
Abstract
Despite the progress made in technological advancements, the utilization of stenting for both protected and unprotected left main coronary artery (LMCA) disease remains associated with elevated rates of long-term mortality and significant adverse clinical events, sometimes manifesting as cardiogenic shock. A considerable number of individuals retain the opportunity to receive catheter-based interventional therapy as a viable substitute for re-operative coronary artery bypass grafting (CABG). Despite the changed appearance, patients with acute blockage of the protected LMCA still have major adverse cardiac events (MACE) at a similar rate. Acute occlusion of the unprotected LMCA as an acute coronary syndrome (ACS) is uncommon, but that of the protected LMCA is relatively rare. We present a case of a post-CABG patient who developed ACS as a posterior wall myocardial infarction and acute left ventricular failure due to obstruction of a protected LMCA with substantial stenosis across its distal segment extending to the left circumflex (LCx) artery. The pharmaco-invasive management of the protected LMCA thrombotic occlusion with primary percutaneous coronary intervention resulted in significant patient improvement. These lesions are amenable to complex and high-risk coronary intervention with current technology, and the results have been quite encouraging in terms of long-term survival.
Keywords
Introduction
Despite the advancements achieved in technology, the use of stenting for both protected and unprotected left main coronary artery (LMCA) disease continues to be linked with increased rates of long-term mortality and significant adverse clinical events, which may occasionally present as cardiogenic shock. A significant proportion of patients have the option to undergo catheter-based interventional therapy as a feasible alternative to re-operative coronary artery bypass grafting (CABG). Notwithstanding the altered physical manifestation, individuals with acute obstruction of the protected LMCA continue to exhibit significant unfavorable cardiac events at a comparable frequency.1 Acute occlusion of the LMCA is responsible for the poor clinical outcome owing to fatal arrhythmias and cardiogenic shock. 2 The existence of concurrent protected LMCA, on the other hand, may affect the clinical presentation and prognosis. According to the current studies, acute LMCA occlusion accounts for 0.8% of all primary coronary interventions (PCIs). 3 Despite the absence of clear guidelines for effective reperfusion techniques in acute occlusion of the LMCA, a rational evidence-based strategy is critical for the best clinical result. We present a case of acute occlusion of a protected LMCA resulting in a posterior wall myocardial infarction and acute left ventricular failure that was successfully treated with primary PCI and additional supportive measures.
Case Report
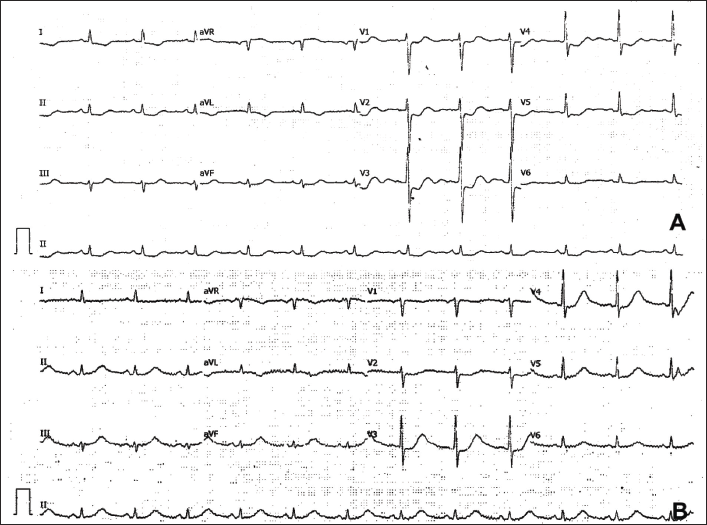
A 67-year-old man, hypertensive and diabetic, presented to the emergency room (ER) complaining of intermittent escalating epigastric discomfort at rest for the previous 15 days, which had worsened to constant ongoing pain for the last 4 h. In 2011, he underwent CABG surgery. His vital parameters were stable upon arrival, except for a few basal rales. The electrocardiogram (ECG) revealed ST-segment depressions in leads V1-6, II, III, and aVF, as well as T-wave inversions in leads I and aVL. The most significant observation was the presence of ST-segment elevation in lead aVR. In retrospect, we considered the ECG showed a mix of characteristics suggestive of a posterior wall myocardial infarction and LMCA occlusion (Figure 1A).
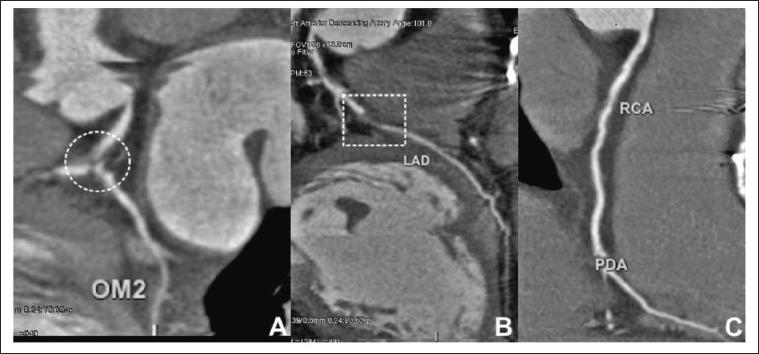
The patient had previously consulted with another cardiologist approximately one week prior regarding discomfort in the epigastric region and was recommended to undergo a computed tomography coronary angiography (CT-CAG). The results of this procedure indicated the presence of native coronary artery disease, a functioning left internal mammary artery (LIMA) graft connected to the left anterior descending artery (LAD), and a blocked saphenous venous graft (SVG) connected to the left circumflex (LCx) artery. As a result of the crucial stenosis at the distal LMCA bifurcation and the 90% stenosis in the proximal LAD, the LIMA to LAD graft filled the LCx retrogradely but only marginally. The right coronary artery (RCA) was not grafted because there was no substantial lesion at that time of CABG (Figure 2A−C).
He began complaining of shortness of breath before being transferred to the catheterization laboratory. In the ER, his vital parameters deteriorated to a heart rate of 112 beats per minute, blood pressure of 110/70 mm Hg, respiratory rate of 34 breaths per min, and room air saturation of 75%. He was started on continuous positive pressure ventilation after a clinical examination revealed sinus tachycardia and bilateral basal rales, which boosted his oxygen saturation to 98%. Intravenous nitroglycerine and furosemide infusions were started after an initial 80 mg bolus dose of furosemide. Transthoracic echocardiography revealed posterior and lateral wall hypokinesia with mild mitral regurgitation and grade II diastolic dysfunction, with a calculated ejection fraction of 35% [modified Simpson’s method].
Given ongoing epigastric pain and acute left ventricular failure, he was subjected to emergency CAG after administration of a loading dose of dual antiplatelet therapy (aspirin 325 mg and ticagrelor 180 mg). There was thrombotic occlusion of the LMCA, which was not described in the previous CT-CAG, and the rest of the findings were comparable to what was previously reported. The proximal segment of the non-grafted RCA demonstrated 70% stenosis (Figure 3A−F).
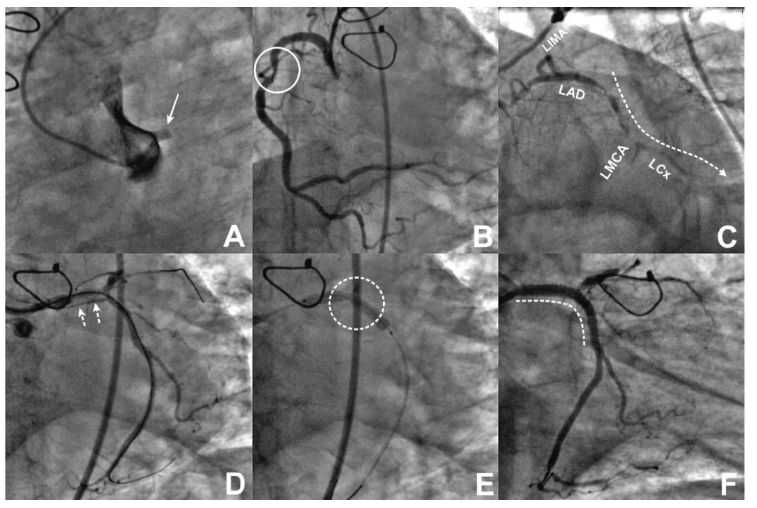
His laboratory parameter was within normal limits except elevated troponin (34 ng/ml; normal range 0−012 ng/ml) and N-terminal prohormone B-type natriuretic peptide (3200 pg/ml; normal value <450 pg/ml). We performed PCI via a trans-femoral approach on the occluded LMCA using a balance middleweight guide wire that initially did not cross the occlusion. The successful passage of the Fielder XT guide wire from the LMCA to the first obtuse marginal artery established the TIMI 2 flow. There was significant stenosis of the LMCA to the LCx, as well as a thrombotic burden across the distal segment of the LMCA extending into the proximal part of the LCx artery. A 3.5 × 26 mm zotarolimus drug-eluting stent is inserted after sequential pre-dilatation with 2.75 × 12 mm, 3.0 × 12 mm balloons at 20 atm. As a result of the stent’s under expansion, the non-expanding narrowing was post-dilated at 20 atm. pressures with a 3.5 × 10 mm non-compliant balloon. The proximal optimization technique (POT) for the proximal segment of the LMCA done using a 4.0 × 8 mm balloon at 16 atm was employed. To prevent the slow-no flow phenomena, which could establish the TIMI 3 flow, intracoronary nitroglycerine and sodium nitroprusside were injected.
The patient was shifted to an acute medical care unit where the non-invasive ventilation continued for 24 h. As part of the medical stabilization, intravenous diuretics, and nitroglycerine, low-molecular heparin were employed. The patient recovered well after the procedure with a reduction in ischemic changes (Figure 1B) and was discharged on the second day on dual antiplatelet treatment, carvedilol, perindopril, eplerenone, empagliflozin, long-acting nitrates, and high-dose statins. He has completed his 6-month follow-up with no more symptoms.
Discussion
After CABG, it is well-established that atherosclerosis progresses more rapidly in segments proximal to severe luminal stenosis, in grafted coronary artery segments, and in normal segments between high-grade stenosis and the anastomosis site. 4 In a 1994 study, Weintraub et al. examined the long-term rate of re-operative CABG and PCI after CABG, finding that the 5-, 10-, and 12-year freedom from CABG or PCI was 96, 81, and 69%, respectively. The reported annual frequency of interventions has increased over time, and it is now significantly higher in younger people. These findings highlight the ultimately palliative role of coronary artery revascularization. 5 Re-operative CABG may not always be successful due to factors such as inadequate revascularization, graft failure, and the development of stenosis in the native coronary arteries (CABG). Redo of CABG or PCI may need to be performed on the patient again if any of the aforementioned concerns arise. 6
The PCI for LMCA stenoses, both unprotected and protected, has become increasingly popular due to recent advancements in interventional technology. Currently, PCI for the treatment of protected LMCA disease exhibits greater mortality and major adverse cardiac events (MACE) rates compared to PCI for other coronary lesions. However, it could potentially serve as a feasible alternative for patients requiring a repeat bypass procedure. 7 Re-operative CABG (n = 1561) and PCI (n = 2613) were compared in patients from Emory University Hospitals who had prior CABG, and the results were analyzed by Weintraub et al. The hospital mortality rate was reduced (1.2% vs. 6.8%) after angioplasty compared to repeat CABG (P.0001), however, there were more repeat interventions performed after PCI. 6 Percutaneous interventions on protected and unprotected LMCA stenosis utilizing PTCA and other interventional devices are described by Keeley et al. along with the immediate and 7-year outcomes of 273 patients (1.3%) out of 21,271 interventions performed between the period of 1990−1907. They found that out of 219 procedures for protected LMCA stenosis, 142 were elective and 32 (0.15%) were defined emergency interventions like our case. 1 Acute LMCA blockage has also been shown to have a deleterious influence on long-term survival; however, this is an extremely uncommon occurrence in 0.15 % of patients who have already had CABG (protected LMCA occlusion) while 0.8% of primary PCI cases are attributed to acute unprotected LMCA occlusion.1, 3, 6
A patient with a complex surgical cardiac history who had undergone CABG using a modified Cabrol type anastomosis with SVG conduits to two coronary arteries suffered recurrent acute coronary syndrome (ACS), as reported by Sabah et al. After coronary angiography revealed significant stenosis in the Cabrol-type SVG grafts, they opted for a protected PCI with Impella support. 8 Since LMCA lesions frequently exhibit aorto-ostial involvement and large, calcified, eccentric plaques, the efficacy of routine PTCA is often compromised. This has led to the widespread routine use of cutting-edge interventional devices like stents, atherectomy, and lasers. 1 PCI of protected LMCA is associated with good short-term results, but it has serious long-term consequences such as an increased risk of myocardial infarction, CABG, and death. 9 As a result, regardless of whether or not they are suffering symptoms of recurrence of the ischemic events, patients who have undergone PTCA of the LMCA should be evaluated with a stress test or non-invasive imaging techniques such as computed tomography angiography at least once a year.
Our case showed an interesting revelation, namely the existence of occlusion in the protected LMCA. This particular manifestation of ACS as a posterior wall myocardial infarction (ST-segment myocardial infarction) is considered to be uncommon. Moreover, utilizing CT-CAG, it was demonstrated that there was a reverse flow of blood from the LIMA to the LAD graft across the two severe stenoses of the proximal LAD and LMCA bifurcation. The identification of these features resulted in a delay in the diagnosis, despite the occurrence of anginal attacks for the past 15 days. Subsequently, the critical stenosis of the LMCA bifurcation got occluded, resulting in the onset of ACS. Performing primary PCI on the protected LMCA is an infrequently conducted procedure.
Conclusion
The acute occlusion of the protected LMCA is a very rare cause of ACS in a patient with prior CABG. The primary PCI performed in an emergency may preclude the use of imaging tools and modern intervention tools for the plaque modifications, recurrent ischemic events should be watched for on a regular basis.
Authors’ Contributions
PJ and GPK are the primary physicians of the case. PJ collected data, and drafted the manuscript while GPK collected images and edited the manuscript. KCM is involved in the intensive care management of the case. AJ rendered her contribution towards manuscript preparation and English language editing.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Consent for publication was obtained from all participants.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Yashoda Hospitals and in accordance with the Declaration of Helsinki.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Consent from Patient / Patient’s Attender
As a corresponding author, I declare that there is no financial or non-financial conflict/competing interests. This manuscript has not been submitted to any journal before for publication as a part or complete version. I give complete consent and rights to the journal for its publication. Informed consent was obtained from a participant included in the study. All procedures performed in studies involving human participants were by the of ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.