
Abstract
In-stent restenosis (ISR) within bifurcation lesions of the left main (LM) coronary artery (LMCA) is challenging due to its complex anatomy and critical function. This case series highlights 3 patients with LM bifurcation ISR (Medina 1,1,1) post-index intervention using different stent strategies as follows:
Case 1
A 58-year-old male developed distal LM bifurcation stenosis after ostial left anterior descending artery (LAD) stenting. Mini-culotte bifurcation angioplasty effectively managed this.
Case 2
A 62-year-old male presented with neo-atherosclerosis-induced distal LM bifurcation ISR post-provisional LM-left anterior descending artery (LAD) stenting. A single-stent crossover with a drug-coated balloon in a large side branch achieved optimal flow restoration.
Case 3
A chronic total occlusion in the right coronary artery and distal LM bifurcation ISR due to stent overhang into LMCA in a 72-year-old male was resolved with a string culotte technique.
These cases underscore ISR management strategies tailored to patient-specific anatomy and clinical needs, advocating advanced imaging techniques like intravascular ultrasound and optical coherence tomography for procedural precision and safety.
Keywords
Learning Points
Maintain left main (LM) bifurcation procedures as simple, safe, and minimal as possible to optimize outcomes and reduce complications. Intravascular imaging techniques like optical coherence tomography (OCT) and intravascular ultrasound (IVUS) are crucial for addressing limitations in the Medina classification and providing a comprehensive assessment of bifurcation lesions, including plaque characteristics and bifurcation angles. There is no fixed criterion for choosing between 1-stent or 2-stent strategies. Intravascular imaging helps guide this decision by evaluating critical lesion characteristics and predicting side branch (SB) closure. The DEFINITION criteria assist in distinguishing between complex and simple bifurcations, aiding in stent strategy decisions. Drug-coated balloons (DCBs) are emerging as a promising treatment for SB lesions and in-stent restenosis (ISR). Adequate Proximal Optimization Technique (POT) is essential to prevent complications such as SB closure, stent malapposition, or underexpansion, which can lead to ISR or stent thrombosis. Carinal shift is a significant cause of SB compromise and must be managed carefully.
Background
Management of coronary artery disease (CAD) encompasses both medical and interventional strategies, including percutaneous transluminal angioplasty (PTCA). 1 However, coronary bifurcation lesions represent a complex subset, and PTCA can be challenging to perform in true bifurcation lesions due to worse immediate and long-term outcomes compared to simple lesions. 2 Bifurcation lesions occur in 15%-20% of all percutaneous coronary intervention (PCI) cases. 3 A bifurcation lesion is a coronary artery narrowing occurring adjacent to, and/or involving, the origin of a significant side branch (SB) that cannot be compromised.
The Medina classification for bifurcation lesions, proposed in 2005, is a simple and widely accepted system based on plaque involvement in 3 anatomic segments. 4
Various stenting techniques have been developed to manage bifurcation lesions, each with benefits and limitations. 5 The increased risk of negative outcomes including abrupt closure of SB, stent thrombosis (ST), and in-stent restenosis (ISR; re-narrowing of a coronary artery that has previously been treated with a stent)6, 7 in bifurcation procedures has led to a debate regarding its management.
The following vital aspects need to be considered during bifurcation stenting:
Importance of SB One-stent versus two-stent strategy upfront Behavior of ostial left circumflex artery (LCx): Achilles heel of left main (LM) bifurcation lesion Minimization of metal at carina and preservation of the flow dynamics Crossover vs. nailing of the ostial left anterior descending artery (LAD), final kissing balloon inflation (FKBI) of SB, and proximal optimization technique (POT)-side-POT for SB in the treatment of ostial LAD lesions Utility of intravascular imaging (IVI) in deciding optimal 1-stent or 2-stent strategy, preventing SB loss in provisional stenting, predicting the behavior of SB after provisional stenting of the main vessel (MV) Role of fractional flow reserve (FFR) in assessing SB occlusion in provisional stenting
Due to the risk of target vessel revascularization, stent failure because of ST or ISR in the main branch (MB) or SB, loss of SB because of sudden abrupt closure or development of stenosis on follow-up; treating bifurcation lesions requires specialized approaches beyond conventional PCI techniques, with an emphasis on optimizing stent placement. 8
We present 3 cases where patients presented primarily with critical left main coronary artery (LMCA) bifurcation ISR (Medina 1,1,1) disease after 1-1.5 years of the index procedure, emphasizing the reason for ISR occurrence and discussing the optimal management strategy. Various interventional strategies including mini culotte and string culotte techniques, as well as the use of drug-coated balloons (DCBs) and advanced imaging modalities, such as optical coherence tomography (OCT) for precise guidance during PCI are discussed below.
Case presentation
Case 1: Mini Culotte Technique in Bifurcation Lesions
Patient presentation and assessment
A 58-year-old male, with a history of hypertension, CAD, previous stenting to ostial LAD 1.5 years ago, presented with New York Heart Association (NYHA) III angina and dyspnea. Electrocardiography (ECG) showed T-wave inversion in leads V3-V6. Echocardiography (ECHO) showed moderate left ventricle (LV) systolic dysfunction with a left ventricular ejection fraction (LVEF) of 37%, hypokinetic anterior, inferior, and lateral walls, mild mitral regurgitation (MR), and tricuspid regurgitation (TR).
Challenge
Coronary angiogram (CAG) revealed distal LM bifurcation (Medina 1,1,1), 90% lesion and mid right coronary artery (RCA) 100% chronic total occlusion (CTO). The patient refused the option of coronary artery bypass surgery (CABG). The RCA was opened first, followed by the decision to treat the LM bifurcation. Angiography showed that the reason for ISR was a geographical miss (GM) while stenting the ostial LAD. A GM refers to inadvertent stent deployment entirely or partially missing the target lesion, associated with a significantly increased 1-year target vessel revascularization rate independent of clinical and anatomic variables. 9
Intervention
The RCA intervention was performed first, followed by the LM bifurcation procedure 23 days later. Since there was a GM, the SB was a huge LCx subtending a large myocardium that cannot be jeopardized in any way; therefore, we adopted a dedicated 2-stent strategy. Because both the MV and SB were of almost equal size and had a favorable angle, we opted for a culotte technique. No LV assist device was used. The choice of the culotte strategy was driven by the need to cover the distal LM bifurcation adequately, where disease had developed due to disturbed flow dynamics caused by the geographical miss at the LAD ostia. Additionally, financial constraints precluded the use of OCT and a drug-coated balloon (DCB) in the SB. Both LAD and LCx were wired with RUNTHROUGHTM NS wire (Terumo Interventional Systems, USA) in LAD and Fielder FC™ in the LCx. Both LAD and LCx lesions were pre-dilated with a 3.0 × 15 mm noncompliant (NC) balloon at 18 atmospheres (atm). This was followed by the deployment of a 4.0 × 22 mm drug eluting stent (DES) in the ostial LMCA-LCx at 14 atm, followed by a POT with a 4.5 × 08 mm noncompliant (NC) balloon at 20 atm. RUNTHROUGHTM NS wire was recrossed into the LAD through LM-LCx stent struts. Struts were dilated with 1.5 × 10 mm and 3.0 × 15 mm NC balloons. DES (4.0 × 22 mm) was deployed in the LAD keeping minimal struts in LMCA at 14 atm (mini culotte) overlapping with the previous LAD stent. Further, POT was performed with a 5.0 × 08 mm NC balloon at 16 atm. The Fielder FC™ wire was recrossed into the LCx through the stent struts and dilated with 1.5 × 10 mm and 3.0 × 15 mm NC balloons at 16 atm.
The stents in the LAD and LCx were post-dilated with 4.5 × 8 mm NC balloons at 15-20 atm, followed by kissing balloon dilation with 4.0 × 08 mm NC (LAD) and 4.5 × 08 mm NC (LCx) balloons at 14 atm, and again with swapping of balloons. Final rePOT was done with a 5.0 × 08 mm NC balloon at 14 atm. The patient was started on dual antiplatelet therapy with ecosprin 150 mg once daily (od) and clopivas 75 mg od post-procedure.
Post-procedure outcome
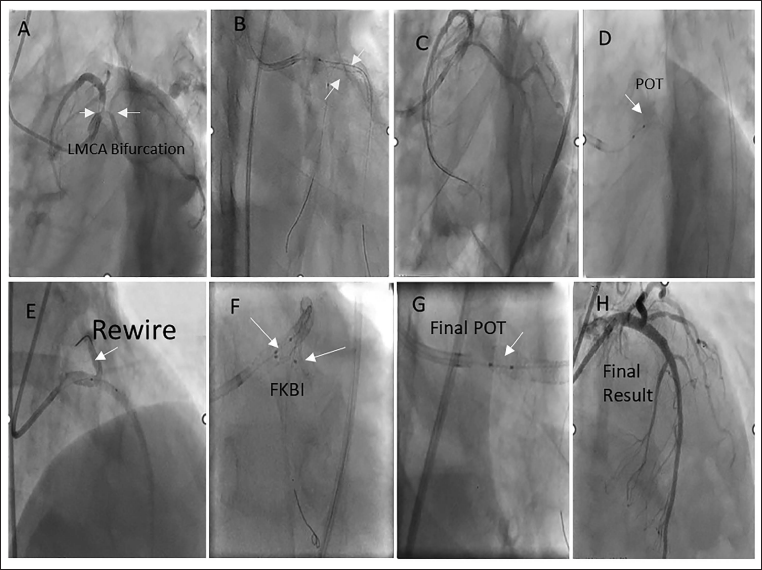
The final result of the intervention was a successful restoration of blood flow with thrombolysis in myocardial infarction (TIMI) III flow. Figure 1 recapitulates the sequence of events in Case 1.
Representative Images for Case 1. (A) LMCA Bifurcation (1,1,1) 90% (B) RFA/7fEBU 3.5/7F, RUNTHROUGHTM NS Wire in LAD, Fielder FC™ in LCx (Retroflexed LCx); Pd with 3.0 × 15 mm in Both LAD and LCx. (C) Resolute Onyx 4.0 × 22 in LM-LCx at 14 atm. No Distal Dissection Was Noted. (D) POT 4.5 × 8 mm NC at 20atm. (E) Recrossing of RUNTHROUGHTM NS Wire in LAD Through LM-LCx Struts. Struts Were Dilated with 1.5 × 10 mm and 3.0 × 15 mm NC Balloons. DES (4.0 × 22 mm) Was Deployed in the LAD Keeping Minimal Struts in LMCA at 14 atm (mini culotte) f/b POT and Recrossing of Wire in LCx (F) FKBI 4 × 8 mm in LCx and 4.5 × 8 in LAD at 14 atm, Swapping of Balloons. (G) Final POT 5.0 × 8 mm NC at 18 atm. (H) Final Result.
Follow-up
The patient maintained a stable clinical condition for a period of 1 year following treatment. Unfortunately, after this 1-year period, the patient succumbed to dengue shock syndrome, leading to mortality.
Case 2: Neoatherosclerosis Management with 1-Stent Strategy and DCB
Patient presentation and assessment
A 62-year-old male patient with hypertension presented with complaints of angina on exertion (AOE) and dyspnea on exertion (DOE) NYHA Class III. The patient had a history of CAD and stenting to the LMCA-LAD and mid-RCA 1.2 years ago. His ECG showed normal sinus rhythm (NSR) with a QS pattern in leads V1-V3, I, aVL, and T-wave depression in V1-V6, suggesting ischemic changes. ECHO revealed severe LV systolic dysfunction with an LVEF of 35%, mild MR, and both anterior and inferior wall being hypokinetic.
Challenge
CAG showed ostial RCA 99% stenosis with TIMI I flow and 90% LMCA bifurcation (Medina 1,1,1) disease. The RCA was fixed first with a DES, followed by intervention to the LM bifurcation 8 days later. No LV assist device was used. It was important to assess the cause of ISR and also minimize the stent layer at the bifurcation site.
OCT was performed to identify the cause of ISR. Ostial LAD showed neoatherosclerosis (presence of lipid-attenuating plaque on OCT), with few stent struts overlying at the ostial LCx leading to SB stenosis while the LMCA stent was well apposed. The pre-procedural lesion assessment at the LM-LAD is shown in Supplementary Figure 1. Assessment of the LM-LCx pre-OCT run is presented in Supplementary Figure 2.
The bifurcation angle and carina tip can be derived from OCT pullback in MV. Analysis using reconstructed OCT images, that is, cut-plane analysis using pullback from MV and angle measurement in the SB in the longitudinal view is presented below. (A) Two wires for bifurcation from MB to SB. (B) Detected SB location. (C) Length between the proximal branching point and the carina tip (BP-CT length). (D) Cut-plane analysis. (E) Longitude mode. (F) Distal reference. (G) LAD ostia. (H) LM proximal.
SB location. (G) Polygon of confluence and point of bifurcation.
Intervention
The treatment approach in this case was a single-stent strategy with the additional use of a DCB in the SB. This strategy aimed to address restenosis by using DCB to deliver medication directly to the artery wall, reducing the likelihood of further plaque buildup without adding another stent layer into the artery, which aligns with the provisional strategy proposed by the European Bifurcation Club (EBC). Provisional stenting was chosen due to the presence of neoatherosclerosis in the LM-LAD stent, necessitating the use of a DES in the LM-LAD. Dedicated bifurcation stenting was avoided to prevent the formation of 3 metal layers at the carina, which would increase the risk of ISR) at the ostial LCx, target vessel revascularization (TVR), and target vessel failure (TVF). Therefore, DCB was considered a promising strategy to avoid excess metal layers and effectively treat a large SB. A comparison between provisional and 2 stent strategy is provided in Supplementary Table 1.
A 7F right femoral arterial access was obtained. The left system was hooked with a 7F XBU/3.5 guide catheter. The lesion in LM-LAD was crossed with a Fielder FC™ PTCA wire, and a RUNTHROUGHTM NS PTCA wire was placed in the LCx. The lesions in the LCx and LAD were pre-dilated with a 3.5 × 10 mm Wolverine cutting balloon at 10atm. Pullback from LAD-LMCA showed fibroatheroma at the ostia of the LAD with stent struts overlying the ostia of the LCx. OCT pullback from the LCx to the LM revealed a fibroatheroma plaque at the ostial LCx. A Resolute Onyx 4.0 × 18 mm stent (Medtronic, India) was deployed in the ostial LM to proximal LAD at 14 atm, followed by POT with a 4.5 × 8 mm NC balloon at 14 atm. The LM-LAD stent struts were opened up first with a 2.0 × 10 mm SC balloon followed by inflation of a DCB SeQuent Please Neo™ 3.5 × 15 mm (paclitaxel-eluting balloon) at 10 atm for 90 s at the ostia of the LCx keeping a few mm in the LMCA. FBKI was done with 4.0 × 10 mm NC in the LAD and 3.5 × 15 mm DCB in the LCx at 12-14 atm. Final POT was performed using 4.5 × 8 mm NC balloons at 18 atm. The patient was started on dual antiplatelet therapy with ecosprin 75 mg od and ticagrelor 90 mg twice daily (BD) post-procedure.
Post-procedure outcome
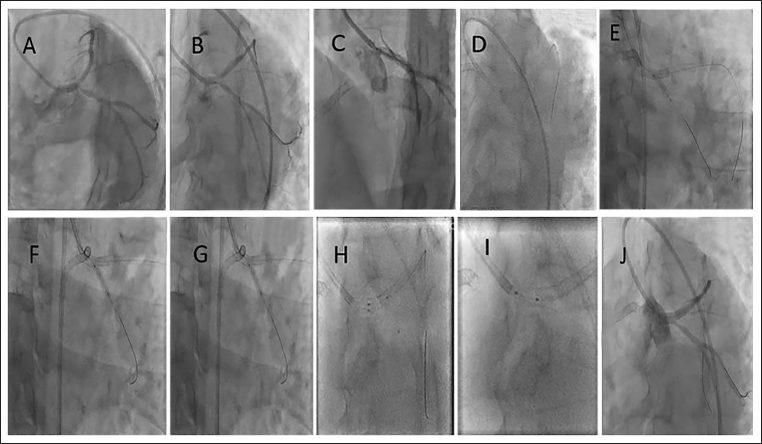
The final OCT pullback confirmed the absence of major dissections, and that adequate MLA was achieved in the ostial LCx and the proximal LM. The stent in LAD to LM was well apposed and expanded. A figure of 8 was seen at the polygon of confluence without any stent strut overhanging at the LCx ostia. Post-procedural lesion assessment at the LM-LAD is shown in Supplementary Figure 3. Figure 2 recapitulates the sequence of events in Case 2.
Representative Images for Case 2. (A) LMCA Bifurcation (1,1,1) 90% (B) EBU 3.5/7f, Fielder FC™ in the LAD, RUNTHROUGHTM NS Wire in the LCx. Both LAD ISR and LCx Dilated with 3.5 × 10 mm Wolverine at 10 atm. (C) Onyx 4.0 × 18 mm from the Ostial LM to LAD at 14 atm. (D) POT with 4.5 × 8 mm NC. (E) Stent Struts Dilated with 2.0 × 10 mm SC Balloon. (F) Stent Struts Dilated with 2.0 × 10 mm SC Balloon. (G) 3.5 × 15 mm DCB at 10 atm for 90 s. (H) FKBI with 4.0 × 10 mm NC in the LAD and 3.5 × 15 mm DCB in the LCx at 12 atm. (I) Final POT 4.5 × 8 mm NC at 18 atm. (J) Final Result.
Follow-up
The patient experienced an episode of exertional angina, leading to a CAG. The angiography revealed a 99% occlusion due to ISR at the ostio-proximal segment of the RCA. The left system was observed to be completely normal with TIMI III flow.
Case 3: String Culotte Approach for Stent Overhang
Patient presentation and assessment
A 72-year-old male patient presented with chest pain radiating to the left shoulder, accompanied by sweating and breathlessness upon walking, which had been persisting for 3 months. He had a history of COPD, hypertension, chronic kidney disease, CAD, and stenting to ostial LAD done 8 months back. ECHO indicated moderate LV dysfunction with an LVEF of 37% and hypokinesia of the anterior wall.
Challenge
CAG showed double vessel disease with RCA as 100% CTO and critical LMCA bifurcation disease (Medina 1,1,1). It was appreciated that the previous 3.0 mm LAD stent was overhanging into the LMCA by 2-3 struts, and that the stent was grossly malapposed and underexpanded. This led to the development of a new disease at the LMCA bifurcation.
Intervention
The intervention strategy was to minimize the stent layers at the carina and LAD. Since the stent struts were already in the distal LMCA, the string culotte technique was used, thereby minimizing additional stent layers in the carina and LAD. The string culotte technique is also called the cross-stent technique, and is a modified form of the culotte technique (1-2 stent strut protruding from the SB into the MV) and is used to minimize the overlapping of the stent struts in the 2-stent technique). (Kawasaki et al. 2010) No LV assist device was used during the procedure.
A 6F right radial access was obtained. EBU 3.0/6F was engaged to the left system. The lesion in the LCx was crossed with a Fielder XT™ wire through LM-LAD stent struts, which were already overhanging in the distal LMCA. This was confirmed on the stent boost. The LCx was predilated with a 1.5 × 10 and 2.5 × 10 mm NC balloon at 20 atm. A RUNTHROUGHTM NS wire was placed in the LAD (the wire entered forming a curve ensuring entry into the stents through the stent struts and not behind the struts). The LAD stent was postdilated with 3.5 × 10 mm NC at 24 atm. The wire was then removed from the LAD. A Resolute Onyx 3.5 × 26 mm stent was deployed in the LM to LCx, passing through the already stented LAD with 2 struts hanging in the distal LMCA (string culotte). POT was performed with a 4.0 × 6 mm NC balloon at 16 atm.
A run-through NS wire was recrossed into the LAD through the LMCA-LCx stent struts, and the struts were dilated with a 1.5 × 15 mm balloon. This was followed by postdilation of both LAD and LCx stents with 3.5 × 10 mm NC. FKBI with the same balloons was done at 12-14 atm. Final POT was performed with 4.5 × 6 mm NC at 12atm. The patient was started on dual antiplatelet therapy with ecosprin 75 mg od and ticagrelor 90 mg BD post-procedure.
Post-procedure outcome
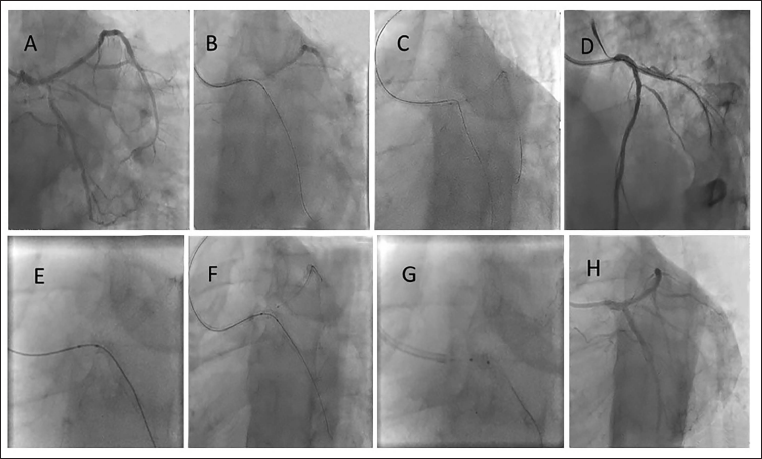
TIMI III flow was achieved. Figure 3 recapitulates the sequence of events in Case 3.
Representative images for Case 3. (A) LMCA bifurcation (1,1,1) 90% (B) Fielder XT™ to cross the LCx Through LMCA-LAD stent struts, predilated with 1.5 × 15 mm, and 2.5 × 10 mm NC at 20 atm. (C) RUNTHROUGHTM NS Wire in LAD and LM-LAD stent dilated with 3.5 × 10 mm NC at 24 atm. (D) Onyx 3.5 × 26 mm from the LM-LCx deployed at 12 atm. (E) POT 4.0 × 6 mm NC at 16 atm. (F) RUNTHROUGHTM NS Wire in LAD, Stent Struts Dilated with 1.5 mm Balloon f/b Post Dilation with 3.5 NC Each in the LAD and LCx at 12-14 atm and FKBI with Same @12 atm. (G) Final POT 4.5 × 6 mm NC at 12 atm. (H) Final Result.
Follow-up
The patient visits for follow-up and is currently doing well.
Discussion
This case series explores the complexities of managing coronary bifurcation lesions in 3 patients who developed post-PCI complications in the form of new critical disease developing at the distal LM bifurcation (Medina 1,1,1) and ISR in the previous stent. Each case highlights unique challenges in CAD management, different mechanisms that led to disease development, and tailored interventional strategies. The aim of treating a bifurcation lesion is to prevent TLR and target vessel failure. Thus, aspects that need to be discussed at the index procedure itself include 1-stent versus 2-stent strategy, type of bifurcation strategy if 2 stents are used, IVI to assess the carina angle, length of the lesion, placement of the stent, recrossing of the wire through the distal stent strut, poststenting parameters including expansion and apposition of the stent, and prevention of stent struts overlying in the polygon of confluence. In the treatment of bifurcation lesions in the coronary artery, diverse strategies, and techniques are being explored with a focus on minimizing metallic elements, enhancing procedural outcomes, and using imaging techniques to optimize the outcomes. 10
Bifurcation CAD
Coronary bifurcations are frequently affected by atherosclerotic disease. Endothelial shear stress (ESS) is the main flow-related factor affecting the distribution of atherosclerosis in a bifurcation. Plaques are more prevalent in low-ESS areas, such as the lateral walls of the MV and SBs, whereas they are less common in the flow divider or carina, characterized by high ESS.11–13 Furthermore, it has been demonstrated that ISR is governed by the same flow laws by which the pattern of the initial lesion is reproduced with predominant neo-intimal proliferation. 14 Atheroma progression results from flow disturbances caused by the initial plaque and extends in an anterograde and circular manner. 15
The first step in approaching a bifurcation lesion is to identify and define it. The EBC defines a bifurcation lesion as a coronary artery narrowing occurring adjacent to, and/or involving the origin of a significant SB, which is defined as a branch that cannot be compromised in the global context of a particular patient, that is, a branch responsible for symptoms or ischemia, collateralizing vessel, and left ventricular function. PCIs for bifurcation lesions are associated with lower procedural success rate than for non-bifurcation lesions.16, 17 Moreover, bifurcation lesions are a technically demanding and complex subset due to the following reasons:
Clinical settings and anatomical relevance of the 2 branches (size, length, supplied territory, viability, collateral, etc.) Disease extent in 2 branches and plaque morphology (thrombus, calcium, etc.) Ease of access of 2 branches (guidewires, balloons, stents, atherectomy devices, etc.) Anatomy of bifurcation (carinal angle, angle between proximal MB, distal MB and SB, carina-branch tip length, eccentric, or concentric disease at bifurcation)
DEFINITION Criteria for Complex Bifurcation Lesions
The DEFINITION criteria for bifurcation lesions were developed based on the DEFINITION study.18, 19 The criteria encompass 2 major and 6 minor angiographic criteria (Table 1). These criteria were used to distinguish between simple and complex bifurcation lesions.
Components of the DEFINITION Criteria.
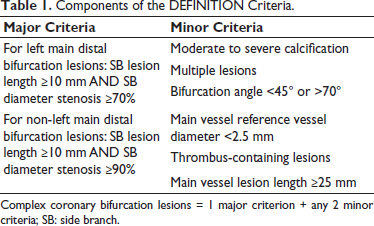
Complex coronary bifurcation lesions = 1 major criterion + any 2 minor criteria; SB: side branch.
A bifurcation lesion is defined as complex if it meets 1 major criterion plus any 2 minor criteria. For complex bifurcation lesions, provisional stenting is associated with a higher risk of cardiac death and major adverse cardiac events (MACE) compared with a systematic 2-stent approach. On the contrary, for simple bifurcation lesions, a systematic 2-stent strategy results in a higher risk of MACE compared with provisional stenting.
LM Bifurcation Lesion: A Difficult-to-Treat Subset
LMCA bifurcation disease behaves differently as compared with the non-left main bifurcation subset. It is characterized by a large-sized parent vessel with a rapidly tapering MV caliber, wide distal bifurcation angle, a huge myocardial area perfused by SB (especially when left dominant circulation), and frequent involvement of a trifurcation lesion with a large ramus intermedius branch, which are some of the factors that make LM bifurcations more complex and technically difficult from non-LM bifurcations.20, 21, 22 Development of target lesion revascularization (TLR) and TVF (ISR or ST) in LMCA lesions is a very severe clinical complication. CABG is still the therapy of choice for treating LMCA bifurcation lesions. 23 However, with the current understanding of bifurcation anatomy, advancements in PCI techniques, evolution of second-generation DES, and adjunctive pharmacotherapy, there is a need for an evolved standard of care for LMCA revascularization.24, 25
Classification of Bifurcation Lesions
Bifurcation lesions may be classified in various ways.26–29 The most commonly used classification system for clinical and research purposes is the Medina classification according to which, these lesions are divided into 3 segments for quantitative coronary angiographic analysis: proximal MV, distal MV, and SB. A binary number (0 or 1) is assigned to each of these segments based on the absence or presence of a stenosis >50%. 30 According to the Medina classification, true bifurcation lesions are defined as 1.1.1, 1.0.1, and 0.1.1, that is, more than 50% involvement of the SB lesion is essential to consider the lesion a true bifurcation lesion.
However, this classification system has limitations, as it does not identify the length of the lesion in the ostium of the SB, length of the LMCA before the bifurcation, or the presence of trifurcation and angulation. Moreover, no differentiation is made between a normal segment and a lesion that is <50%. It also does not account for plaque morphology, that is, whether it is calcific, thrombotic, etc. These shortcomings highlight the need for a more comprehensive classification, encompassing bifurcation angles and plaque distribution and length.
All these factors can make a difference in choosing a strategy to treat bifurcation lesions. The choice of a 2-stent approach depends on factors such as SB size, length of the lesion in the ostial SB, percent stenosis of the SB, the angle between the distal MV and SB, and plaque morphology at bifurcation; this information may be essential to ensure effective treatment for each specific case. 31
One-Stent Versus Two-Stent Strategy
Coronary bifurcations may develop atherosclerotic disease because of flow dynamics. Therefore, ST and restenosis rates are higher in bifurcation CADs and there has been a lot of debate on the management of bifurcation CADs. The question of when to intervene in the SB along with the MV and using which strategy is always under scrutiny. Two philosophies of bifurcation lesion management exist, of which, one is a provisional stent placement strategy, in which the MV is treated, and the SB is left alone unless threatened or if actual closure occurs; in this case, the SB is also treated with a bailout technique like TAP or reverse internal crush. The second strategy is a dedicated 2-stent strategy, in which the treatment of both the MV and SB is planned from the beginning.
According to the current guidelines from the EBC, the preferred option for the majority of bifurcation lesions is provisional stenting, while an upfront 2-stent strategy may be used for lesions of higher complexity, particularly those involving an SB that supplies a substantial myocardial territory. 32
LM bifurcation stenting strategies highlight the criticality of choosing the most appropriate treatment approach based on lesion anatomy, involving a decision between a 1-stent and 2-stent strategy. 33 The basic idea behind PCI of any bifurcation disease is to keep things simple, maintain the flow dynamics, and minimize disturbances in the original anatomy of the coronary artery; this is achieved by minimizing metal layers by ensuring minimal overlap and ensuring that the stent is well-apposed and expanded. 34
In all the 3 cases described in this report, provisional stenting was performed as the index procedure. Because of the disturbed flow dynamics at the bifurcation due to various reasons, the patients again presented with LM bifurcation (1,1,1) ISR within a span of 8 months to 1.5 years. In 6% to 18% of cases, SB compromise was seen after MV stenting. 35 SB occlusions usually occur due to carina shifts; however, they may also occur due to plaque shifts, ellipse deformations of the ostial SB, impacts of dissection, and protrusion of LM stent struts on SB arterial flow.
Predictors of SB occlusion observed with various imaging techniques are shown in Table 2. 36
Typical Predictors of SB Occlusion.
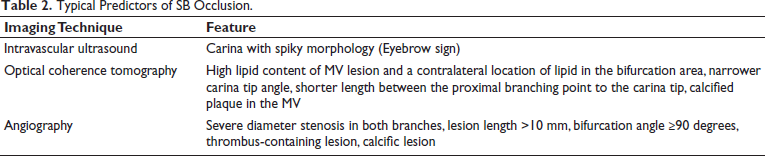
In all such conditions, based on IVI and angiogram, the decision of 1 stent vs 2 stents can be taken.
The following fallacies are associated with provisional stenting:
Only using an angiogram does not provide all the required information about bifurcation anatomy. Angle of SB origin can only be assessed by IVI (whether or not the carina is spiky) Underexpansion and malapposition occur due to gross mismatch of MV and distal vessel GM or pulling of the stent occurs in the LMCA while nailing the ostia of LAD Abrupt SB occlusion or development of ISR at SB ostia may occur in the future
Among our cases, Case 1 featured a GM at the ostia of LAD, and Case 3 featured underexpanded and malapposed stent struts hanging in the distal LMCA leading to the development of the lesion at the distal LMCA, ostial LAD, and ostial LCx. In Case 2, there was crossover stenting from LMCA-LAD and subsequent neoatheroma, and stent struts overlying the ostial LCx, leading to the formation of the lesion at the bifurcation segment.
Ostial LAD Lesions
Ostial coronary lesions are one of the most challenging subsets of bifurcation lesions to treat during PCI. Ostial LAD lesions usually occur in continuation with the distal LM. 37 Compared to nonostial lesions, ostial lesions have high rates of ISR and long-term adverse events.38, 39 Slippage of the balloon and extension of dissection into the LMCA can lead to worse post-procedural outcomes. Protrusion of stent struts into the LM versus incomplete coverage of the ostial lesion is not uncommon in intravascular ultrasound (IVUS) studies 40 and can lead to an increased risk of restenosis and ST. 41 Most importantly, since the adjacent LCx is the Achilles heel of coronary bifurcation lesions (CBL), the LCx may be compromised during ostial LAD stenting acutely or during follow-up and may lead to ischemia, TLR, and TVF. 42 These observations were seen in all 3 of our cases.
The first case showcases the utilization of the mini culotte technique to address a GM in a bifurcation lesion. By deploying 2 stents strategically, this approach ensured full coverage of the diseased area, exemplifying the importance of precision in bifurcation interventions, particularly if significant stenosis and thrombotic disease occur. The culotte technique is one of the most useful in handling bifurcation lesions, allowing for optimal coverage of the diseased segments and minimizing the risk of SB occlusion. 43 It is performed for coronary bifurcations when the SB is important and needs to be preserved, there is a high likelihood of SB occlusion after MV stenting, and the angle of the bifurcation is less than 70 degrees. 43
Stent Overhang
Stent overhang into the LMCA occurs when the ends of a coronary stent deployed in an SB extend into the LMCA. 44 If not properly addressed, stent overhang can lead to significant complications, including impaired blood flow leading to restenosis or ST.
The third case discusses the application of the string culotte approach to address complications arising from stent overhang into the LMCA. This strategy ensures minimal stent overlap, minimal metal layers, and optimal stent apposition, emphasizing the importance of innovative techniques in managing complex anatomical challenges.
Role of DCBs in Coronary Interventions
DCBs are particularly effective in treating ISR and can be employed as a stand-alone treatment, thereby minimizing the need for additional stents, and preserving vessel flexibility and thus flow dynamics.45, 46 Their role complements conventional stenting interventions by providing an additional layer of anti-restenotic therapy, which is instrumental in improving long-term outcomes. This includes reduced rates of TLR, showcasing their significance in modern interventional cardiology. 47
The second case in the series focuses on managing neoatherosclerosis using a 1-stent strategy complemented by a DCB. This approach underscores the evolving role of DCBs in coronary interventions, particularly in delivering medication directly to the artery wall. This targeted delivery helps in reducing the risk of further plaque build-up and restenosis without introducing additional layers of stent material and the formation of neocarina. DCBs deliver anti-restenotic drugs directly to vascular lesions during balloon inflation, effectively inhibiting smooth muscle cell proliferation and consequently reducing the risk of restenosis.
Role of Imaging
Imaging plays a crucial role in examining the anatomy of the bifurcation, calcification, bifurcation angle, wire recrossing during the procedure, stent struts covering the SB ostium, GM, and overhang of stent struts. The diffuse nature of LM bifurcation lesions makes angiography less reliable in gauging the severity of the disease at both branch ostia. Relying solely on angiography-guided interventions may lead to the risk of suboptimal outcomes, including SB occlusion in cases of a “true” bifurcation or unwarranted complex interventions that could potentially be avoided. Considering these challenges, pre-procedural IVI evaluation emerges as a valuable tool.
IVUS or OCT helps in identifying the causes of ISR post-index procedure and thus helps to decide the optimal strategy for the management of bifurcation lesions. 48 An IVUS-derived minimal lumen area exceeding 3.7 mm or a plaque burden below 56% in the LCx ostium serve as indicators that effectively rule out functional SB compromise, with FFR <0.8, following MV stenting in the treatment of LM bifurcations.
Importance of SB in Coronary Interventions
The importance of the SB, particularly the ostial LCx, in coronary interventions is underscored by its vulnerability to compromised blood flow due to various mechanisms. 36 These mechanisms include carinal shift, plaque shift, ellipse deformation of the ostial SB, and the impact of dissection and protrusion of LM stent struts on the SB arterial flow. 49 Predictors of compromised coronary flow in the LCx SB following LM-to-LAD crossover stenting involve a range of factors. These factors include the length of the LM artery stent, plaque burden in the LCx, minimum lumen area of the ostial LCx as assessed by IVUS, and the angles between the LAD and LCx (narrow angle) and between the LM and LCx (wide angle). These considerations highlight the crucial role of the SB in preserving optimal blood flow and illuminate factors that may impact its patency during coronary interventions. 36
Conclusion
The cases presented in this series emphasize the need for a tailored, patient-centric approach in managing post-PCI complications in CAD, especially bifurcation lesions. Leveraging advanced imaging techniques, such as IVUS/OCT, in the pre-procedural phase significantly enhances the precision of stenting strategies in LM bifurcation disease, contributing to improved procedural success and patient safety. This series offers insights and guiding principles for improved patient outcomes in LM bifurcation ISR management.
Footnotes
Acknowledgements
The authors of the article would like to thank BioQuest Solutions for the editorial assistance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors confirm that written consent for submission and publication of this case report has been obtained from the patient in line with COPE guidance.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.