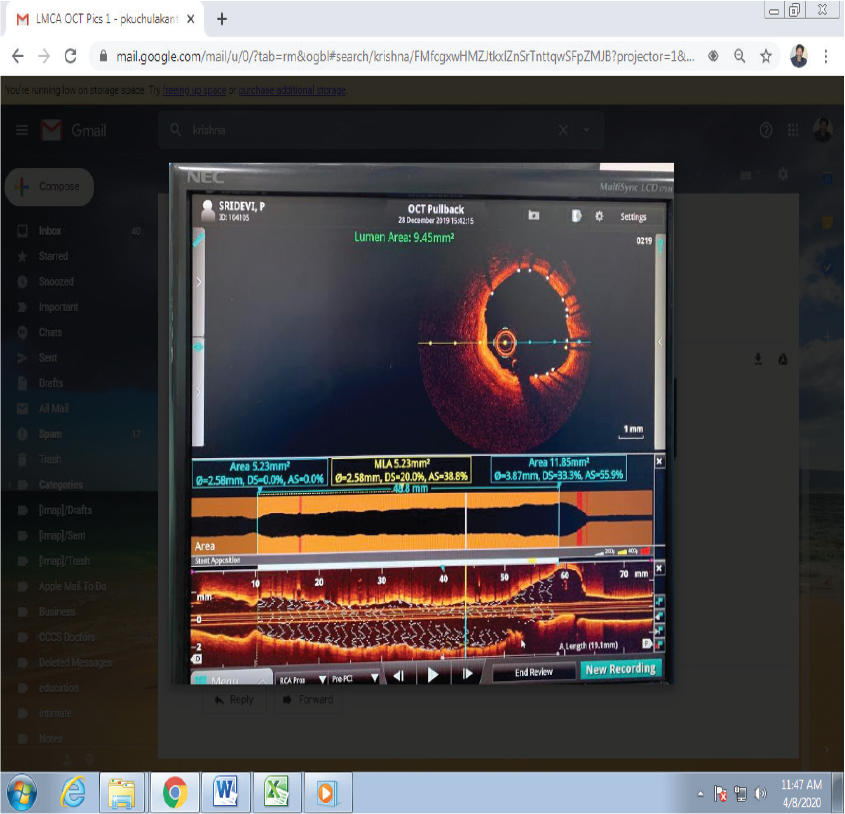
Optical coherence tomography (OCT) is the newer imaging modality with higher resolution and faster pull back speed to assess the intravascular characteristics of the vessel and plaque. OCT is especially useful to identify stent under expansion and malapposition with more precision compared to IVUS. An example of OCT post-LM stent is shown in Figure 3. Although at present no guideline recommendations are available for OCT-derived LM for intervention, Dato et al have published their experience in 133 patients with LM bifurcation using LM area stenosis ≥ 75% and LM area stenosis between 50 and 75% with the minimum lumen area < 4 mm2 or plaque ulceration. The authors have reported no difference in target vessel failure between conservative (n = 58) and stent group (n = 48) at 18 months follow-up. 29
Intravascular Ultrasound Showing Excellent Stent Expansion
OCT after LM Stent Showing Good Apposition and Stent Area
Role of FFR in LM Stenting
Measurement of fractional flow reserve is an important adjunct in the decision making of LMCA intermediate stenosis. Medical therapy for LMCA guided by the FFR value of > 0.80 has been shown to be safe over a 5-year follow-up compared to those subjected for CABG when the FFR values were < 0.80. 30 When LMCA FFR is between 0.08 and 0.85, additional IVUS interrogation may be used to decide for intervention. In the case of bifurcation LM disease, FFR pullback should be done across both LAD and LCX branches. It should be borne in mind that stenosis of LAD or LCX will increase the FFR value in LMCA. In such a situation, re-assessment of LM FFR should be done after stenting of LAD or LCX lesions. FFR assessment is also very useful to avoid stenting of jailed LCX branch after stenting across LAD.
Strategies for LM Stenting
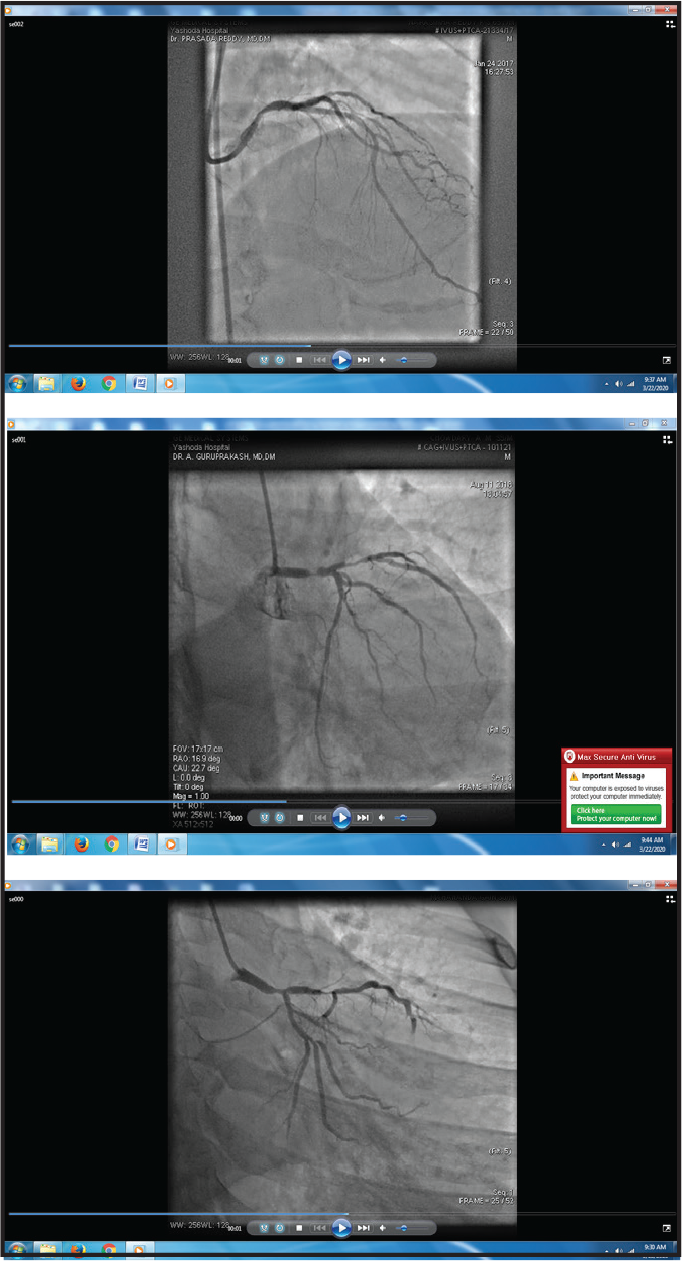
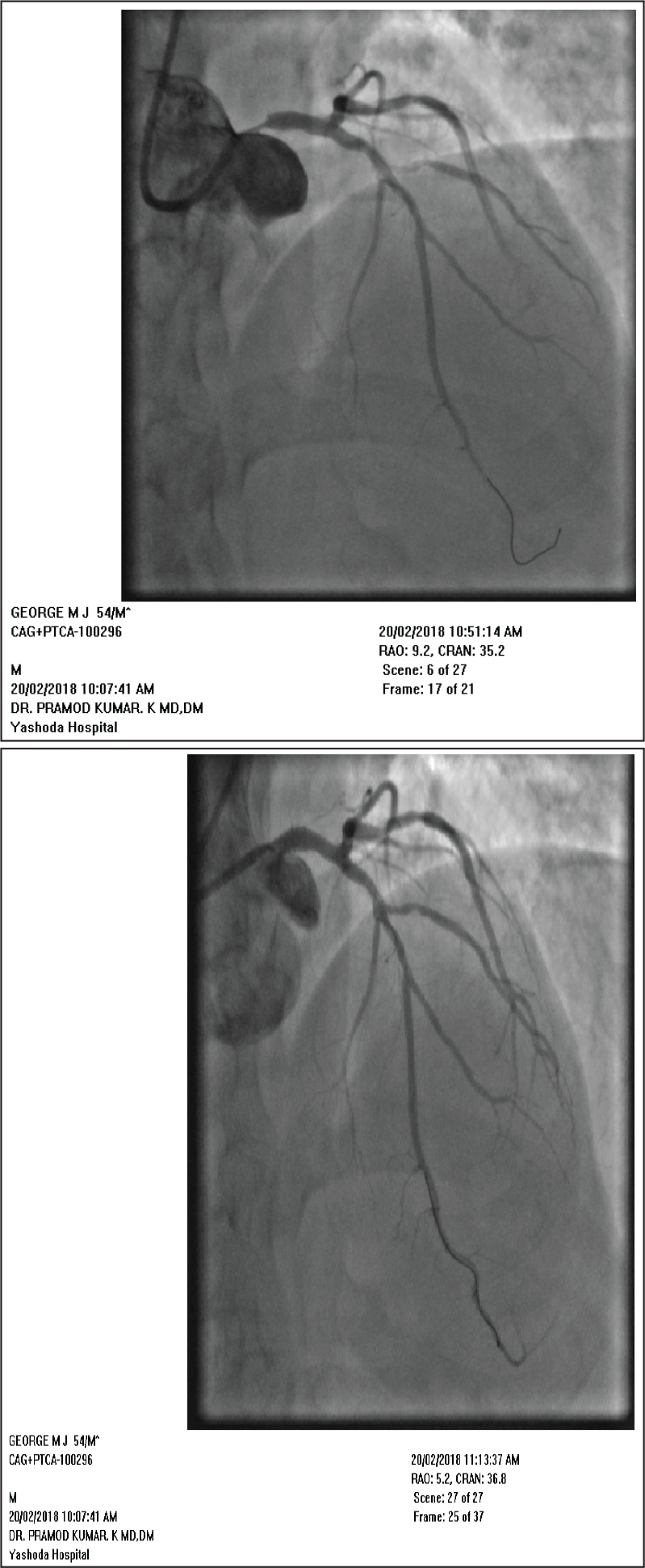
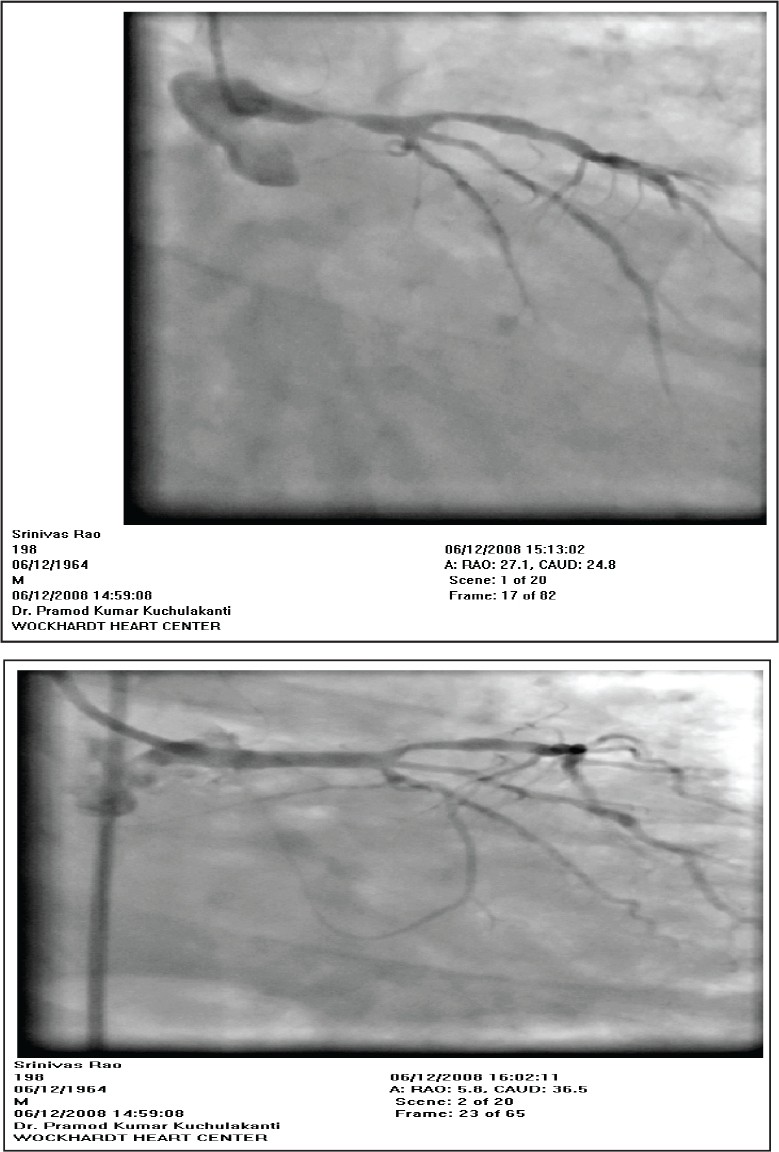
Ostial and shaft lesions may be easily carried out by appropriate sized stents and optimizing the result with post-dilation using a non-compliant balloon. When treating ostial LM lesions one or two struts should be positioned into aorta and adequate dilatation should be done without causing dissection of aorta. Examples of Ostial and Shaft lesion stenting are shown in Figures 4 (a) and (b) and 5 (a) and (b).
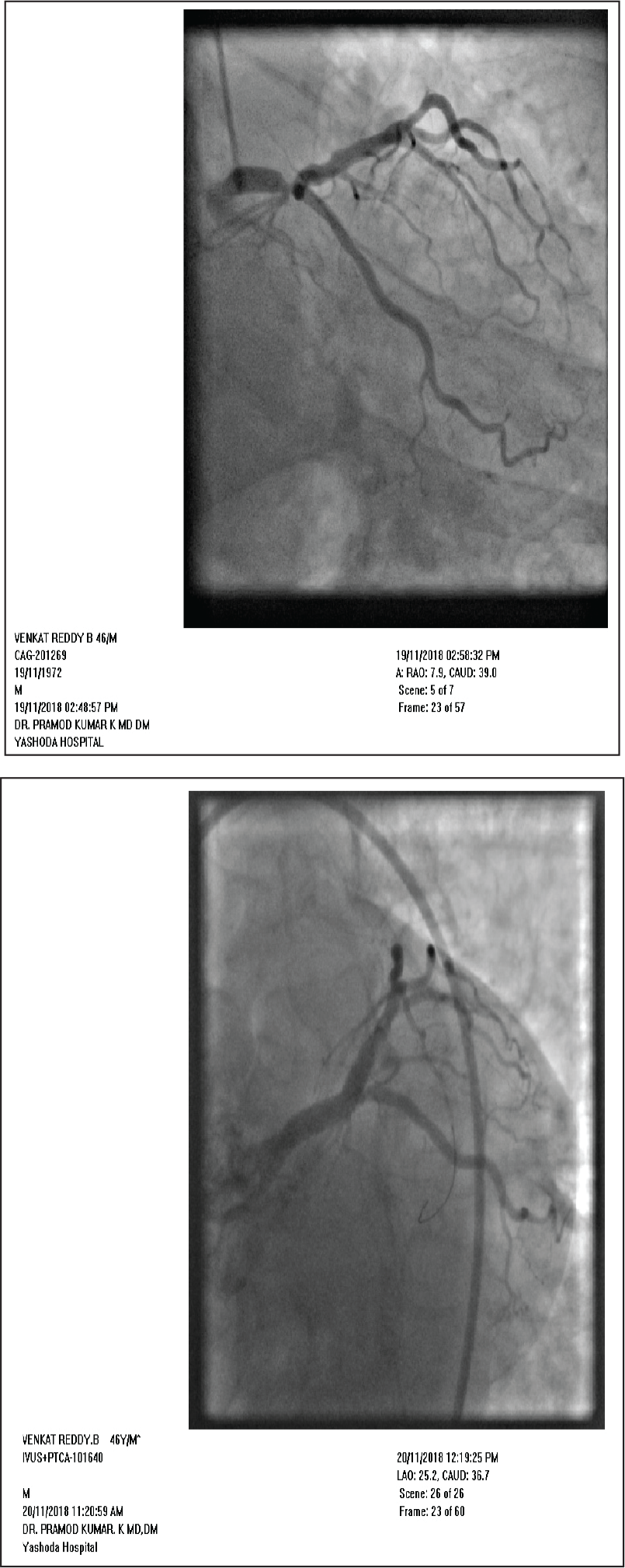
Distal LM lesions may be treated by several approaches:
(a) Critical Ostial Left Main Lesion (b) After Stenting of Ostial Left Main
(a) Severe Stenosis of the LM Shaft (b) Post Stenting of Shaft Lesion
(a) Distal Left Main and LAD Lesion (b) Cross-over Stenting From Left Main to LAD
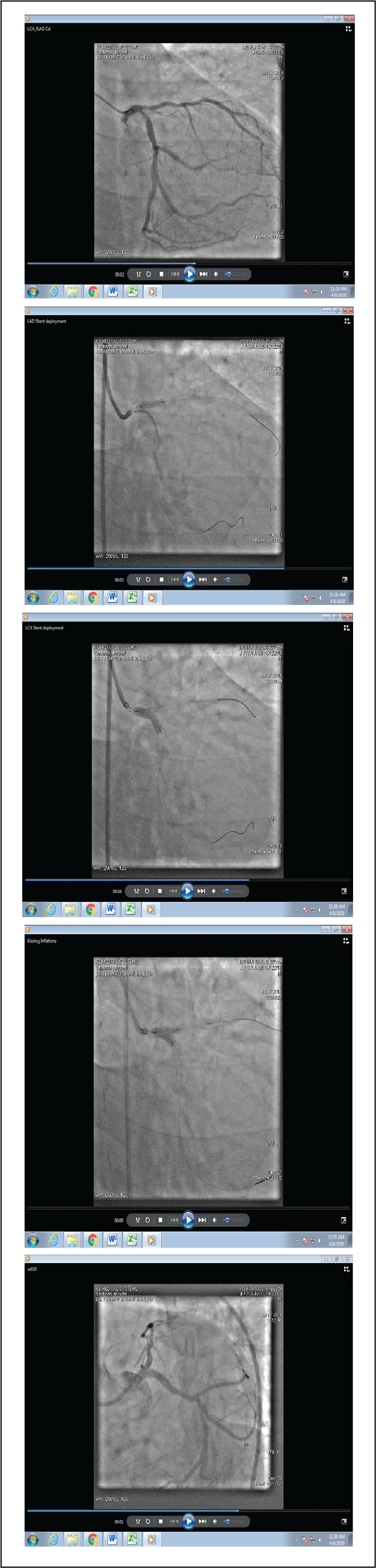
(a) Pre-PTCA Angio Showing Distal LM Bifurcation Lesion Involving Ostia of LAD and LCX (b) Deployment of Stent in LAD While LM-LCX Stent in Position (c) Deployment of LM-LCX Stent and Mini Crush of LAD Stent (d) Kissing inflation of Both LM-LCX and LAD Stents (e) Final Angiogram Showing Good Result
Mechanical Circulatory Support
In patients with acute coronary syndrome, severe left ventricular dysfunction, and hemodynamic instability undergoing LMCA intervention, it is important to be well versed with mechanical circulatory support devices. These devices provide cardiac output sufficient to maintain myocardial flow and end-organ perfusion, and help to unload the left ventricle during the procedure. Currently there are four percutaneous mechanical circulatory devices available: intra-aortic balloon pump, impella, extra corporeal membrane oxygenator and lastly tandem heart. IABP is the most commonly available device with easy and expeditious insertion, but is associated with low efficacy to augment cardiac output. It may be useful in pre-shock/shock patients, electively or during emergency crash situations during LM PCI. Impella provides higher cardiac output and may be considered in high risk LM PCI or during severe shock. Tandem heart and ECMO are mainly useful for cardiac arrest situations. 32 It is very important to plan the device strategy prior the commencement of LM intervention.
Conclusions
Percutaneous intervention with stent implantation for LMCA disease has become a standard procedure in contemporary practice with safety, expedited recovery, and durability. Precise selection of the strategy aided by intra coronary imaging, functional evaluation, and mechanical support when needed have improved the immediate and long-term results in this high risk intervention. It is however important to have a team approach and operator expertise before embarking on LMCA interventions.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.