
Abstract
Objective
@ctivehip is a home-based multidisciplinary telerehabilitation programme for older adults with hip fracture, conducted with the assistance of their family caregivers. This programme was useful in improving their functional recovery. Nevertheless, we were concerned about how the programme might have affected caregivers, whose assistance was essential for supporting older adults in using new technologies and ensuring their safety during the exercises and activities at home. The aim of the present study was to compare the burden, psychological factors and physical fitness of the family caregivers of older adults who opted the @ctivehip telerehabilitation programme versus those family caregivers of older adults who received the face-to-face rehabilitation provided by the Andalusian Public Healthcare System (in Spain).
Methods
In this single-blinded, non-randomized clinical trial, participants were older adults with hip fracture and their family caregivers. The telerehabilitation group (n = 30) underwent a 12-week multidisciplinary telerehabilitation programme, and the comparative group (n = 32) received face-to-face rehabilitation. Caregivers outcomes measured were (i) the burden using the Zarit Burden Interview, (ii) the anxiety and depression with the Hospital Anxiety and Depression Scale (HADS), and (iii) the Physical Fitness with the International Fitness Scale (IFIS).
Results
There were not statistically significant differences on caregiver burden between family caregivers in the @ctivehip and the comparative group, although there was a trend towards lower values [[Mean (95%CI); 14.73 (9.09 to 20.37) vs 16.03 (10.63 to 21.43); p = 0.771] as well as for anxiety and depression [5.66 (3.21 to 8.78) vs 11.19 (8.52 to 13.86); p = 0.022]. Likewise achieved better, though not statistically significant, scores in physical fitness [19.37 (17.94 to 20.81) vs 17.15 (15.77 to 18.53); p = 0.055].
Conclusion
Caregiver burden is not associated with telerehabilitation. In addition, telerehabilitation is associated with lower anxiety and depression levels among family caregivers who opt for this programme. Physical fitness is not related with telerehabilitation.
Introduction
Hip fracture is one of the most important problems related to public health today. The incidence of hip fracture increases exponentially with age, 1 reaching 830,000 cases per year in Europe. 2 In this sense, the ageing of the population observed in recent decades will lead to an increase in the incidence of hip fracture globally 3 along with higher mortality rates.4,5 In addition, hip fracture implies significant physical, social and economic consequences for older adults and their family caregivers6,7 that should be considered by social and health policies.
One of the key factors to improve and accelerate the recovery process is the inclusion of a rehabilitation programme in the short and medium term. 8 However, the limited resources make it difficult in many cases to continue rehabilitation after hospital discharge. 9 Telerehabilitation has emerged as an option that can facilitate the follow up by health professionals, reduce hospital visits and allow patients to rehabilitate from home. 10 In this context, we developed the @ctivehip, a telerehabilitation programme for older adults with hip fracture supported by their family caregivers at home. 11 The role of family caregivers was essential to assist older adults in using new technologies and ensure their safety during the performance of the exercises and activities at home. 12
The literature highlighted the relevance of family caregivers during the recovery process, as hip fracture patients usually need assistance in their activities of daily living. In addition, these family caregivers provide a great deal of emotional and social support.13,14 For those reasons, hip fracture has a direct impact on the health of family caregivers, 15 who usually experience an increased caregiver burden, 16 mental health problems such as anxiety and depression, 17 and physical problems. 18 Family caregivers have demanded more information about the older adults’ transition to home 19 and to be more involved in the decision-making process during the hospital stay of their relatives. 19 They have also suggested the use of technology to improve communication and dissemination of knowledge. 20 Based on these statements and the demands of family caregivers of a previous study that we conducted in Spain, 16 we created the @ctivehip telerehabilitation programme in which family caregivers had a very active role. Nevertheless, one of our main concerns was how the programme, which has been useful in improving the functional recovery and quality of life of older adults,21,22 could have affected their caregivers. Scientific evidence shows that caregivers do not pose a burden when carrying out this telerehabilitation in stroke patients,23,24 but there is no evidence related to telerehabilitation in hip fracture patients. Thus, the aim of the present study was to compare the caregiver burden, psychological factors, and physical fitness of family caregivers of older adults who used the @ctivehip telerehabilitation programme with the same variables in those family caregivers of older adults who received face-to-face rehabilitation at home provided by the Andalusian Public Healthcare System (in Spain).
Methods
Study design and population
This single-blinded, non-randomised clinical trial was carried out at the acute care unit of the “Virgen de las Nieves” University Hospital (Granada, Spain), and it was approved by the Ethics Committee of the Granada Research Center (CEI-GRANADA). The protocol was registered at ClinicalTrials.gov (Identifier: NCT02968589). The trial was developed according to the established guidelines by the Helsinki Declaration and Law 14/2007 on Biomedical Research. The methodology of this study has been previously described referring to the patients and is summarized below referring to the caregivers. 21 This clinical trial was written and conducted according to the ROBINS-I tool for assessing the risk of bias in non-randomised studies of interventions. 25
Participants in the present study were the family caregivers of older adults with hip fracture who participated in the aforementioned clinical trial. All older adults and their family caregivers were invited to enroll in the study if the older adults met the following inclusion criteria: (1) had undergone hip fracture surgery; (2) were 65 years or older; (3) had a high (self-reported) pre-fracture functional level (Functional Independence Measure (FIM) index > 90 points) the week before fracture; (4) were allowed weight-bearing at 48 h after surgery; (5) were discharged to their own (or their relative's) home after hospitalization, not to an institution; (6) had a family caregiver; (7) had internet access and/or a family caregiver with internet access; and (8) agreed to participate in the study by signing the informed consent form. Patients were excluded if they (1) had severe cognitive impairment (Score below 24 points on the Mini-mental State Examination) 26 ; (2) had a terminal illness with which they were not expected to live beyond 6 months; or (3) had any post-surgery complications that made it impossible to begin rehabilitation during the first week after surgery. Family caregivers of excluded patients were not invited to participate in the study.
Recruitment, allocation and blinding
The recruitment took place at the “Virgen de las Nieves” University Hospital of Granada, between January 2017 and July 2018. Eligible older adults and their family caregivers were invited to join the study by an occupational therapist (OT) or a physiotherapist (PT) associated with the study. Older adults with a hip fracture and their family caregivers could choose the allocation between (1: telerehabilitation group) usual care during hospital stay (2–5 rehabilitation sessions), an educational workshop, and the @ctivehip telerehabilitation programme (maximum of 60 sessions); or (2: comparative group) usual care during hospital stay (2–5 rehabilitation sessions), an educational workshop, and the usual post-discharge rehabilitation provided by the Andalusian Public Healthcare System, consisting of face-to-face rehabilitation at home (5–15 sessions). Due to the study design, and the fact that it was the older adults and their family caregivers who chose the allocation, it was not possible to blind them to group allocation. However, the OT, the PT and the sport scientist who collected data were blinded to the group allocation. At the same time, the statistician, the PT and the OT who performed the data analysis were also blinded to the group allocation.
Intervention
Both groups: Usual care during hospital stay and caregiver's workshop
During the hospital stay after a hip fracture, patients in both groups received the usual care, including a few rehabilitation sessions (between 2–5 sessions). Besides, an informative leaflet with recommendations and home exercises was given to the older adults and their family caregivers during the hospital stay. The family caregivers of both groups were also invited to participate in an educational workshop. The educational workshops were delivered twice a week during the patient's hospital stay by an OT and a PT, and the contents focused on postoperative management and handling of older adults with hip fracture. The workshops had two sections designed using the teach-back method based on a previous study 27 : (1) background knowledge, information and recommendations for hip fracture recovery, and (2) practice of caregiver's hands-on skills, such as supporting older adults during walking, stairs, transferring and performing other activities of daily living (e.g. bathing, dressing, toileting). A detailed description of the educational workshop is provided elsewhere. 28
Telerehabilitation group (@ctivehip)
The older adults in the telerehabilitation group performed a 12-week multidisciplinary telerehabilitation programme called @ctivehip with the support of their family caregivers at home. In the telerehabilitation programme, the older adults could complete up to five sessions of 30 to 60 min per week: three physical exercise sessions (including lower and upper body strengthening exercises, balance exercises, and cardiovascular exercises) and two occupational therapy sessions (showing a description of self-care activities and walking aids, the safest way to perform activities of daily living, and options for creating a safer home environment to prevent new falls). Each session included pre-recorded instructional videos with activities and exercises appropriate to the patient's functional status. A detailed description of the programme was provided in the protocol. 11 The role of the family caregivers was to support and supervise the older adults during the home-based sessions and to maintain communication with the health care providers through videoconferences and text messages. Thus, family caregivers played a key role during the use of the telerehabilitation programme.
Comparative group (usual care)
In addition to the usual care during the hospital stay, the educational workshops and the informative leaflet, older adults in the comparative group were offered the usual rehabilitation programme provided by the Andalusian Public Healthcare System at hospital discharge, which consists of 5–15 sessions of face-to-face rehabilitation at home (physiotherapy/occupational therapy).
Procedures
The older adults and their family caregivers enrolled in the study were assessed two times: (1) before hospital discharge (during the first week after surgery); and (2) three months after hospital discharge (at the end of the telerehabilitation programme). Participants were able to report any adverse or serious event by phone, videoconference or self-report on the online platform which was reviewed weekly by one OT.
At the beginning of the study, some sociodemographic data such as age, gender, weight, height, relationship with the patient, employment, support from other caregivers and the number of caregivers were collected during the interviews with older adults and their family caregivers. The main outcomes are described below.
Outcomes
Caregivers burden. The caregiver burden was measured by the Zarit Burden Interview. 29 The Zarit scale includes 22 questions regarding aspects of the caregiver's burden, such as mood, physical state, economic situation, and social state, as well as the caregiver's feelings in providing care to the patient. The maximum score is 110, a score below 46 is usually considered indicative of “no burden”, and a score above 56 is indicative of “severe burden”. The internal consistency of the Zarit Burden is good, with a Cronbach's α = 0.86. 30
Anxiety and depression. The psychological factors of family caregivers were measured with the Hospital Anxiety and Depression Scale (HADS). 31 This scale measures the presence of anxiety and depression. It is divided into two subscales, one related to anxiety and the other one related to depression with 7 questions for each of them. The maximum score is 42 points, with a maximum of 21 points for each subscale. In both subscales, a score above 11 indicates the presence of depression or anxiety. The internal consistency of the HADS is good with a Cronbach α = 0.80. 31
Fitness level. The fitness level of the family caregivers was measured by the International Fitness Scale (IFIS). 32 The IFIS scale consists of five questions regarding self-perceived general physical fitness, cardiorespiratory fitness, muscular strength, agility and flexibility conditions. On each question, the highest score (5 points) corresponds to the best perception of fitness and the lowest (1 point) to the poorest perception of fitness. The total score ranges from 5 to 25 points. The test-retest reliability of the IFIS, as measured by the average weighted K, is 0.45. 32
Functional status. The Functional status of the older adults with hip fracture was assessed using a self-reported scale (Functional Independence Measure (FIM) 33 ) and a performed test (Short Physical Performance Battery (SPPB) 34 ). The FIM is a clinician-rated outcome that assesses the level of assistance a person requires for daily activities. The total score ranges from 18 (totally dependent) to 126 (totally independent). The score demonstrated excellent internal consistency, with a Cronbach`s α of 0.95. 35 The SPPB has been widely used to measure the physical performance of older adults with hip fracture.34,36 It consists of three subscales: balance, walking and chair standing. Higher scores indicate better mobility (range 0–12 points). The internal consistency is high, with Cronbach's α = 0.87. 37
Sample size
The present study shows the secondary results of the clinical trial. The sample size was calculated using the functional status of older adults with hip fracture, which is the main outcome of the clinical trial, as described in the protocol. 11 Finally, a total of 70 participants, (35 in the telerehabilitation group and 35 in the usual care group) were included to obtain an 80% statistical power and an α error of 5% using a two-sample t-test. The software Epidat: software for epidemiological data analysis. Version 4.2, July 2016. Consellería de Sanidade, Xunta de Galicia, España; Organización Panamericana de la salud (OPS-OMS); Universidad CES, Colombia was used.
Data analyses
Before performing the analysis, continuous variables were checked for normal distribution by visual inspection of histograms together with the Kolmogorov-Smirnov test. An independent t-test was used to determine baseline differences between the telerehabilitation and the usual care groups for continuous variables. Sex was the only categorial binomial variable, so an X2 test was used to determine the difference.
Differences between both groups were tested with the per-protocol approach, which included those participants who met the following criteria: (1) to have valid data in both the pre- and the post-intervention assessments and (2) to have completed at least 10 sessions of the telerehabilitation programme, a criterion that only applied to the telerehabilitation group. Two models of analysis of covariance (ANCOVA) were used to determine relationships of the telerehabilitation programme. To carry out Model 1, the post-rehabilitation outcomes were used as dependent variables, the group (i.e. telerehabilitation vs. usual care) as a fixed factor and the baseline outcomes as a covariate. To test for the influence of potential confounders a sensitive analysis in Model 2 was performed. The variables that demonstrated an additional predictive capacity in Model 1 (number of rehabilitation sessions, caregiver's depression status, patient's age and patient's FIM and SPPB scores) were included as covariables in Model 2, along with the baseline outcomes. Sample data are presented as mean values and Standard Deviations or percentages. For the intention-to-treat approach, all participants (N = 69) were included and those without valid data were imputed through multiple imputations. The intention-to-treat analyses are presented as Supplementary Material. All analyses were performed using the SPSS software (version 25.0, IBM Corporation, Armonk, NY, USA), and the level of significance was set at p < 0.05.
Results
For the clinical trial, a total of 401 older adults with hip fracture and their family caregivers were identified to be eligible for the study, of which 69 older adults and their family caregivers were finally enrolled in the present study and assigned to either the telerehabilitation group (n = 35) or the usual care group (n = 34). A total of 62 family caregivers (30 in the telerehabilitation group and 32 in the usual care group) were included in the per-protocol analysis, while all 69 family caregivers were included in the intention-to-treat analysis. The intention-to-treat analysis is presented in Appendix A and B. The CONSORT 2010 flow chart (Figure 1) shows the reasons for exclusion and dropouts during the study. There were no adverse events or deaths in either group during the study.

Figure CONSORT 2010 flow chart.
Table 1 shows the baseline characteristics of family caregivers and older adults divided into the telerehabilitation and the usual care groups. There were no statistically significant differences between groups in most baseline outcomes, except for the age of both, the caregivers and the patients, with a difference of 8 years in the case of the caregivers (p = 0.010) and 4 years in the patients (p = 0.005), being the telerehabilitation group the youngest in both cases.
Baseline characteristics of family caregivers and older adults divided by the telerehabilitation and usual care groups.

*significant differences (p < 0.005).
Basal: after hip fracture surgery and before rehabilitation; BMI: body mass index; FIM: functional independence measure; HADS: hospital anxiety and depression scale; IFIS: international fitness scale; n: sample size; SD: standard deviation; SPPB: short physical performance battery. Values are presented as mean ± SD or percentages.
P-value was obtained by the independent samples T-test for continuous variables, and by the chi-square test for categorical variables.
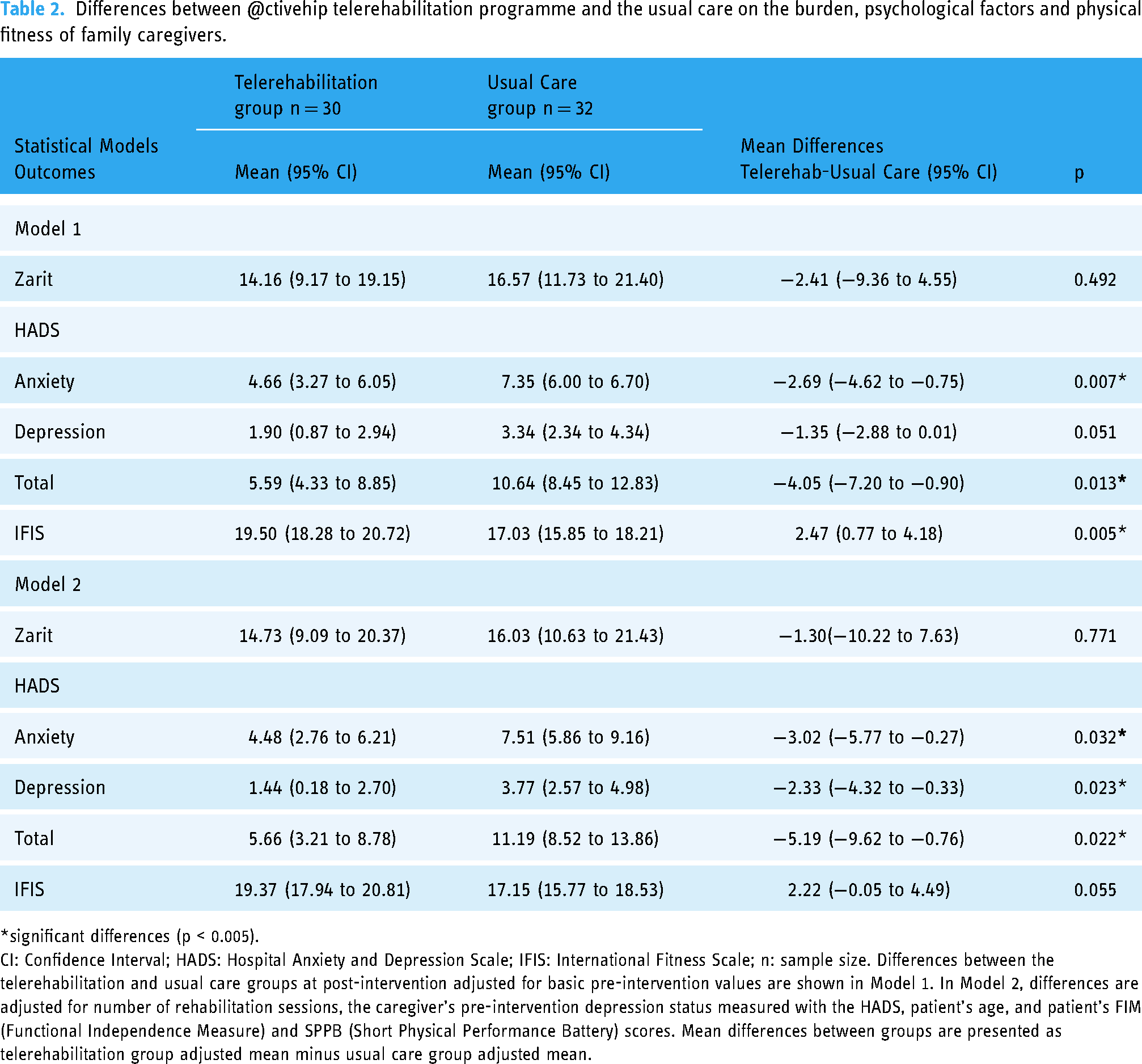
The per-protocol analysis is presented in Table 2, which shows the differences between the telerehabilitation and the usual care group 3 months after the hip fracture adjusted for the baseline values (Model 1) and additionally adjusted for the number of rehabilitation sessions, the pre-intervention depression status measured with the HADS, patient’s age, and the patient's FIM and SPPB scores (Model 2). The caregiver burden was not higher in family caregivers who supported older adults using the telerehabilitation programme; in fact, the score was lower than in the usual care group, although the differences were not statistically significant in model 1 and model 2. Concerning family caregivers’ anxiety and depression, scores were lower in the telerehabilitation group in both, model 1 (p = 0.013) and model 2 (p = 0.022). The physical fitness level of family caregivers showed higher scores in the telerehabilitation group compared to the usual care group (p = 0.005), although these differences were not statistically significant in model 2 (p = 0.055).
Differences between @ctivehip telerehabilitation programme and the usual care on the burden, psychological factors and physical fitness of family caregivers.
*significant differences (p < 0.005).
CI: Confidence Interval; HADS: Hospital Anxiety and Depression Scale; IFIS: International Fitness Scale; n: sample size. Differences between the telerehabilitation and usual care groups at post-intervention adjusted for basic pre-intervention values are shown in Model 1. In Model 2, differences are adjusted for number of rehabilitation sessions, the caregiver's pre-intervention depression status measured with the HADS, patient's age, and patient's FIM (Functional Independence Measure) and SPPB (Short Physical Performance Battery) scores. Mean differences between groups are presented as telerehabilitation group adjusted mean minus usual care group adjusted mean.
Discussion
The present study assesses whether the use of the @ctivehip telerehabilitation programme, focused on the recovery of older adults with hip fracture and delivered with the support of a family caregiver, has a relationship with increased caregiver burden and worsens the caregiver's psychological status and physical fitness compared to the face-to-face rehabilitation at home (usual care). The results indicate no association between the use of the @ctivehip telerehabilitation programme and increased caregiver burden compared with the usual care. In addition, telerehabilitation is associated with the reduction of anxiety and depression among family caregivers who choose the telerehabilitation programme. However, there is no relationship between telerehabilitation and physical fitness of family caregivers.
The profile of family caregivers who participated in our study is similar to those who participated in previous studies18,38–43. They were mainly middle-aged adult daughters18,38–43 of older adults with hip fracture. However, the age of family caregivers was slightly lower in our study, specifically in the telerehabilitation group. In Spain, only 56% of older adults access the Internet on a daily basis, a figure that increases in middle age to 90%.44,45 The usage of Internet and Communication Technology declines with age, which may explain the age difference between the groups, that were selected by choice in our study.
The caregiver burden in our study was low at the baseline in both groups compared to previous studies.16,46 The main reason for the differences could be based on the profile of the older adults included in our study, which had a high pre-fracture functional level and no cognitive impairment, which implies little previous need for care. Likewise, these two factors allow better functional recovery and social integration of older adults with hip fracture 47 and a lower caregiver burden.16,48 On the other hand, the caregiver burden levels were reduced in both groups in our study after the end of the intervention. These results could be due to the following reasons: 1) the very good functional recovery of older adults who participated in the clinical trial that was reported elsewhere (FIM score at 3 months = 120.54 points for those who used the telerehabilitation programme and 108.29 points for those who received face-to-face rehabilitation at home), 21 and 2) the workshops on postoperative patient management and home recommendations given to both groups during the hospital stay. 21 These workshops and the resolution of questions before hospital discharge contributed to increasing the caregivers’ knowledge and skills, which could be related to improved caregiver self-efficacy. Lin et al. highlighted that lower self-efficacy was correlated with a higher burden. 49 However, improving self-efficacy requires more than the provision of knowledge. In this sense, the teach-back method used in a previous study 27 was also included during the delivery of the workshops in the hospital, and during the follow up of the health providers through videoconferences and text messages while they used the telerehabilitation programme.
The levels of anxiety and depression were also lower in our study than in others39,42,50 and lower in the telerehabilitation group compared with the control group. Differences between our study and others could be based on variations in the social and health systems. In Spain, the public national health system takes care of all medical expenses (e.g. surgery costs, medical appointments, rehabilitation and commute to and from appointments), which can reduce caregivers’ concerns, including concern for economic problems, contrarily to the study by Siddiqui et al., where they observed that the economic aspect is a cause of stress for caregivers. 50 The high pre-fracture functional level and no cognitive impairment of the older adults and the support of other family caregivers could also explain the lower levels of anxiety and depression in our study. The differences between groups could be based on the active role of family caregivers who supported older adults using the @ctivehip telerehabilitation programme. Being part of the recovery process and having close communication with health professionals14,17 could have helped family caregivers to improve their psychological factors.
The telerehabilitation programme did not have an impact on the perceived physical fitness of family caregivers, despite their active participation. They were alert and physically active when supervising and supporting the older adults in the performance of the exercises and activities at home. They even exemplified the exercises sometimes. Family caregivers were a key factor to ensure the security and right execution of the programme with the support of the health care providers at the distance. The absence of association between physical fitness and rehabilitation may be due to the lack of specific contents and training for family caregivers supporting older adults in the telerehabilitation programme. Our results are difficult to compare because, to our knowledge, this is the first study considering the perceived fitness of family caregivers. Nevertheless, a previous study 18 reported the presence of caregivers’ physical problems and their influence on caregiving during the first six months after the hip fracture. Thus, physical fitness should be studied in the future as a possible factor influencing the general health status and the caregiver burden, in addition to the mental health status which has been further studied in the literature. 41
The inclusion of family caregivers during the decision-making process about the transition to home,20,51 as well as the active role that they took during the recovery process, 14 are demands stated by caregivers around the world, and we included them in our study. This could explain why there is not association between family caregivers who used the @ctivehip telerehabilitation programme and an increase of their caregiver burden, compared with those who received face-to-face rehabilitation at home, although caregivers who used the @ctivehip telerehabilitation programme had to spend more time supporting their relatives. Our results have clinical implications and support the literature's recommendations to: (i) including family caregivers during the decision-making process, 51 the transition care, 20 and the functional recovery process 17 ; (ii) improving communication and information sharing with older adults with hip fracture and their family caregivers 19 ; and (iii) increasing family caregivers’ knowledge and skills for them to feel more confident during the provision of care. 16
This study is not free of limitations. A choice-based non-randomized controlled trial was conducted, which could influence the results. Family caregivers who used the telerehabilitation programme could be more motivated than those who chose face-to-face rehabilitation at home, so the use of the telerehabilitation programme cannot be generalizable to all family caregivers. However, there were no differences between groups in terms of the caregiver burden, psychological factors and perceived physical fitness. The reasons why family caregivers did not choose the @ctivehip programme were previously reported 17 : the perception that older adults would not complete the exercise at home, the barriers that could be posed by the use of technology or caregivers’ lack of time to support their relative with technology. 17 Concerning the lack of time, it is surprising that this was one of the reasons for not carrying out the programme when there was a greater number of family caregivers employed in the telerehabilitation group, as described above, who finally were not more burdened by the @ctivehip telerehabilitation programme. The second limitation is the profile of the older adults and caregivers who participated in our study. We included family caregivers of older adults with a high pre-fracture functional level and no cognitive impairment because the programme would be supervised by the family caregivers at home. We considered that it could be more feasible to test an online intervention with this profile of older adults. Thus, our results cannot be extended to all older adults with hip fracture and their family caregivers. The third limitation is the moderate interrater reliability of the scale used to assess family caregivers’ physical fitness. 52 However, to our knowledge, this is the first study to examine the relationship between a telerehabilitation programme for older adults with hip fracture with increased burden, psychological factors and fitness status of family caregivers who support them. Our results endorse the appropriateness of using the telerehabilitation programme without causing excessive burden on family caregivers.
Conclusion
Our study showed that there is no association between the use of the @ctivehip telerehabilitation programme and increased caregiver burden, and it is associated with reduced anxiety and depression levels among participating family caregivers compared with the family caregivers of older adults with hip fracture who received the face-to-face rehabilitation provided by the Andalusian Public Healthcare System. Physical fitness of family caregivers is not associated with telerehabilitation. Considering the need of designing new strategies and tools for the recovery process of older adults with hip fracture that include their family caregivers, telerehabilitation could be a new option that needs to be studied more in deep in future research conducting randomized clinical trials when it is possible. Given that caregiver burden did not increase, we recommend that future telerehabilitation programmes incorporate specific contents to enhance family caregivers’ knowledge and skills while they provide support to older adults.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231213574 - Supplemental material for Is a telerehabilitation programme for older adults with hip fracture associated with burden of family caregivers who provide support?
Supplemental material, sj-docx-1-dhj-10.1177_20552076231213574 for Is a telerehabilitation programme for older adults with hip fracture associated with burden of family caregivers who provide support? by María Fernández-González, Mario Lozano-Lozano, Lydia Martín-Martín, Mariana Ortiz-Piña, Miguel Martín-Matillas and Patrocinio Ariza-Vega in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231213574 - Supplemental material for Is a telerehabilitation programme for older adults with hip fracture associated with burden of family caregivers who provide support?
Supplemental material, sj-docx-2-dhj-10.1177_20552076231213574 for Is a telerehabilitation programme for older adults with hip fracture associated with burden of family caregivers who provide support? by María Fernández-González, Mario Lozano-Lozano, Lydia Martín-Martín, Mariana Ortiz-Piña, Miguel Martín-Matillas and Patrocinio Ariza-Vega in DIGITAL HEALTH
Footnotes
Acknowledgments
Not applicable.
Contributorship
All authors made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. PA-V conceived the study. MO-P and PA-V carried out the literature review. LM-M, MM-M, MO-P, and P-AV were involved in the protocol development and the obtainment the ethical approval. LM-M, MM-M, MO-P and P-AV carried out the patient recruitment. MF-G and ML-L were involved in the data analysis. MF-G wrote the first draft of the manuscript. All authors reviewed and edited the manuscript critically for important intellectual content and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of the Research Centre of Granada (CEI-GRANADA) approved this study. The study was conducted according to guidelines established by the Helsinki Declaration and Law 14/2007 on Biomedical Research.
Funding
The project Activating older people after a hip fracture (ActiveHip+) has been supported by EIT Health (210752) and the Foundation for Progress and Health, Ministry of Andalusia, Spain (PI-0372-2014).
Informed consent
All participants signed a consent form.
Guarantor
PA-V
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.