
Abstract
There are only a few case reports of iatrogenic compression of left circumflex during mitral valve surgery. We encountered 2 such incidences which were successfully managed with timely percutaneous intervention. The possible mechanisms causing this tricky complication and tips to avoid it are discussed in this report.
Introduction
Mitral valve (MV) surgical repair is the procedure of choice for the treatment of severe mitral regurgitation (MR), particularly in leaflet prolapse. Annuloplasty procedures, with rings or bands, enable remodeling of the mitral annulus to adequate size and shape, enhance the coaptation area, and prevent further dilatation. These surgical procedures have become popular in the modern era and are preferred over the valve replacement. However, the proximity of the left circumflex coronary artery (LCx) to the mitral annulus, especially near the anterior commissure, places this artery at a risk of injury during MV surgery. There are a few reports in the literature reporting such occurrence both during mitral replacement and repair.1, 2 Herein, we report 2 cases of iatrogenic circumflex Cx stenosis following MV repair surgery which could be successfully tackled by prompt percutaneous intervention (PCI) in our institute.
Case Reports
The first patient was a 55-year-old man who had severe MR due to prolapse of both leaflets. Preoperative coronary angiography showed left dominant circulation with normal coronaries (Figure 1A). The patient underwent mitral annuloplasty (30-mm Carpentier-Edwards ring [Edwards Lifesciences Corporation, U.S.A]) by means of minimally invasive right thoracotomy through the right fourth intercostal space. During surgery he developed transient complete heart block. After the procedure as soon as he reached the intensive care unit, he developed an episode of ventricular tachycardia which was reverted by direct-current shock (200 J). The postshock electrocardiogram (ECG) showed inferolateral ST-segment elevation myocardial infarction. Echocardiogram showed inferolateral dyskinesis of the left ventricle with mild left ventricular systolic dysfunction. Emergency CAG (Coronary Angiography) revealed acute occlusion of the circumflex Cx. Percutaneous angioplasty and stenting (Xience v stent, 4.0 × 18 mm) was performed with optimal result (Figure 1B). Clinical status and ECG changes settled, with no further arrhythmias. This patient is doing well for last 1 year after discharge.
Presurgical Coronary Angiogram Showing Normal Circumflex Artery in Case 1

Coronary Angiograms After the Surgery Showing the Lesion in Circumflex Artery and Post-PCI Result in Case 1

Presurgical Coronary Angiogram Showing Normal Circumflex Artery Arising from RCA in Case 2

The other patient is a 45-year-old man who had severe MR due to prolapse of PML with preoperative coronary angiography showing normal coronaries with anomalous origin of LCx from right coronary artery (RCA; Figure 2A). The patient underwent mitral annuloplasty (32-mm Carpentier-Edwards ring) by means of median sternotomy. On the first postoperative day, he developed retrosternal chest discomfort. ECG showed ST elevation in V3–V6 (Figure 3). Echocardiogram showed inferolateral dyskinesis of the left ventricle with mild left ventricular systolic dysfunction. CAG was done which revealed a subtotal occlusion of the circumflex Cx. Ad hoc percutaneous angioplasty with stenting (Xience alpine, 2.75 × 18 mm) was performed with good result (Figure 2B). ECG changes settled promptly and the patient was asymptomatic at a 3-month follow-up.
Coronary Angiograms After the Surgery Showing the Lesion in Circumflex Artery, Arising from RCA and Post-PCI Result in Case 2

Preoperative and Postoperative ECGs Showing Inferolateral MI Picture in Case 2

Discussion
Our 2 cases described above have clearly demonstrated the development of occlusion of LCx with significant ischemia following MV repair surgery. We could detect the problem in time and successfully bail out on both occasions with timely coronary angioplasty. Iatrogenic injury to circumflex artery during MV surgery is not uncommon with a few cases being reported since the first report of LCx compression following MV replacement by Danielson et al in 1967. This sequel is rare but can happen even in centers with considerable experience in MV surgeries (both repair and replacement) and the reported incidence is from 0.5% to 1.8%.1-11
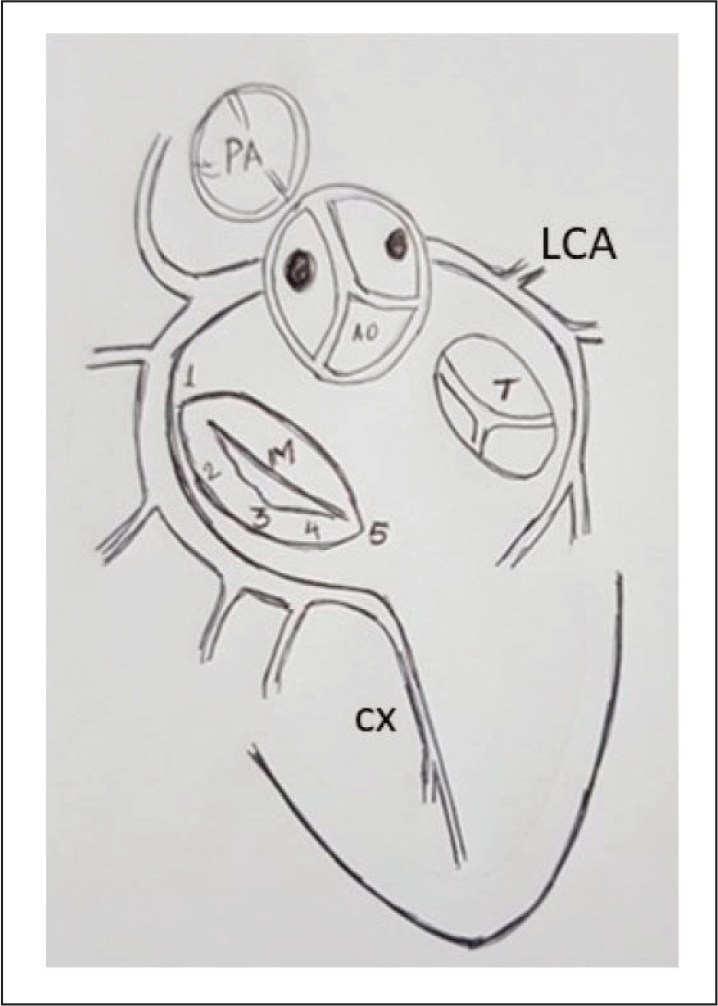
5 Imaginary Points on Mitral Valve and the Relation to the Circumflex Artery When Seen by a Surgeon
Anatomical Basis
Pessa et al suggested 5 imaginary points (Figure 4) on MV when seen by a surgeon: number 1 is at the level of the anterior commissure, 5 at the level of the posterior commissure, and the other 3 points are equidistant from these 2 extremes. The shortest distance between these structures was observed in the area of the anterior commissure. 12 Virmani et al asserted that injury to the Cx is highest in dominant left coronary system and in balanced networks. Virmani et al measured distances of 3–7.5 mm between the Cx and the mitral annulus in balanced or left-dominant networks, and a distance always more than 5 mm in right-dominant networks in the 15 hearts studied. 4 Cornu et al showed that in right dominance the Cx lies at an average distance of 8 mm from point 1 and a 5 mm average distance from point 4; in a balanced network, the Cx lies at a 4.5 mm average distance from point 1 and at a 3.5 mm average distance from point 2. 13
Kaklikkaya and Yeginoglu proposed that the proximal LCx is at the greatest risk because the distance from that part of the artery and the MV annulus is only 2.3 mm in the left-dominant pattern, whereas the mean distance is 5.1 mm in the right dominant system and 3 mm when the pattern is balanced. 14 In a review of all previous cases, Hilltrop found left dominance in 69% and balanced circulation in 19%. 1 of the 4 cases reported by Hilltrop had a left dominant system with the anomalous LCx taking a retroaortic course originating from the right sinus. Our second case had a similar anatomy as the above-cited patient. 2 However, the occurrence in some cases is not fully explained by these anatomical mechanisms.
The mechanisms of injury of the Cx, independent of anatomical pattern are as follows:
Fixation suture that completely encircles and occludes the artery Suture that passes through and completely obliterates the artery Vascular distortion or a large quadrangular resection that causes dynamic or fixed occlusion Laceration of the artery that results in localized hemorrhage Subintimal hematoma, coronary spasm, thrombotic occlusion due to laceration of the endothelium Introduction of an air embolus into the RCA. Air embolism usually causes only transient ischemia, but in a few cases it can cause a myocardial infarction Heavy calcifications beyond the valve leaflets (into the annulus and myocardium) The use of a large ring (≥ 30 mm) can contribute to vascular distortion.
2
Presentation
The clinical manifestations of these ischemic lesions can be very diverse and depend upon the type of injury (partial, dynamic, or complete coronary occlusions), the Cx affected, the site of the injury to the artery, and preoperative myocardial reserve. The onset of symptoms is typically reported immediately (intraoperative to a few hours postoperative).
A presentation may include (a) the inability to be weaned from extracorporeal circulation, (b) refractory ventricular arrhythmias, (c) ST-segment elevation, and cardiac-enzyme elevation, (e) echocardiographic evidence of the left ventricular segmental wall motion abnormalities, or (e) persistent hypotension. 15
Treatment and Prevention
The paucity of reported cases does not permit to define the best treatment modality (surgery vs PCI). Surgical treatment is MV reintervention (exploring the MV, partially or completely, and removing the ring or band; Relocating the sutures toward the leaflets, passing them more superficially near the anterolateral commissure and the P1 and P2 segments, simply removing the presumable culprit sutures, or Cx bypass grafting in some cases).
The intraoperative use of TEE (Trans Esophageal Echocardiography) enables the visualization of abnormal segmental wall motion and the rapid diagnosis of an ischemic lesion. Intravascular ultrasound imaging can also help clarify the nature of an obstructive lesion in the circumflex artery.
The alternative to surgery is PCI (with or without a stent) and is particularly useful when the patient is relatively stable or when the diagnosis is made after leaving the operating room. If the vessel is only partially occluded, it is generally a straightforward procedure with high success rates. It is possible that the suture yields to high pressure balloon dilatation facilitating successful stent deployment. Correction of vessel distortion following surgery may be another mechanism of relief from ischemia. Some authors advocate that the spatial anatomy of the Cx and MV annulus by conventional angiogram or by MDCT (Multi Detector Computed Tomography) should be made mandatory before MV surgery to prevent this potential complication.
Conclusion
No large case series exist and there is no consensus as to which subset of patients is at increased risk. Monitoring of ECG and the use of intraoperative TEE looking for new RWMA is paramount to ensure a timely diagnosis. Increased awareness of this potential sequel, proper presurgical evaluation and meticulous surgical technique should further help avoid LCx injury in patients undergoing MV surgery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.