
Abstract
Background:
With projections indicating an increase in childhood cancer diagnoses by 2050, family members in Kenya frequently assume extensive caregiving responsibilities. These duties are demanding and may adversely impact caregivers’ quality of life. In Kenya, caregivers manage both clinical and non-clinical tasks; however, there is a paucity of evidence regarding the extent of caregiver burden and its effect on their well-being. As cancer incidence rises, this data gap impedes the development of effective interventions to support caregivers and improve cancer care outcomes across the country.
Objective:
This study aimed to assess the burden and quality of life of caregivers at a national referral hospital in Kenya.
Methods:
This study employed a cross-sectional descriptive design involving 124 conveniently sampled participants. The Caregivers’ Quality of Life Index-Cancer and Zarit Caregiver Burden Interview tools were used to collect data on the caregivers’ quality of life and burden. Descriptive analysis was performed to generate frequencies, Pearson’s chi-square was used to assess the association between variables, and multiple linear regression was used to assess the association between variables.
Results:
Of the 124 participants, 91.9% were mothers aged 20–40 with secondary education, while most of the children (57.3%) were male, half were aged 1–5 years, and 47.6% had blood cancers. The average quality of life and burden scores were 83.38 (SD: 21.04) and 41.43 (SD: 17.52). Employment significantly reduces caregivers’ burden (B = −10.96, p = 0.001) and quality of life (B = −13.04, p = 0.001) while combined treatment significantly increases caregivers’ burden (B = 8.06, p = 0.049).
Conclusion:
The burden of care on caregivers of children with cancer is significant and has a negative impact on their quality of life. To help reduce this burden and enhance caregivers well-being, we recommended interventions such as flexible work arrangements, paid family leave, psychoeducation, and accessible respite care.
Introduction
By 2050, an estimated 13.7 million children worldwide will be diagnosed with cancer, 1 with approximately half of cases projected to occur in Africa. 2 Leukaemia, Wilms tumours, and lymphoma are the most common types of childhood cancer.3–5 In Kenya, approximately 3000 children currently have cancer. 5
Historically, caregiving is a family responsibility rooted in cultural norms of collective responsibility. Parents, as primary caregivers for their sick children, leverage their existing bond and trust.6,7 Caregivers manage activities of daily living, advocate for their loved ones, attend medical appointments, and balance family and work roles.8,9 However, as cancer management improves and convalescence extends, caregiving grows more complex, especially as a child’s illness progresses. 10 This exacerbates the care burden, often reducing the caregiver’s quality of life.11,12
In low- and middle-income countries including Kenya, caregiving is an especially complex and difficult responsibility.13–16 In Ghana, caregivers had average scores of quality of life 17 with caregivers often reporting effects on their physical health, role adjustment, which added more burden, thus affecting their health. 18 In Ethiopia, the burden of caregiving was moderate19,20 and about three-quarters of caregivers experienced poor social support. 21 In Kenya, the degree of caregiver burden was assessed to be moderate to severe, mainly attributed to low economic status. 22
In Kenya, caregivers often start with a lower quality of life due to existing poverty and limited access to health and education, making the demands of caregiving disproportionately more damaging to their physical and mental well-being. 23 Additionally, Kenyan caregivers not only assist with daily living activities but also perform both clinical and non-clinical care duties, sometimes carrying out responsibilities typically reserved for trained healthcare professionals—such as providing comprehensive nursing care often without formal training.23,24 These responsibilities have been shown to result in psychological and economic challenges, including job loss, emotional distress, and increased anxiety, all of which add to the caregiver’s burden and negatively affect their quality of life.13–16
Despite clear evidence that caregiving can have major impacts, only a single study—conducted over 5 years ago—has examined caregiver burden and quality of life in Kenya, 22 even as the cancer rates and investment in cancer care continue to increase in the country. Therefore, this study aims to address this gap by contributing to the understanding of the burden faced by caregivers and their quality of life in Kenya, ultimately informing interventions that could enhance the well-being of caregivers and improve cancer care outcomes in Kenya.
Materials and methods
Study design and setting
This baseline study used a cross-sectional approach to understand the burden and quality of life of caregivers of children with cancer receiving treatment at a national referral hospital in Kenya between October 2023 and January 2024. The study was conducted at Kenyatta National Hospital; a level six referral and teaching hospital located in Nairobi City in Kenya. Kenyatta National Hospital was purposefully selected due to its status as one of only two referral public healthcare facilities in Kenya specialising in the treatment of children with cancer and managing a significant volume of referrals from across the country, making it a critical location for paediatric oncology research. The study participants represent a wide array of sociodemographic backgrounds, reflecting the diverse communities served by the hospital, which enriches the findings and ensures that the study’s conclusions apply to a broader population of children battling cancer in Kenya.
Sampling and participant selection
The study targeted primary caregivers of children diagnosed with solid or haematological cancers as part of a baseline study for an interventional trial assessing the effect of a psychoeducation programme on caregivers’ burden and quality of life. The study sample was calculated using the standard formula for comparing two proportions. Based on an expected 20 percentage points reduction (from 74% at baseline 22 to 54% at endline) in the burden of caregiving, a study power of 90%, a significance level of 5%, and a sample size of approximately 116 was calculated and adjusted for a 10% loss to follow-up to obtain a final sample of 127.
The study included adult primary caregivers, the person taking care of the child directly offering emotional and physical care—of children below 18 years diagnosed with cancer. Any caregiver with a history of mental illness or cancer diagnosis was excluded due to challenges in differentiating the burden on quality of life caused by the disease and caregiving. The researcher obtained a list of admitted patients at the paediatric oncology wards at Kenyatta National Hospital and, using convenience sampling, recruited participants.
Data collection procedures and tools
Interviewer-administered questionnaires—Zarit’s Caregiver Burden Interview 25 and Caregiver Quality of Life Index-Cancer 26 —were used to collect demographic data and caregivers’ burden and quality of life. The 22-item Likert scale Zarit’s caregiver burden measured caregivers’ health, psychological well-being, financial status, social connections, and relationship with the patient. The tool has been previously used in a similar setting exhibiting its reliability, hence suitable to be used in this study.22,27,28
The 35-item Caregiver Quality of Life Index-Cancer measured the quality of life of caregivers using a five-point Likert scale (0 = not at all, 1 = a little bit, 2 = somewhat, 3 = quite a bite, and 4 = very much) with a total score of 0–140. 26 The scale assesses caretakers’ daily routines, sleep patterns, financial situations, spirituality, psychological elements, caregiver-patient interaction, social aspects, caring aspects, and family relationships with an emphasis on finance, disruption, positive adaptation, and burden. The tool has been used in Africa, making it reliable and suitable for this study and it has been created focusing mainly on caregivers of patients with cancer.20,29
The study instruments were assessed for content and construct validity by three experts in oncology with experience working with caregivers in Kenya. Then, the tools were pretested among caregivers of children with chronic illnesses like autism, cerebral palsy, and congenital anomalies. With limited number of paediatric patients receiving care for cancer, the suitability of the tools was assessed among caregivers with a similar level of caring experience.
This was done to determine their appropriateness, practicability, and suitability. Face and construct validity were guaranteed to confirm that the study tools were developed according to the study objectives. Cronbach’s α coefficient indicated that the tools’ reliability for Caregiver Quality of Life-Cancer and Zarit Caregiver Burden was 0.83 and 0.88, respectively. The tools were checked for completeness and accuracy and coded before data entry.
Data collection was done by the principal investigator (first author) and a quantitatively trained research assistant in a private room at the paediatric oncology wards. First, participants were screened to ensure they met the inclusion criteria and to provide them with more information about the study—the study’s objectives, benefits, and risks—and allow them to provide written informed consent. Second, participants who met the inclusion criteria and provided their consent were interviewed for an average of 45–60 min. Out of the 182 caregivers screened, 127 participants consented to join the study, and 3 withdrew during data collection. All participants were given access to a professional counsellors based in the hospital for immediate and continued counselling when needed.
Study variables
Outcome variables included caregiver burden and quality of life. The level of burden was measured using the Zarit’s caregiver burden scale with a scale of 0–4 (0 = never, 1 = rarely, 2 = sometimes, 3 = frequently, and 4 = nearly always) and a total score of 1–88; where 0–20 is no to mild burden, 21–40 is mild to moderate, 41–60 is moderate to severe, and ⩾61 is severe burden. 30 Caregivers’ quality of life was assessed using the Caregiver Quality of Life Index-Cancer tool with a total score of 0–140. 26
Predictor variables included caregivers’ sex (male or female), age in years (20–29, 30–39, 40–49, 50–59, and 60+), marital status (married or unmarried: single, divorced, separated, and widowed), employment status (employed: formal, self-employed, business, farmers and casual labourer, and unemployed) and highest level of education (higher: college and university education and lower: secondary education and below), and child’s sex (male or female), age in years (<1, 1–5, 6–10, and 11–15), diagnosis (blood tumour: leukaemia and solid tumour: lymphoma, nephroblastoma, neuroblastoma, retinoblastoma, rhabdomyosarcoma, brain tumour, osteosarcoma, synovial sarcoma, and other cancers) and current treatment (single regimen: either chemotherapy, radiotherapy, surgery or palliative care and combined treatment regimens).
Data analysis
Collected data were entered into a Microsoft Excel sheet and cleaned before being entered into Statistical Package for Social Sciences version 20 for further analysis IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). We assessed normality for the continuous data including caregivers’ burden and quality of life, which showed normal distribution. Thus, mean, median, and standard deviation (SD) were used to describe continuous data, while frequencies and percentages were used to describe categorical data. Pearson’s chi-square and multiple linear regression were used to measure the association between the independent variables and caregivers’ burden and quality of life. The variance inflation factor was used to assess multicollinearity among the variables. Statistical significance was set at p ⩽ 0.05.
Ethical considerations
Ethical approval for the study was obtained from the Kenyatta National Hospital and the University of Nairobi Ethics and Review Board (KNH-ERC/A/492). Research permits were provided by the National Commission for Science, Technology and Innovation (NACOSTI-P-23-30490) and the Hospital’s Paediatric Department. The purpose of the study was clearly explained to the participants who provided written informed consent. Personal identifiers such as names and phone numbers were omitted to ensure participants’ anonymity and data collected was managed by the research team only to maintain confidentiality.
Results
Sociodemographic characteristics of the participants
Of the 124 participants who took part in the study, 114 (91.9%) were women, 51 (41.6%) were 20–29 years old and 104 (84.9%) were mothers. At least two-thirds of the participants were married (n = 83, 66.9%) or unemployed (n = 84, 67.7%), and 46 (37.1%) were secondary educated (Table 1). Many of the participants’ children were boys (n = 71, 57.3%), aged 1–5 years (n = 62, 50.0%), and second-born (n = 40, 32.2%). Fifty-nine (47.6%) children had blood cancers, of which 47 (37.9%) had leukaemia. Almost all children were on treatment, with those on a single regimen (n = 101, 81.5%) being mainly on chemotherapy (n = 95, 76.6%; Table 1).
Characteristics of caregivers and their children.

Yes, nursery, primary, secondary (total).
Blood cancers: leukaemia (n = 47, 37.9%) and lymphoma (9.7%), and solid tumours: nephroblastoma (n = 22, 17.7%), retinoblastoma (n = 14, 11.3%), neuroblastoma (n = 8, 6.5%), brain tumours (n = 3, 2.4%), osteosarcoma (n = 3, 2.4%), and others solid tumours (n = 9, 7.3%).
Caregiver burden
The overall mean caregiver burden was 41.43 (SD: 17.52), with the mean burden for caregiver relationship with the child, psychosocial and financial burden of 20.33 (SD: 7.87), 18.0 (SD: 10.73), and 3.0 (SD: 1.32), respectively. About half of the participants (n = 60, 48.4%) had mild to moderate burden, 31 (25%) had moderate to severe burden and 22 (17.7%) had severe burden, while 11 (8.9%) had no to mild burden (Table 2).
Caregivers’ levels of burden and means within the subscales.
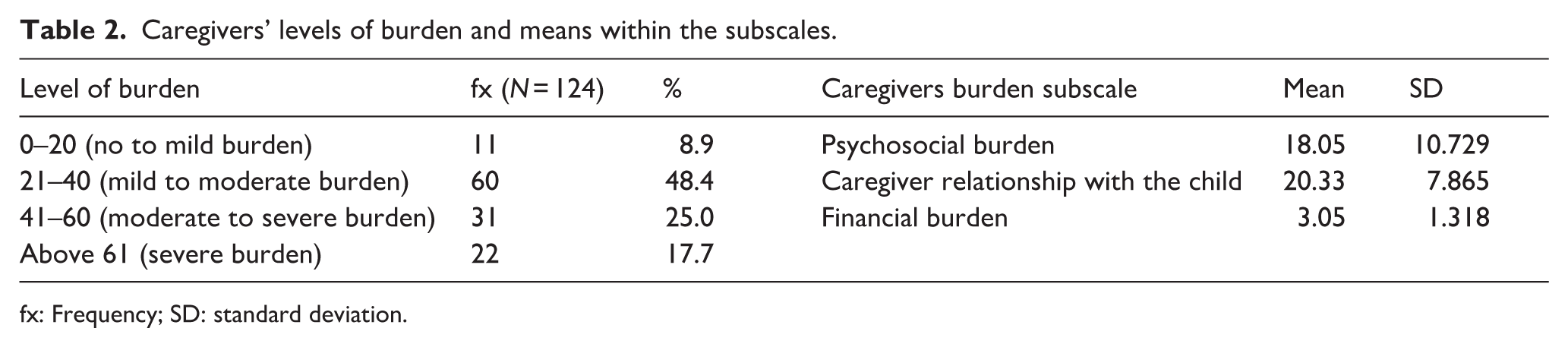
fx: Frequency; SD: standard deviation.
Caregivers of children experienced substantial burden, particularly in balancing caregiving with other responsibilities, with 89% reporting stress frequently or nearly always due to this conflict. Financial strain was a major concern, with 69% feeling they lack sufficient funds for their child’s care alongside other expenses, while 56.5% believing they should be doing more. Emotional and social burden were evident, as 45.1% felt their child expects exclusive dependence, 27.6% reported a suffering social life, and 31.7% are afraid of their child’s future. Privacy loss affected 28.2% frequently or nearly always, and 27.4% felt they had lost control of their life. Positively, participants expressed low desire to relinquish care (only 6.5% sometimes or more) and minimal embarrassment or anger (10.5% and 9.8% frequently/nearly always). However, overall, 41.9% felt burdened frequently or nearly always, with health suffering for 34.9% and dependency concerns high at 71.5% (Figure 1; Supplemental Table 1).

Responses on Zarit Caregiver Burden.
Caregiver’s quality of life
The overall mean of caregivers’ quality of life was 83.38 (SD: 21.04) with subscale means of 22.30 for burden, 17.81 for disruptiveness, 16.86 for positive adaptation, and 9.24 for financial concerns (Table 3).
Quality of life—Overall and subscale means.
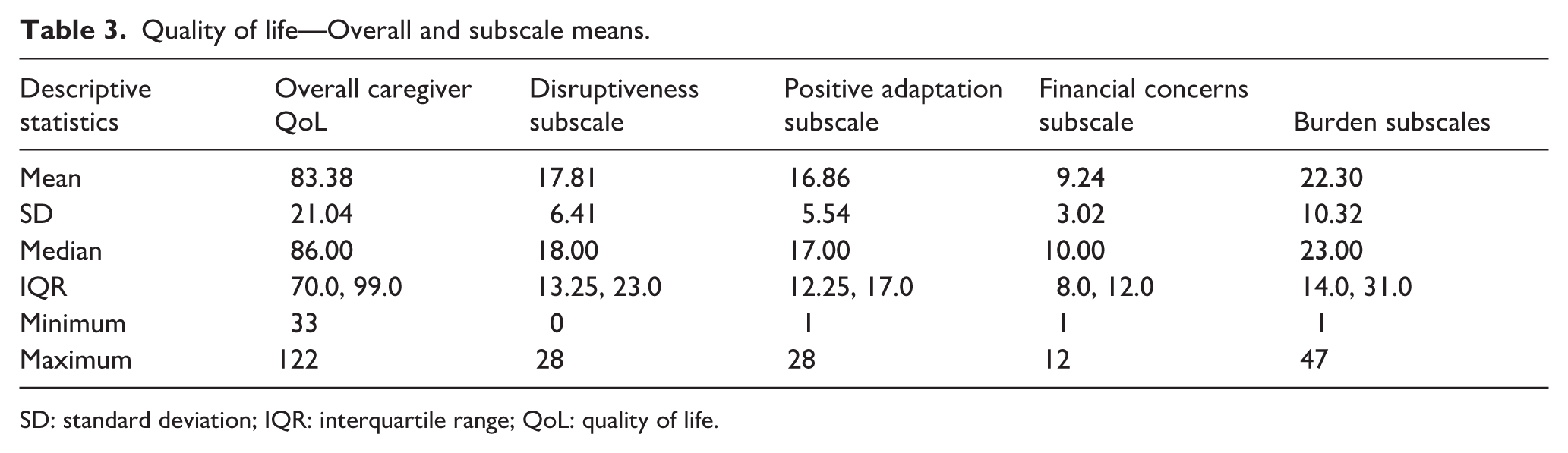
SD: standard deviation; IQR: interquartile range; QoL: quality of life.
Participants reported mixed impact on their quality of life. Most participants (94%) reported altered daily routine, with 61% noting increased stress and worries. Fifty-two percent felt increased mental strain, and 42% experienced fatigue, with 68% uncertain about their future and 61% concerned about insurance. However, 48% felt supported by friends and neighbours, with 70% feeling a positive outlook on life and 61% noting improved spiritual focus, though only 4% felt confident in getting loved ones well, and 51% showed interest in family care involvement (Figure 2; Supplemental Table 2).

Responses on Caregiver Quality of Life Index-Cancer.
Factors associated with caregiver’s burden and quality of life
Our model accounted for 19.6% (R 2 = 0.196) of the caregivers’ burden and 20.6% (R 2 = 0.206) of their quality of life. Employment significantly reduces caregivers’ burden (B = −10.96, p = 0.001) while combined treatment significantly increases caregivers’ burden (B = 8.06, p = 0.049), with having a solid tumour showing borderline significance for lower burden (B = −7.10, p = 0.052). Caregivers’ quality of life significantly reduces with employment (B = −13.04, p = 0.001; Table 4). A significant association was found between the three subscales of burden and the overall caregiver burden and quality of life (Supplemental Table 3). Similarly, with the exception of positive adaptation, there was a significant association between quality of life subscales and overall caregivers’ burden and quality of life (Supplemental Table 4).
Relationship between sociodemographic variables and caregiver quality of life and burden.

SE: standard error; CI: confidence interval.
Bold: Significance p < 0.05.
Two-sided test.
Discussion
Our study found that most primary caregivers of children with cancer were middle-aged, married mothers, caring for boys aged 1–5 diagnosed mainly with haematologic cancers. Caregivers reported a moderate quality of life and mild to moderate burden; employment significantly reduced both, while combined treatments increased burden.
In our study, caregiver burden was generally moderate, with nearly half of participants experiencing mild to moderate levels, a quarter reporting moderate to severe levels, and a smaller proportion facing severe burden. A previous study conducted at the same hospital highlighted that many caregivers experienced moderate to severe burdens, 22 but our findings indicate a considerable improvement in the situation over time. This improvement could be attributed to potential shifts in cancer care, support or individual coping mechanisms within the care environment over the period, but could also be due to different patient profiles. Also, the hospital has a better integrated cancer care with more oncology specialists and expanded caregiver support groups, resulting in potentially caregivers receiving more support and training, making them feel more prepared and in control of their role, 31 which lowers burden. In addition, a moderate caregiver burden could be related to improvements in the National Health Insurance Fund coverage, providing adequate financial cover for cancer treatment directly reducing the financial concerns subscale of burden, 32 thus lowering the overall burden. 33 However, our study showed caregivers had less burden compared to those in Ethiopia.19,20 This is majorly attributed to the differences in caregivers profiles with most caregivers in Ethiopia being fathers and employed, compared to our study, where most were mothers and unemployed.
Overall, caregivers reported a moderate level of quality of life, with average scores observed across the burden, disruptiveness, positive adaptation, and financial concerns subscales. The moderate quality of life could be attributed to financial constraints due to the increased cost of treatment, 34 social stigma in avoidance of financial help, and increased caring burden. 35 A moderate quality of life could indicate that caregivers are highly resilient and use effective coping mechanisms to manage stressors. It could also indicate that caregivers see caregiving as a moral duty, highlighting the cultural and spiritual nature of caregiving in Kenya, limiting the negative emotional toll. 36 The average financial concerns could indicate that financial strain may not be overwhelming the caregiver’s quality of life, or it is being successfully mitigated by family support or other measures such as improved health insurance in Kenya. 32 In addition, the moderate quality of life seems to be maintained by money and adaptation but strained most significantly by the loss of personal time and freedom. Interventions should focus on reducing disruptiveness through hospital-based respite care, subsidised accommodation near the hospital, and flexible work.
The mean quality of life of our participant’s was lower compared to that of a study done in Ghana, 17 and a higher compared to Singapore. 37 In our study, most participants indicated a lack of support from family members, which could negatively affect caregivers’ well-being during the caregiving period. Support from family members is essential for caregivers during the diagnosis and treatment of childhood cancer, as it provides psychological and financial support as well as care for other children at home. 16 Communities, friends, and society play a crucial role in addition to family support. Most participants reported a significant lack of support from friends and neighbours. In Ethiopia, about three-quarters of participants indicated that they experienced poor social support, with only one person reporting receiving assistance. 21 In Ghana, participants withdrew from social activities because of stigma and negative comments from others. 18 This indicates the perception that people have towards cancer. Community engagement and literacy can help reduce social stigma, foster social help, and reduce treatment abandonment.38,39
We found that employment had a dual effect—it reduced burden but also lowered quality of life. This suggests that while work may alleviate some stressors such as financial, it may strain caregivers’ overall well-being, possibly due to time constraints or emotional toll. Employment often acts as a protective factor and a psychological buffer against the overwhelming demands of caregiving. 40 The income from employment directly alleviates the significant financial strain associated with caregiving, reducing financial stress and hence reducing the perceived burden on the caregiver. 40 Second, while caregiving can become all-consuming, work provides a separate identity, offering a structured psychological break from the constant caregiving demands. 41 This external validation and sense of normalcy can counteract the feelings of isolation and loss of self often reported by non-employed caregivers. 42 The workplace offers a ready-made social network of colleagues and supervisors. Positive social interaction and support outside the caregiving environment help buffer the mental health consequences of burden. 43
Despite employment mitigating the feeling of burden by providing resources and respite, it sometimes severely strains the caregiver’s time, energy, and resources, leading to a measurable decline in quality of life. Juggling two demanding, full-time roles—as an employee and caregiver—results in severe time constraints and work-care conflict. Employed caregivers frequently sacrifice time for self-care, sleep, leisure, and personal appointments. 18 This chronic time poverty directly lowers their quality of life in the physical, psychological, and social domains.41,44 The demand of both roles sometimes exceeds the caregiver’s capacity, leading to physical and emotional exhaustion, poor health outcomes, and a reduced sense of overall well-being. Besides, employed caregivers often experience issues like absenteeism, presenteeism, arriving late, or leaving early. These issues can result in disciplinary action, missed promotions, reduced hours, or job loss, creating a continuous state of anxiety about job security and long-term financial health,45,46 affecting overall quality of life. In this regard, interventions that support flexible hours, compressed workweeks, and work-from-home options and paid family leave, supportive management training, availability of affordable, high-quality formal and informal respite care services are recommended to reduce caregivers’ burden and improve their quality of life.
The study also found that combined treatment modalities were associated with a significant increase in caregiver burden. Treatment, while curative, is often toxic, aggressive, and unpredictable and requires the caregiver to manage complex tasks and side effects, acting as a stressor, directly increasing their objective burden. 47 Chemotherapy is a major driver of caregiver burden due to the management of severe side effects 48 while surgical interventions, especially extensive ones, introduce physical demands and recovery requirements. 49 Besides, while often less physically demanding than chemotherapy, radiotherapy imposes a strict schedule that creates major logistical hurdles, especially in low-resource settings. 50 Hence, health facilities should provide psychoeducation and structured discharge training to equip caregivers with the skills to manage treatment side effects at home. Furthermore, reducing barriers such as simplifying scheduling and providing transport or accommodation assistance can directly mitigate the disruptiveness caused by treatment demands.
Study limitations
The findings should be interpreted cautiously due to several limitations. This study was conducted at a single national referral hospital in Kenya, which limits the generalisability of its findings. As a hospital-based study, we did not collect important variables such as family socioeconomic status or coping strategies. Although the study tools were pretested with caregivers of chronically ill children, which could influence their validity, the experts’ review aided reliability. The cross-sectional design limits conclusions about causality, while convenience sampling may have introduced self-selection bias. Despite these issues, using validated tools allows comparison with similar studies, though some questions may have been sensitive, potentially impacting response reliability.
Conclusion
In conclusion, our study highlights that caregivers experience moderate levels of burden and quality of life, with employment status being a key factor affecting both. To support caregivers and reduce isolation and stress, we recommend interventions such as flexible work arrangements, paid family leave, psychoeducation, and accessible respite care, and promotion of peer support and community programmes. Future research should use longitudinal approaches to identify effective strategies for improving caregivers’ quality of life.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261434998 – Supplemental material for Burden and quality of life among caregivers of children diagnosed with cancer at Kenyatta National Hospital, Kenya: A cross-sectional study
Supplemental material, sj-docx-1-pcr-10.1177_26323524261434998 for Burden and quality of life among caregivers of children diagnosed with cancer at Kenyatta National Hospital, Kenya: A cross-sectional study by Doris W. Machaki, Albanus Mutisya, Jostine Mutinda, Sherry Oluchina and Samwel Maina Gatimu in Palliative Care and Social Practice
Footnotes
Acknowledgements
We acknowledge the contributions of all the study participants (children, parents, and caregivers). We wish to express our appreciation to Dr Michael Weitzner, who gave us permission to use the Caregiver Quality of Life Index-Cancer tool.
Ethical considerations
Ethical approval for the study was obtained from the Kenyatta National Hospital and the University of Nairobi Ethics and Review Board (KNH-ERC/A/492). Research permits were provided by the National Commission for Science, Technology and Innovation (NACOSTI-P-23-30490) and the Hospital’s Paediatric Department.
Consent to participate
Written informed consent was obtained from all subjects involved in the study after clearly explaining the purpose of the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by The Aga Khan University–Kenya, School of Nursing and Midwifery Dean’s Fund. The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset generated and/or analysed during the current study is not publicly available due to participant privacy. Data can be available from the corresponding author* upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.