
Abstract
Background:
American Indian (AI) persons with advanced cancer (PwAC) in South Dakota have seen increased rates of cancer incidence and mortality compared to national rates. These inequities are driven by social determinants of health. Providing early palliative care is highly important for rural PwAC but is sparsely available in rural South Dakota.
Objective:
To explore cancer care experiences and patient symptoms and caregiver burden among AI and rural PwAC, and their family caregivers (FCGs), to understand the barriers and opportunities for adapting an early palliative care intervention.
Design:
Descriptive study design reporting on the qualitative and quantitative data collected.
Methods:
PwAC and FCG participants were recruited from a rural healthcare facility delivering cancer care and serving AI tribal and rural/frontier populations. Quantitative data were collected using online surveys to discover symptoms and caregiving burden among PwAC (n = 18) and FCGs (n = 12), respectively. These participants were invited to semi-structured interviews to elicit perspectives of rural cancer care delivery (n = 11 PwAC and 8 FCGs).
Results:
PwAC experience moderate symptom burden with 83.3% lacking energy, 77.8% feeling drowsy, and 72.2% feeling pain. FCGs experience high caregiver burden across all three subscales of the caregiving scale. Qualitative analysis found an overarching category of “Healthcare Fragmentation Amplified by Living in a Rural/Frontier Location” with three underlying codes: “Being Seen and Heard: Value-Based Connection to Distant Resources,” “Facilitating Decision Making from Afar,” and “Problem Solving Skills and Solutions.”
Conclusion:
This study demonstrates that rural cancer care is challenged by multiple factors, including fragmented healthcare, lack of healthcare infrastructure, and vast travel distances. This greatly impacts PwAC and FCG’s ability to feel seen and heard, make decisions, and problem-solve. Supportive programs designed for the local rural context are imperative to improve the quality of life for rural PwAC and their FCGs.
Plain language summary
People living with advanced cancer in rural and frontier areas often face unique challenges when trying to get the care and support they need. In South Dakota, many people live far from cancer and palliative care services especially American Indian individuals. This can affect their health, quality of life, and overall experience with healthcare. Family members and loved ones who help care for someone with advanced cancer may also experience high levels of stress and burden. This study explored the experiences of people with advanced cancer and their family caregivers who live in rural/frontier areas of South Dakota. We asked participants to do surveys about symptom/caregiving burden and invited them to take part in interviews to share their experiences in their own words. Eighteen people with advanced cancer and twelve family caregivers completed surveys, and nineteen people participated in interviews. People with advanced cancer reported symptoms such as low energy, drowsiness, pain, and difficulty sleeping. Many also worry about their illness and future. Family caregivers reported high levels of burden, including emotional stress, strain on daily life, and challenges within their relationships. Participants described how living in a rural or frontier area made cancer care more difficult. Long travel distances, limited local services, and lack of coordination between healthcare providers often made people feel unheard and unsupported. Participants described having to make complex medical, financial, and personal decisions from afar, while also solving practical problems such as travel costs and missed work. Overall, this study shows that people with advanced cancer and their caregivers in rural and frontier areas face significant challenges that affect their quality of life. These findings show the need for palliative and supportive care programs that are designed specifically for rural communities and reflect local resources, culture, and needs.
Introduction
While the national cancer incidence rates have been steadily declining, rates have been continuing to increase in South Dakota (SD) 1 with SD also experiencing a higher cancer mortality rate than the nation. 2 For American Indians (AIs), national cancer incidence and mortality rates are lower than overall national cancer rates.1,2 However, AIs in SD experience great cancer disparities, with an incidence rate 1.2 times higher than the national rate for all races and 1.4 times higher than the national AI cancer incidence rate.1,2 Increased incidence rates leave AI and rural persons in SD at risk for cancer care inequities that are driven by social determinants of health, including socioeconomic, cultural, geographic, and environmental factors. 3 These factors are also highly influenced by rurality. 4 Over 50% of SD residents live in rural and frontier areas, 5 and 95% of SD counties are categorized as rural or frontier, which are known to be resource-constrained and have complex factors affecting health outcomes. 6 Furthermore, the ten poorest counties in SD are classified as rural/frontier, and are a part of/adjacent to one of the nine federally-recognized AI tribes in SD that have poverty rates between 22% and 48.6%, all of which are classified as rural/frontier counties. 6
Rurality also impacts how advanced cancer is at diagnosis, with cancer more often being diagnosed at later stages in rural areas. 7 Cancer mortality rates are also higher in rural areas, which also tend to have an older population with more comorbidities, physical and mental. Major cancer care challenges in rural areas include healthcare workforce shortages, geographical barriers and isolation, and more underinsured/uninsured individuals. In SD, nearly half of cancers are diagnosed at regional and distant stages; 55% for AIs and 40% for whites. 8 Furthermore, oncology clinical practice guidelines recommend early palliative care for patients diagnosed with advanced cancer, which includes hematologic malignancies. 9 However, providing oncology care for rural populations that is consistent with the guidelines is stifled by limited palliative care services at the state, national, and global scale.10–12 Providing early palliative care to patients with advanced cancer is of utmost importance to address their high likelihood of symptom burden. 13 Furthermore, family caregivers (FCGs) of persons with advanced cancer (PwAC) often experience burdens when informally providing care for these patients. 14
The vision for our work is to improve the quality of life for those living with advanced cancer in rural or frontier areas of the Great Plains region. To achieve this vision, the purpose of this study was to better understand rural cancer care from the perspectives of rural PwAC and their FCGs. This study addresses the critical gaps in the literature by examining how worsening cancer incidence and mortality rates intersect with limited access to palliative care in rural and frontier settings to inform interventions that address the challenges to high-quality care. 15
Methods
Design
Data collected for this cross-sectional descriptive study occurred between July 2022 and April 2023 with the purpose of better understanding the cancer care experiences, including the greatest challenges and needs, of PwAC and their FCGs through semi-structured interviews. To elicit objective measurement of socio-demographic and burden faced by this population, surveys were also administered.16,17
Setting and participants
Participants (PwAC and FCGs) were recruited from a rural healthcare facility delivering cancer care with a 100% rural/frontier service area. This facility is led by advanced practice providers in conjunction with oncologists at an urban facility and does not offer palliative care services. While there is access to non-specialty allied health professions, specialty palliative care services are 170–225 miles away from the facility. Participant ZIP code was collected to ensure they lived in a rural/frontier setting. For this study, rural was defined as rural-urban commuting area (RUCA) codes 4–10. 18 Furthermore, it is important to note that the area is also classified as frontier and remote level 2–4. 19 This facility also provides service to several AI tribes in the region.
Two pools of participants were recruited for this study, PwAC and FCGs. PwAC eligibility criteria were: (1) age 18 years or older, (2) diagnosed with Stage 3 or 4 cancer or hematologic malignancy, and (3) English-speaking. FCG eligibility criteria were: (1) age 18 years or older, (2) serving in a FCG role for a PwAC, and (3) English-speaking. Exclusion criteria for PwACs and FCGs included: (1) Self-reported mental illness (i.e., schizophrenia, bipolar disorder, or major depressive disorder), dementia, active suicidal ideation, uncorrected hearing loss, or active substance abuse. Potential participants were asked if they were experiencing any of these conditions to ensure they could participate fully in the study (i.e., for those with uncorrected hearing loss) and to limit the risk of exacerbating any existing mental illness. However, no potential participant self-reported any of these characteristics. PwACs did not need to have an identified FCG to participate in the study. Likewise, FCGs were eligible to participate even if the person they provided care for did not want to participate.
Advanced practice and registered nurses at the facility were educated on the study’s participant eligibility criteria and informed eligible PwAC and FCGs about the study. The facility had an iPad that was populated with a link to an online digital interest form for PwAC and FCGs to complete if they were interested. After completion of the interest form, the research team reached out to the interested person to confirm eligibility. Participants received a $50 gift card incentive for the interview and survey; participants completing both received $100.
Data collection
Qualitative data collection
Qualitative data were collected via semi-structured interviews using Zoom (without video) or by telephone using an interview guide (Table 1) to identify challenges and needs related to rural cancer care from the perspective of PwAC and their FCGs. All questions in the interview guide were asked to each participant to ensure all questions of interest were asked, with follow-up questions as indicated in each interview. PwACs had the opportunity to interview as a dyad with their identified FCG, or they could interview alone. For those who interviewed as a dyad, each question was asked, and both PwAC and FCG were asked to contribute to the discussion. Of the 11 PwACs, 8 were interviewed as a dyad with their FCG, 3 PwACs were interviewed individually, and 1 FCG was interviewed individually. Each interview was audio recorded and lasted 30–75 min and participants were no longer sought for inclusion after reaching thematic saturation, and no new ideas were being heard during participant interviews. Interviews were transcribed verbatim by a professional transcription service and verified for accuracy with the original recording file by a member of the research team. Digital recordings were destroyed after verification of accuracy was complete.
Interview guide.

The corresponding author (B.V., PhD, RN, CCTC, CNE®, CHPN®, FPCN® – male ) is a doctorally prepared nurse faculty member with an advanced qualitative methodology research background, experience with working with AI persons in research studies, is experienced in palliative care research, is a Certified Hospice and Palliative Nurse, and grew up in a frontier community in SD. One other member of the research team was involved in interviewing participants (S.M., PhD, RN, CHPN, CNE – female). The first author, S.M., is a doctorally prepared nurse faculty member with experience with rural and underserved cancer research, experience with AI persons in research studies, is experienced in palliative care research, is a Certified Hospice and Palliative Nurse, and grew up in a frontier community in SD. B.V. and S.M. conducted the first interview together to test the interview guide; subsequent interviews were conducted based on the researcher’s availability.
Quantitative data collection
To provide more context to the qualitative data, we collected quantitative data to measure symptom and caregiving burden, as well as demographic data. Due to small sample sizes, these quantitative data are only descriptive in nature.
Socio-demographic and patient and FCG context
All participants (PwAC and FCGs) were asked to provide sociodemographic information such as age, gender identity, race and ethnicity, zip code, Veteran status, cancer type and stage, cancer recurrence, marital status, highest level of education, current employment status, yearly household income, home internet access, religious preferences, and self-reported health rating. In addition to these data, PwAC were asked if they had completed an advance directive. FCGs were asked the nature of the relationship to the PwAC, if they live with the person (if not, how far away do they live), duration of providing care, average days per week of providing care, and average hours per day providing care. This information was obtained via a survey either with paper/pencil, or online via REDCap,10,11 depending on their preference. The survey for PwAC included questions related to symptom burden, while FCGs included questions related to caregiving burden.
PwAC instrument – Condensed Memorial Symptom Assessment Scale
The Condensed Memorial Symptom Assessment Scale (CMSAS) is a 14-item inventory that measures 11 physical symptoms (fatigue, lack of appetite, pain, dry mouth, weight loss, feeling drowsy, dyspnea, constipation, difficulty sleeping, difficulty concentrating, and nausea) on a five-point Likert scale, and three psychological symptoms (worrying, feeling sad, and feeling nervous) on a four-point Likert scale. 20 The CMSAS measures symptoms that occurred during the past week. The instrument provides a total (CMSAS-SUM) score (range 0–56) and two subscale scores, one for physical symptoms (CMSAS-PHYS; range 0–44) and one for psychological symptoms (CMSAS-PSYCH; range 0–12). Higher scores indicate greater symptom severity, frequency, and distress. The reliability of the CMSAS-SUM, CMSAS-PHYS, and CMSAS-PSYCH subscales has been reported as 0.85, 0.82, and 0.72, respectively. 20
FCG instrument – Montgomery Borgatta Caregiver Burden Scale
The Montgomery Borgatta Caregiver Burden Scale (MBCBS) is a 14-item, five-point Likert scale inventory that measures objective burden, relationship burden, and stress burden. This instrument provides a total score (range 14–70) and three subscale scores for objective burden (MBCBS-OB; range 6–30), relationship burden (MBCBS-RB; range 4–20), and stress burden (MBCBS-SB; range 4–20). MBCBS-OB includes six items and measures the extent to which the FCG relationship impacts observable aspects of the FCGs’ lives, such as a decrease in time for self and others. Cronbach’s alpha for MBCBS-OB in previous studies ranges from 0.88 to 0.91. 21 MBCBS-RB includes five items that measure the degree to which the caregiving recipient’s behavior is perceived as manipulative or overly demanding. Cronbach’s alpha for MBCBS-RB in previous studies ranges from 0.79 to 0.88. 21 MBCBS-SB includes five items and measures perceived effects of caregiving on personal mental health, such as anxiety and depression. Cronbach’s alpha for MBCBS-SB in previous studies ranges from 0.81 to 0.88. 21
Statistical analysis
Qualitative data analysis
Qualitative data were analyzed using the content analysis approach described by Elo and Kyngäs. 22 Each member of the research team independently read and reread the interview transcripts, using and developing categories and codes to more clearly understand the challenges and needs of AI and rural PwAC and their FCGs. The research team met and compared independent analyses, including categories identified in each transcript and the codes identified within each category. 22 The categories were then aligned for the final read through of the transcripts. The team met once again to resolve any differences in the analysis until consensus was achieved. All coding was completed in NVivo 12 Pro. 23
The dyadic interview transcripts were divided by speaker, the PwAC or FCG, by the transcriptionist, and verified by one of the researchers, B.V. or S.M. While the researcher verifying the transcript was the opposite of the one who conducted the interview, it was clear who was speaking while listening to the audio recording and verifying the correct speakers throughout the transcripts. This fostered the analysis of the transcripts as the researchers could compare PwAC and FCG perspectives between the individual and dyadic interviews.
For the qualitative data, we maintained rigor and trustworthiness as explained by Morse. 24 Credibility was achieved through verbatim participant data transcription, followed by a prolonged immersion with the data, and our in-depth discussions of initial and final categories. Our results are dependable due to our frequent analysis discussions and the independent coding of transcripts using NVivo to use a consistent coding structure. The study could be replicated in another setting, transferability, by following the detailed description of the research methods provided.
Quantitative data analysis
Descriptive statistics were used to find the mean, standard deviation (St. Dev.), minimum (min), and maximum (max) for each variable in each questionnaire. A frequency table containing the demographic data was created.
Results
Eleven PwACs and 9 FCGs completed the interview. Data saturation was achieved after approximately six interviews; however, we completed all scheduled interviews, which resulted in the final sample size. All participants completing interviews also completed surveys. Demographic information for qualitative participants is grouped with the quantitative participants in Table 2.
Demographic characteristics of quantitative participants.
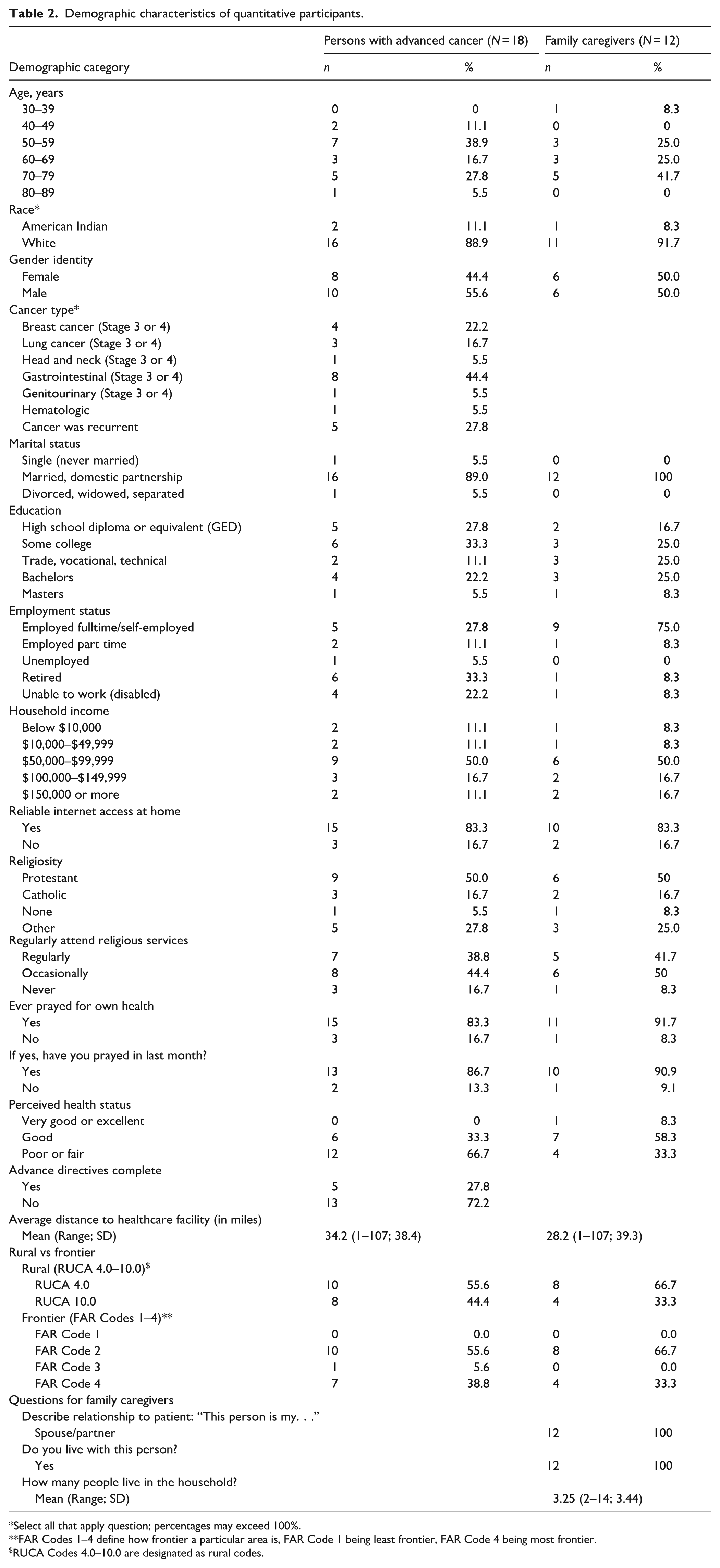
Select all that apply question; percentages may exceed 100%.
FAR Codes 1–4 define how frontier a particular area is, FAR Code 1 being least frontier, FAR Code 4 being most frontier.
RUCA Codes 4.0–10.0 are designated as rural codes.
Qualitative findings
During the semi-structured interviews, PwAC and FCGs openly shared challenges, barriers, and unmet needs of rural cancer care delivery. The overarching category of our analysis is “Healthcare Fragmentation Amplified by Living in a Rural/Frontier Location” with underlying codes identified as “Being Seen and Heard: Value-Based Connection to Distant Resources,” “Facilitating Decision Making from Afar,” and “Problem Solving Skills and Solutions.” All underlying codes are interconnected with the factors of living in a rural/frontier area. The participants who were interviewed as dyadic groups were comprised of spousal pairings only. Because of the homogenous nature of the dyadic interviews (i.e., no opposing views were provided based on what the other party shared, or there was verbal agreement with what was said), further analysis based on dyadic pairs was not conducted. Table 3 includes participant quotes that describe each category and underlying codes.
Descriptive analyses of CMSAS total score and subscales (all persons with advanced cancer and by cancer type).

CMSAS: Condensed Memorial Symptom Assessment Scale; St. Dev.: standard deviation.
CMSAS – higher scores indicate greater symptom distress.
Healthcare fragmentation amplified by living in a rural/frontier location
Fragmentation is a key drawback of the US healthcare system, and is intensified by workforce and healthcare access shortages. 25 The rural and frontier nature of the area where PwAC and FCGs lived demonstrates how this fragmentation is amplified, as it was a pervasive refrain in the interviews. The participants reported having fewer healthcare professionals, treatment options, receiving care across multiple healthcare systems, distance, and the culture of rurality.
Yes, that’s pretty much the biggest influence. It’s just either being at the best or being home. (PwAC 16) . . . if you want a second opinion, you have to travel farther to go get one of those and I didn’t get one of those. I should have but I didn’t. (PwAC 12)
In addition, participants described seeking care from the closest, available healthcare facility for their primary concern, which leads to care across several healthcare systems and from multiple healthcare professionals. These systems and professionals often do not communicate or coordinate well with each other, impacting the PwAC’s ability to be seen and heard, make decisions, and work toward solving their problems.
[There are] so many doctors that it is hard to make sense of where we’re at in any process . . . dropped the ball so many times that it’s heartbreaking, to be real. Not knowing what our options are as far as progression because no one wants to talk about it . . . In our experience, the communication between teams is lacking, and because of that, things like late prescriptions, going without medication, going without any answers on referrals, questions that come up along the way, treatments that have side effects that, “Oh, well, it’s Saturday evening,” so you’re not talking to anybody until at least Monday afternoon. Those needs are our highest priority. (FCG 7) Then, I had an interim doctor and then another interim doctor, and he moved. Then, I had another interim doctor for, I think, two telemeds, and that’s about it. They always had a sort of start from scratch to start treating, and at what had been done, what had worked, what had not, and then try to fit it into a plan for me. (PwAC 17)
An expected sub-category of rurality was distance, as explained by participants who portrayed its impact on all aspects of their cancer journey. Distance affects their ability to see others, including healthcare professionals, family, and friends. This often makes them feel unseen and unheard, isolated as they try to make decisions and problem-solve throughout their journey with cancer.
For some of those people that would be out in the country [living in an isolated area] or even just not get out of their house. . .. (PwAC 9) . . .then you have to basically travel wherever that may be . . . that could be four hours away, that could be two-and-a-half hours away, that could be as far as seven hours away. (FCG 7) Some people who have to go a great distance get here or to the next care center, that the expense and the time of travel and the unpredictability of the weather, you can’t change that. (PwAC 17)
In addition, participants reported how a rural culture of being “tough” influences their care.
Being expected to be a tough, rural woman sometimes which is not. [Laughter] Sometimes we need tender loving care, too. Not everybody is a tough farm wife. (PwAC 13)
Being seen and heard: Value-based connection to distant resources
Participants portrayed how crucial it is to be treated like a human being who is seen, heard, and supported as a whole person throughout the cancer journey. They reported a need for counselors, support groups, and contact with cancer survivors, not available in their rural area. They desire care by a full interdisciplinary team, including spiritual care, who listens to and educates them.
I think, in general, whether it be rural or not, just human contact, human association is really important. (PwAC 18) If you want to see a counselor or a nutritionist or something like that, you sometimes have to travel out of town. . .. (PwAC 12) A support group or something would be really nice to have here. (FCG 2) When he first got it [cancer], we met with the nurses, we met with the social worker, we met with the pharmacist, and we met with a doctor, I think. They all gave us some information and ideas. (PwAC 1) I think it [spirituality] should be approached because this is the time when people start thinking about “What’s going to happen to me?” (PwAC 4) The way they’re treating you like I’m a human and they give me any information I need, even information I don’t need . . . They’re always very happy to treat you like a person and answer all your questions, and I really appreciate that. (PwAC 13)
Being seen and heard was described as creating human connections while interacting with a variety of healthcare professionals. This relates to the category of healthcare fragmentation amplified by living in rural/frontier areas, as PwAC and their FCGs often seek healthcare from several healthcare facilities (providers) because of availability and distance. This is compounded by turnover and shortage of healthcare professionals in rural facilities, which impede continuity of care.
Detriment with the fact that so many of my doctors were here only a short time. (PwAC 17)
Facilitating decision making from afar
Decision making is an ongoing process in which PwAC, FCGs, and healthcare clinicians make frequent, multifaceted decisions through the cancer journey. Participants depicted the multiple and frequent decisions they must make when diagnosed with cancer and throughout the journey. However, they also indicated how living in a rural area impacts their decisions. Treatment decisions were mentioned the most. Deciding where to receive treatment was greatly influenced by how far and which treatments were offered at different locations. Distance also affected their decisions not to start or when they stopped treatments.
. . .it’s like a constant decision-making process over the years of how we’re going to treat it, who we’re going to accept the treatment through, is the treatment worth it with all of the side effects, what can we do to improve quality of life. (PwAC 8) Right away, “This is terminal. It’s everywhere.” At that point, it was decisions, are we going to move to be closer to treatment at Mayo, are we going to stay. . .? Are we going to keep the same doctor that you had? . . .. Are we going to treat this at all? (FCG 7) In the meantime, should we be focusing more on just spending as much time together as we can instead of running from appointment to appointment, down to who we have involved in our lives, honestly. (FCG 7)
They also reported needing to make decisions related to legal and financial matters, planning, and their living situation. Legal and financial matters included powers of attorney, advance directives, and wills. Participants explained how they had to plan for an uncertain future while also planning for the worst-case scenario. Decisions related to living situation entailed if they could live in their current housing situation while experiencing symptoms of cancer and its treatment. In addition, an aspect of planning was setting themselves or their FCG up in a housing situation that allowed them independence.
Being a farmer, I’m a long-range planner and when that [cancer] hit, long-range planning went out the window. [Laughter] I came home and told we got the – together with my two hired men and told them they were going to have to do it because I was going to spend the rest of the summer chasing doctor appointments and I wasn’t wrong, and I didn’t have energy enough to do anything for them in between either. (PwAC 4) . . .do I want to be buried? Do I want to be cremated? All that kind of end-of-life choices. (PwAC 9) The reason why we’re doing it isn’t for me. It would be nice if we get it done before I die. For me, it’s for XXX. Puts everything on one level [single story house]. It’s something that will advance her work and will simplify her life a ton. (PwAC 16)
Problem-solving skills and solutions
Problem-solving skills are essential for PwAC and FCGs to develop practical solutions to overcome their individual barriers and challenges in navigating cancer care with limited resources. Participants referenced the need for problem-solving to navigate their journey with cancer with fewer resources, especially when traveling a distance for treatment and incurring additional costs such as lodging, meals, and gas.
. . .that was really frustrating and confusing and I literally just honestly felt like giving up. This is hard. It’s really hard. Very stressful for a family member to try to get their loved one to these appointments when you financially can’t do it. (FCG 3)
The lack of continuity of care previously described often results in delays in care. Participants reported difficulty in navigating healthcare and accessing care in a timely manner.
The healthcare system is almost like they have gatekeepers set up to try to prevent you . . . to stop you from getting to where you need to be. (FCG 6) Once we got in the door, then we were great, but it was getting in the door. (PwAC 7)
Living in rural and frontier areas while receiving cancer care creates locally context-specific challenges for PwAC and their FCGs, which require problem-solving skills and solutions.
I’ve been thinking about things like this and all the obstacles that could stand in front of a family. These are challenges for us and they’re real challenges . . . So, all I do is I cry a lot and I pray . . . Really takes a lot out, not only emotionally. It drains me as a wife. Really puts my faith to the test every day. (FCG 3)
Quantitative results
Socio-demographic and patient and FCG context results
Eighteen PwAC and 12 FCGs completed the surveys, 44.4% and 50% were female, respectively (Table 2). All FCGs were married or in a domestic partnership with a PwAC participant, leaving six PwAC participants who participated independently. Half of the sample’s households earned between $50,000 and $99,999. The sample was 100% rural. Furthermore, 38.8% of PwACs and 33.3% of FCGs were at the highest level of frontier code (FAR Code Level 4). The average one-way driving distance for PwAC to the healthcare facility was 34.2 miles (range 1–107, SD 38.4), and 28.2 miles one way (range 1–107, SD 39.3) for FCGs. Finally, 27.8% of the PwAC sample had previously completed an advance directive.
CMSAS – Persons with advanced cancer
Table 3 presents the descriptive analyses of the CMSAS. The mean CMSAS-SUM was 17.7 (range 1.6–37.4, SD 10.05), indicating that PwAC overall had a mild to moderate degree of symptom burden, but burden was variable among the physical and psychological subscales, with symptoms being associated with their cancer diagnosis. Table 3 also shows CMSAS scores by cancer type. Among this sample, those with lung cancer (n = 3) had the highest average symptom burden with a score of 26.1. Despite the range in burden, the scores suggest there is burden present in this patient population.
Table 4 presents the symptom frequencies within the CMSAS. Lack of energy (83.3%), feeling drowsy (77.8%), pain (72.2%), and difficulty sleeping (66.7%) were the most prevalent physical symptoms, and worrying (61.1%) was the most common psychological symptom (61.1%).
Frequency of 14 symptoms of the CMSAS.

CMSAS: Condensed Memorial Symptom Assessment Scale; PwAC: persons with advanced cancer.
The frequency and percentages of the responses are based on patients who answered yes to the presence of symptom.
Montgomery Borgatta Caregiver Burden Scale – FCGs
FCG descriptive burden results are in Table 5. FCGs experience a high degree of caregiving burden while caring for PwAC. The mean overall score was 49.25 (range 37–59, SD 6.3). In the objective burden and relationship burden subscales, there were scores that reached the maximum for the subscale, indicating they experience notably high amounts of these types of burden. The mean objective burden is higher than 23, which is considered a “quite high” burden. 26 The mean relationship burden was less than one point lower than the “quite high” score of 15, while the stress burden was three points less than a “quite high” score. 26
Descriptive analyses of Montgomery Borgatta Caregiver Burden Scale – total score and subscales.

FCG: family caregiver; St. Dev.: standard deviation; OB: objective burden; RB: relationship burden; SB: stress burden.
Qualitative and quantitative results integration
As participants of the qualitative portion of the study were also included in the quantitative portion, a few notable findings emerged when comparing the qualitative and quantitative results together. Within the CMSAS, there were high levels of worrying and lack of energy, which was echoed by many participants, especially within “Facilitating Decision Making from Afar.” Many narratives expressing uncertainty of if they should treat the cancer, if they financially can support treatment, or if they have the energy to continuing working and expend the energy needed to “chase appointments” (PwAC 4). The symptom of worrying also manifested throughout in the “Problem Solving Skills and Solutions” area, with participants expressing the emotionally draining effects of cancer treatments and sometimes feeling like giving up may be an easier solution.
Discussion
The purposes of this study were met by gaining a better understanding of rural cancer care, the unmet needs and burden experienced by AI and rural PwAC and FCGs. PwAC and their FCGs both experience moderate to high burden, with the majority of PwAC reporting a lack of energy, feeling drowsy, and feeling pain. The overarching category of “Healthcare Fragmentation Amplified by Living in a Rural/Frontier Location” is described by three underlying codes: “Being Seen and Heard: Value-Based Connection to Distant Resources,” “Facilitating Decision Making from Afar,” and “Problem Solving Skills and Solutions.”
These results coincide with the perspectives of healthcare professionals serving this rural oncology population who identified the barriers to cancer care delivery as access, time, and isolation.27–29 The theme of access aligns with the overarching category of healthcare fragmentation amplified by living in a rural/frontier location. This encompasses many factors that influence the ability of PwACs and FCGs to access cancer care and resources.30,31 In addition to PwAC and FCGs, healthcare professionals in a similar geographic area noted how these factors, especially the lack of healthcare workforce and facilities, impact decision making from diagnosis to death. 27 These quotes related to decision making from afar demonstrate that rural PwAC did not have the privilege of making some decisions because of where they lived.
Within the code of being seen and heard, PwAC and FCGs expressed that time with the healthcare team is limited. In recent work, healthcare professionals also stated that time is a commodity in delivering cancer care, both in terms of time with the PwAC and FCG and time for PwAC and FCGs to make decisions. 27 Future work should aim to not only improve PwAC and FCGs feelings of being seen and heard, but also implement evidence-based practices of active listening, holding silence, and acknowledging individual experiences to improve overall cancer care experiences.32,33
While PwAC and FCGs voiced all the factors that lead to geographic and social isolation, they did not express feeling isolated. The healthcare professionals called out isolation and its effects on this population as a major consequence of living in rural and frontier areas. 27 This discrepancy may be influenced by rural PwAC and FCGs who report having a larger social network than their urban counterparts, even though rural residents face structural barriers to connecting and report higher levels of loneliness. 34 Measuring social isolation and loneliness may be a useful metric to compare rural and non-rural differences in future research.
The descriptive analysis revealed that PwAC experience a mild to moderate level of symptom burden, and their FCGs experience a high level of caregiving burden. These elevated burdens are consistent with prior research exploring PwAC and FCG experience for advance cancer.35,36 Burden in our sample is likely confounded by rurality, especially the driving distance to obtain oncology services at the rural healthcare facility (up to 107 miles one way). After removing those who live within 5 miles of the facility, the average distance to cancer treatment in this study increases from 34 to 68 miles one way. This is higher than findings from other rural cancer studies, where the average is approximately 40 miles, and is supported by a national study on travel times for cancer care, which found that travel times increase with increasing rurality.37–39 This determinant of healthcare access greatly impacts SD, where the majority (57.5%) of counties are frontier. 40 Transportation in rural/frontier areas of SD can be hazardous, especially during the winter months. Furthermore, telemedicine visits may be challenging to complete due to poor internet availability and lack of needed infrastructure. 41 Although 83% of our sample had access to reliable internet, it is unclear if the available internet has adequate data speeds needed to support telemedicine visits.
Although the study findings may be similar to other explorations of cancer care experiences in rural/frontier settings, the approach to addressing these barriers will be different from location to location, based on local resources, cultural influences, state-level government, and other factors. However, our assessment of the barriers and challenges is a necessary first step prior to developing intervention solutions for rural and AI PwAC. This study demonstrates a clear need for the development of supportive programs that address the root causes of inequities in rural cancer care while focusing on individual PwAC and FCG needs. While the American Society of Clinical Oncology (ASCO) continues to advocate for all patients having access to high-quality cancer care that is affordable regardless of where one lives, 42 it is imperative to create supportive programs that are based on the local context to narrow the widening gap between rural and urban cancer care disparities. 4
Implications for future research
Objectively and efficiently measuring cancer symptom burden and caregiver burden will inform intervention adaptation to meet the needs of this distinct population. The CMSAS takes PwAC approximately 2–4 min to take and offers insight into their quality of life, 20 overall survival, and other prognostic factors 43 which is essential to evaluating palliative care interventions aimed to support PwAC and their FCGs. Additionally, CMSAS has been used with diverse populations. 44 MBCBS offers insight into the type of burden experienced by the FCGs; hence, using it to adapt and test an intervention will portray if the intervention is most applicable to overall burden or a type of burden. 26
To develop an intervention that is applicable to the state’s population, a few key considerations related to this study’s sample must be considered for future work. The first consideration related to the sample is that all the FCGs were spouses of the PwAC. This study did not capture the burden experienced by FCGs who are not married to the PwAC or have other relationships (e.g., children, family friend, or other information FCG). Since our study’s spousal FCG rate (100%) vastly differs from the national rate for spousal FCGs (12% 45 ), future work must evaluate the caregiving burdens and needs of those not caring for a spouse.
Half of the sample reported a salary between $50,000 and $99,999, with another third reporting an annual income above $99,999, equating to most participants being in the middle to upper class as defined by the 2022 U.S. Census Bureau data. 46 The service area of the rural healthcare facility has poverty rates that range from 2.8% to 34.7% 47 ; therefore, future work will need to ensure that the intervention developed is appropriate to those in the lower socioeconomic class also.
While the sample proportion of participants who identify as AI is aligned with the state demographic of 9%, 6 the goal is to ensure that the palliative care intervention developed is culturally responsive to the AI population in SD. Subsequent work should employ community-engaged approaches for intervention development and recruitment to ensure greater AI representation. This can be achieved through establishing greater partnerships with tribal clinics and health departments, working with AI community liaisons, and co-creating culturally responsive participant outreach and consent options.
Finally, PwAC survivor symptom burden and FCG burden of cancer survivors need further exploration in rural/frontier SD in AI and non-AI persons. Any intervention that arises from this work will likely be delivered to persons receiving active cancer treatments and those who are cancer survivors. A clear understanding of the differences in barriers and challenges for persons undergoing active cancer treatment versus cancer survivors will better inform the intervention.
Limitations
Our study is not without limitations. The results of this study are not generalizable as the sample resides in a single, rural state. Although we sought to be able to differentiate between the perspectives of rural dwellers and AI PwAC, the experiences of AI persons were echoed by the non-AI participants in the sample. Furthermore, we are unable to provide further distinction between AI and non-AI PwAC because of the skewed study enrollment in favor of white rural persons. Many PwACs and their FCGs opted to complete the interview as a dyad. Responses may have been biased because of the caregiving dynamic and a potential fear of hurting their loved ones unintentionally. All dyadic interviews contained potentially difficult information for the other person to hear, but all PwAC and FCGs appeared to share their perspectives openly. Recruitment may have been impacted by our method of recruitment, relying on the cancer center to distribute study information. Future work should prioritize onsite researcher presence to better establish relationships with potential PwAC to enroll in research, and to better diversify caregiver recruitment, including non-spousal caregivers. Lastly, our sample for quantitative data was not adequately powered to conduct correlational analyses. However, the quantitative data helps provide additional descriptive context to the results.
Conclusion
Cancer care in rural/frontier areas is challenged by multiple factors, including fragmented healthcare, lack of healthcare infrastructure, and vast travel distances to receive baseline cancer care. This causes significant impacts on PwAC and FCG’s ability to feel seen and heard, decision making, and problem solving. The results of this study provide essential local data among AI and rural persons in SD that demonstrate the need for palliative care programs to address symptom and caregiver burden to improve the quality of life for those living with advanced cancer in rural or frontier areas of SD and the Great Plains region.
Supplemental Material
sj-docx-2-pcr-10.1177_26323524261438152 – Supplemental material for A descriptive study of cancer care experiences and burden of rural South Dakotans
Supplemental material, sj-docx-2-pcr-10.1177_26323524261438152 for A descriptive study of cancer care experiences and burden of rural South Dakotans by Sarah Mollman, Teddi Dowling, Patricia Woolridge, Jamie Hillmer, James Odom, Marie Bakitas, Hossein Moradi Rekabdarkolaee and Brandon M. Varilek in Palliative Care and Social Practice
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524261438152 – Supplemental material for A descriptive study of cancer care experiences and burden of rural South Dakotans
Supplemental material, sj-pdf-1-pcr-10.1177_26323524261438152 for A descriptive study of cancer care experiences and burden of rural South Dakotans by Sarah Mollman, Teddi Dowling, Patricia Woolridge, Jamie Hillmer, James Odom, Marie Bakitas, Hossein Moradi Rekabdarkolaee and Brandon M. Varilek in Palliative Care and Social Practice
Footnotes
Acknowledgements
None.
ORCID iDs
Ethical considerations
This study was approved by the Avera Health Institutional Review Board (IRB Protocol #IRB00001096).
Consent to participate
Consent to participate in the quantitative portion of this study was obtained electronically prior to completing the surveys by participants acknowledging their willingness to proceed with the surveys. Written consent for the qualitative data collection was waived by the IRB. Participants were informed that their consent was implied by completing the interview and they could stop the interview at any time with no repercussions. No participants stopped the qualitative data collection prior to completion of the interview.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded in part by the Rita and Alex Hillman Foundation and the Arthur Vining Davis Foundations (Hillman Emergent Innovation: Serious Illness and End of Life Award), and in part by the South Dakota State University Research, Scholarship, and Creative Activity Challenge Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are not authorized to be shared publicly per IRB agreements.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.