
Abstract
May-Thurner syndrome/Cockets syndrome/ileocaval syndrome is a rarely diagnosed, anatomical and pathologically variable condition, causing venous flow obstruction in iliocaval territory. We report a case of 64 year old male patient who presented with unprovoked proximal deep venous thrombosis (DVT) of left lower limb. Evaluated for hypercoagulable state, which was negative, the patient underwent catheter guided thrombolysis and anticoagulation for 6 months. Two years later, he developed left lower limb swelling, and venous doppler revealed acute DVT; CT venogram was consistent with left common iliac vein compression by right common iliac artery suggestive of May-Thurner syndrome. Catheter-guided thrombolysis was done, and percutaneous transluminal peripheral angioplasty/stent was placed from inferior vena cava to left common iliac vein. This case highlights the importance of high index of suspicion in managing patients with DVT for possible ileocaval syndrome wherein anticoagulation alone is insufficient and needs more aggressive and definitive treatment to relieve the obstruction and to prevent recurrence.
Introduction
May-Thurner syndrome (MTS) is a venous outflow obstruction disorder characterized by compression of the left common iliac vein by an overriding right common iliac artery. MTS primarily affects young to middle-aged women, although many patients remain entirely asymptomatic. 1 Anatomic variations of MTS, though uncommon, have been described. Treatment usually involves endovascular management, including thrombolysis and/or thrombectomy with or without inferior vena cava (IVC) filter placement, followed by angioplasty and stenting of the left common iliac vein.
Case Report
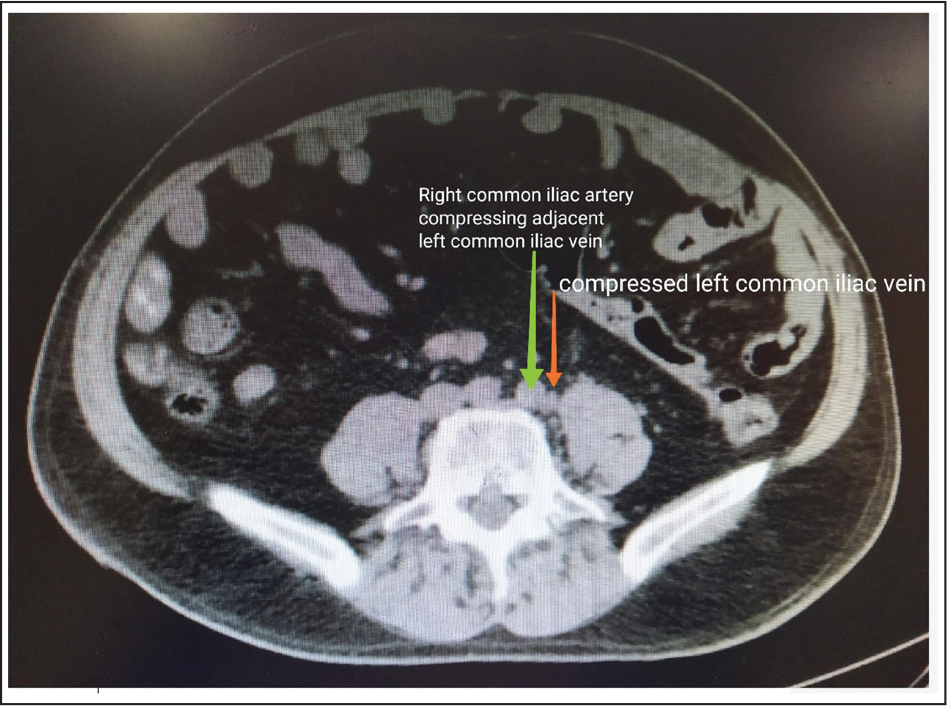
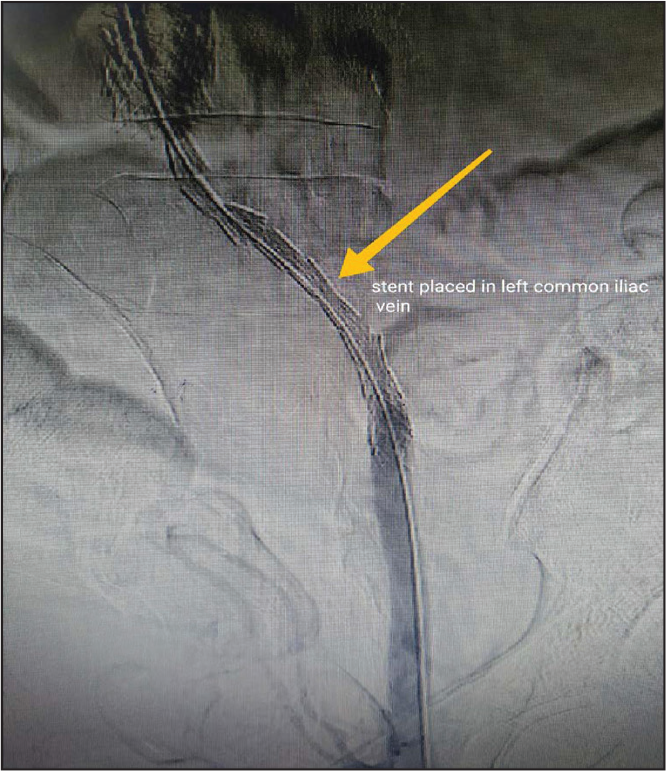
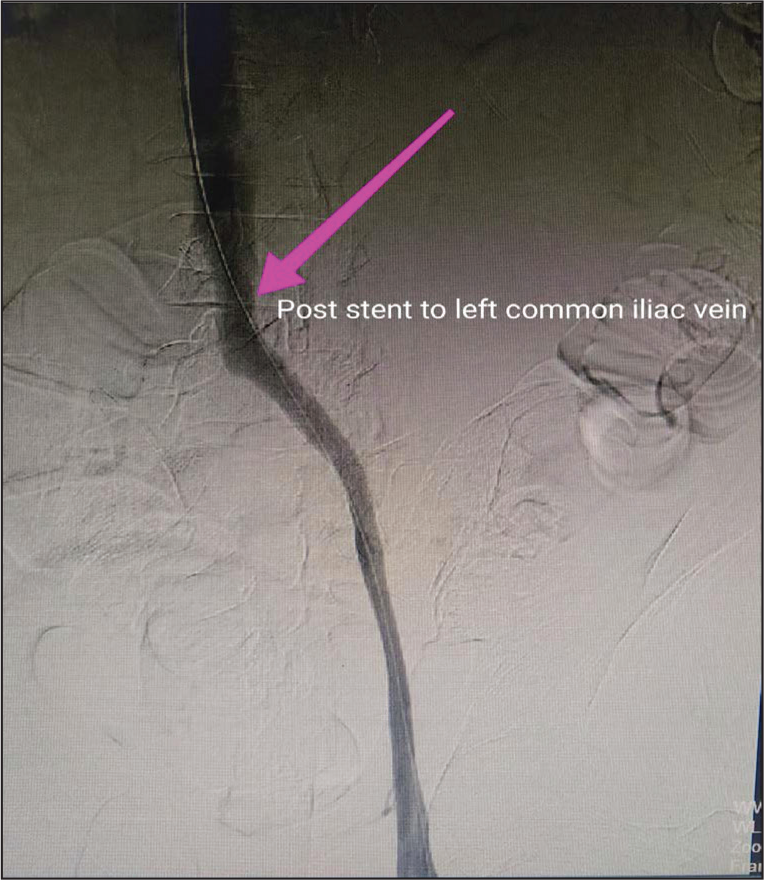
64 year old male initially presented to us in April 2017 with history of left lower limb swelling since 3 days, associated with dull throbbing pain in the left lower limb started in left foot and radiating to thigh, and difficulty in walking since 3 days, with no history of dyspnea, chest pain, trauma, or immobility. Clinical history did not reveal any risk factors for deep venous thrombosis (DVT). Past medical history of gout since 2009, right TKR (total knee replacement) (2009), Type II DM on treatment with antidiabetics and antigout medications. No significant family history. On examination his vitals were stable, there was unilateral swelling of left lower limb with local rise of temperature, and peripheral pulses were palpable. Systemic examination was unremarkable. Basic workup including CBP (complete blood picture), metabolic panel, chest X-ray, and coagulation profile were within normal limits. EKG, 2DEcho were normal. Patient had elevated D-Dimers (1790 ng ml–1). Considering possibility of DVT, lower extremity venous doppler was done which revealed partial luminal thrombus in left external iliac, common femoral, and superficial femoral vein, great saphenous vein showing echogenic thrombus in its distal end. Ultrasound (USG) abdomen with color doppler revealed partial luminal thrombus of left common iliac and external iliac veins. Workup for the cause of DVT was done as there was no identifiable precipitating factor. Homocysteine levels were 13.2 µmols L–1, Protein C, Protein S, Antithrombin III were normal, anticardiolipin antibodies were negative. A diagnosis of unprovoked proximal DVT was made and patient underwent catheter guided thrombolysis with tenecteplase followed by infusion for 24 hours and later he was treated with (rivaroxaban 15 mg twice daily for 21 days followed by 20 mg once daily for 6 months). He was under regular follow-up. In September 2017, the follow-up scan revealed no evidence of thrombus. In June 2019, patient again presented with history of left lower limb swelling since 4 days, with no precipitating event being identified. His vitals were stable .CBP and metabolic panel were normal. Venous doppler revealed left external and internal iliac vein thrombosis. Further evaluation with CT venogram showed significant stenosis and narrowing of left common iliac vein, subacute thrombus in left distal external and internal iliac veins with dilated luminal caliber, possibly MTS. Patient underwent catheter-guided thrombolysis with tenecteplase (20 mg) followed by tenecteplase infusions for next 24 hours. Through left popliteal vein approach, lesion identified and predilated with 4.0 × 100 mm balloon, and 16 × 100 mm sinus-OptiMed drug eluting stent from IVC to left common iliac vein was placed and post stent dilatation was done with 10 × 30 mm balloon and 7.0 × 100 mm cook balloon. Sinus OptiMed stent was used in view of good radial force compared to closed cell Nitinol stents and open cell design for good vessel adaptation. Good results were obtained with no procedural complications. Rivaroxaban (15 mg twice daily for 21 days followed by 20 mg once daily for 6 months) was started. He is under regular follow-up with no new symptoms till date.
CT Venogram Image Showing Right Common Iliac Artery Compressing Left Common Iliac Vein
Peripheral Angiography Image Showing Severe Stenosis of Left Common Iliac Vein

Showing PTPA and Stenting From IVC to Left Common Iliac Vein
Showing Post-PTPA and Stenting From IVC to Left Common Iliac Vein
Discussion
MTS refers to chronic compression of left common iliac vein against lumbar vertebrae by overlying right common iliac artery with or without DVT. 2 Cadaveric and CT studies show prevalence of MTS to be around 25% with majority of patients being asymptomatic. 3 Symptomatic patients account for 2% to 3% of patients presenting with symptoms of venous hypertension, DVT, venous claudication, chronic venous insufficiency, and rarely pulmonary embolism. 3
The majority of cases follow the classic left-sided description, but other variants have been reported, such as right-sided MTS and compression of the IVC by the right common iliac artery, concurrent compression of the left iliac vein, right iliac vein, and IVC by the right iliac artery. 4 The reason behind left-side predominance being the left CIV has a more transverse course and is predisposed to compression, whereas the right CIV ascends more vertically and is therefore not similarly predisposed.
The presence of a spur, possibly from injury to the vein endothelium from the arterial pulsations, is believed to cause deposition of elastin and collagen in iliac vein, leading to intimal proliferation, forming spur, which predisposes to the development of DVT. MTS is estimated to be 3 times more common in females.
Risk factors for MTS include female gender, particularly postpartum females, use of oral contraceptives, individuals with spinal abnormalities, or prior aortoiliac vascular stent placement (acquired form of MTS). 5
Clinical presentation in majority of individuals with MTS anatomy is asymptomatic, but progression of the venous lesion can occur, causing symptoms related to venous hypertension. Clinical presentations of symptomatic MTS include, but are not limited to, acute extremity pain and swelling, venous claudication, or chronic development of symptoms/signs of venous insufficiency (ie, edema, skin discoloration, or skin ulceration).
A diagnosis of MTS may be suspected based upon clinical features and initial diagnostic testing, typically duplex ultrasound. A definitive diagnosis requires demonstration of the stenotic or occlusive venous lesion on vascular imaging. For patients suspected of having MTS, advanced noninvasive venous imaging CT or MR venography should be obtained first to make the diagnosis. The definitive diagnosis is established with invasive venous imaging after removal of the thrombus. Venography can help identify 3 common angiographic patterns in MTS. These include (a) focal stenosis or collateralized short-segment occlusion of the left common iliac vein, (b) acute iliofemoral venous thrombosis with the underlying lesion revealed after successful thrombolysis, and (c) chronic isolated thrombosis of the left common and external iliac veins with collaterals arising from the common femoral vein. Intravascular ultrasonography (IVUS) and hemodynamic pressure measurements are also useful for confirming an MTS diagnosis. In particular, IVUS has been recognized for its invaluable role in stent selection, deployment, and evaluation.
Definitive management of MTS is aimed at (a) resolution of thrombus, (b) recanalization of occluded venous segments, and (c) maintenance of patency of iliac vein by balloon dilatation and stent placement. Endovascular management remains the first line of treatment for MTS. 6
It is important to consider MTS in patients who have no other obvious reason for hypercoagulability and who present with recurrent lower limb thrombosis. Failure to correct anatomical substrate of MTS could lead to recurrent DVT, and to additional complications including pulmonary emboli, chronic venous stasis, and iliac vein rupture which increase further morbidity and mortality. Our patient did not have any evidence of hypercoagulability; he turned out to be a rare case of MTS in a male patient.
Conclusion
This case highlights the importance of the need for high index of suspicion for MTS as systemic anticoagulation is insufficient and patient needs more aggressive and definitive treatment in the form of endovascular stent placement to prevent recurrent thrombosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.