
Abstract
Background:
Advance care planning (ACP) has become central to end-of-life policy in Japan, aiming to uphold autonomy and dignity. However, conceptual confusion about its ethical and legal foundations risks promoting a procedural rather than ethically grounded approach to ACP.
Aims:
This study aimed to (1) assess healthcare professionals’ knowledge of ethical and legal concepts in medical decision-making, (2) examine how patient autonomy is respected through clinical vignettes, and (3) identify factors associated with respect for autonomy.
Design:
Cross-sectional questionnaire survey.
Methods:
Healthcare professionals (n = 549) in a Tokyo geriatric hospital completed measures of attitudes toward and experiences with end-of-life care, knowledge of legislation and ethical concepts underlying medical decision-making, and response to two clinical vignettes depicting decision-making dilemmas. Analyses included descriptive statistics, comparisons across occupational groups, and multivariate regression to identify factors associated with respect for patient autonomy.
Results:
Misconceptions were common: 38% of participants equated ACP exclusively with decisions to forgo active treatment, and many conflated ACP with current rather than future-oriented care planning. The vignette study further demonstrated that a dementia diagnosis alone reduced respect for patient preferences in 27.8% of cases. Ethical dilemmas frequently arose when ACP was applied in practice, especially regarding withholding or withdrawing treatment, suggesting that ACP does not necessarily resolve such dilemmas and may generate new ones in some cases. Two independent factors related to greater respect for patient autonomy were identified: greater knowledge of ethical concepts and personal experience witnessing harm from insufficient medical intervention.
Conclusion:
ACP policies in Japan have advanced more rapidly than healthcare professionals’ ethical and legal understanding, risking procedural rather than ethically grounded practice. Systematic, cross-professional education integrating legal literacy, ethical reasoning, and reflective learning is essential to ensure that ACP genuinely safeguards patients’ rights and supports ethically sound decision-making.
Plain language summary
Keywords
Introduction: Beyond ACP—Clarifying medical decision-making in Japan
Advance care planning (ACP) has been widely promoted in health policy as a means of enhancing autonomy and dignity at the end of life. In Japan, governmental initiatives have strongly endorsed this concept. A major turning point occurred in 2007 following two widely publicized cases involving the withdrawal of life-sustaining treatment.1,2 In the latter case, the Tokyo High Court urged national deliberation and the development of legal and procedural frameworks, instead of establishing legal criteria for treatment withdrawal. 3
Since then, ACP has gradually been incorporated into health policy and has now become an institutional requirement. Three months after the court decision, the Ministry of Health, Labour and Welfare issued the Guidelines for the Decision-Making Process in End-of-Life Care, 4 emphasizing due process in end-of-life treatment decisions. The 2018 revision explicitly promoted ACP, 5 and the 2024 revision of the national medical reimbursement system further required healthcare institutions to develop internal protocols for decision-making support at the end of life, effectively mandating the creation of institutional ACP guidelines.
Building on these developments, recent policy reforms have further strengthened the institutionalization of decision-making support based on national guidelines. In particular, the 2024 revision of the inpatient reimbursement system made hospitals ineligible for the basic inpatient fee unless they established institutional policies on end-of-life decision-making support, thereby effectively mandating the development of institutional ACP guidelines. Only facilities limited to pediatrics, obstetrics, or child–adolescent psychiatry are exempt from this requirement.
In Japan, ACP is recommended for individuals with chronic, progressive, or life-limiting conditions and is implemented across outpatient, inpatient, and long-term care settings. 5 National guidelines define ACP as a multidisciplinary process involving collaboration among physicians, nurses, social workers, and other relevant professionals. Physicians provide prognostic information and treatment options, nurses frequently take a leading role in facilitating ongoing conversations and documenting preferences, and social workers assist with evaluating and coordinating social and home environments. Nurses are expected to play a particularly important role in ACP practice,6,7 and many institutions rely on them to take the lead in developing ACP protocols.
Despite these policy efforts, the actual implementation of ACP remains limited. A recent study 8 reported that only 28.7% of geriatric specialists engaged in ACP during the COVID-19 pandemic, even among experienced clinicians. Furthermore, medical record reviews show that although considerable patient participation in ACP discussions, 7 the boundaries between patients’ preferences and those of family members are often blurred. Whereas these developments have placed ACP at the forefront of national policy initiatives, the ethical and legal understanding of “medical decision-making as a patient’s right” remains inconsistently interpreted and implemented across clinical settings. In Japan, cultural norms that view health conditions as a family matter, 9 traditionally prioritize family preferences over those of the patient,10,11 and favor avoiding assertive decision-making, 11 collectively obscure the identity of the actual decision-maker. This tendency often conflicts with the principle of individual autonomy underpinning informed consent (IC) and, more recently, ACP, which seeks to preserve autonomy even when patients lose decision-making capacity.
IC was introduced to Japan in the 1970s and became widespread in the late 1980s. 12 Its application has been deeply shaped by Japanese sociocultural values. A 1995 government report, for example, explicitly stated that family preferences should be considered an integral part of medical decision-making and could not be ignored. 13 As a result, although IC is now regarded as standard clinical practice, it is often understood primarily as a decision-making process involving physicians, patients, and families rather than as an expression of the patient’s individual right to self-determination. 14 This misunderstanding is particularly evident in clinical practice, where IC is frequently misinterpreted as the physician’s act of explaining the medical condition to the patient and/or family. 15
Family-centered decision-making remains deeply rooted, especially when the patient’s capacity is perceived as diminished. For instance, though the proportion of direct cancer diagnosis disclosures to patients rose from 20%–30% in the 1990s to 70%–90% in the 2010s, 16 it remains common for families to request nondisclosure, or for physicians to assume, without question, that disclosure to the patient is unnecessary when the patient has a mental health condition. 17 However, Japanese law does not grant anyone the right to provide substitute consent for medical treatment on behalf of an adult. Our previous pilot study 18 found that healthcare professionals often conflate patient autonomy with family-centered decision-making, leading to misconceptions about core ethical and legal terminology. This duality has contributed to ongoing conceptual confusion in the ethical and legal foundations of ACP. While culturally competent care requires sensitivity to family roles and social norms, 19 cultural adaptation should not be confused with conceptual misunderstanding.
Existing literature on ACP in Japan has largely focused on its practical implementation, 20 whereas a recent review has summarized culturally sensitive recommendations for ACP in the Japanese context. 11 However, the conceptual understanding of the ethical and legal foundations of medical decision-making has received little attention. This study was therefore designed to explore the ethical and legal landscape of medical decision-making in Japan. Specifically, it aimed to: (1) assess healthcare professionals’ knowledge of the ethical and legal foundations of medical decision-making; (2) evaluate how patient autonomy is respected using clinical vignettes; and (3) identify factors associated with respect for the patient’s autonomy.
Methods
Study participants and setting
This study was conducted at Tokyo Metropolitan Institute for Geriatrics and Gerontology, a 550-bed, public geriatric hospital in the central part of Tokyo, specializing in acute care for older patients, with a reported average length of stay of 12.5 days.
A cross-sectional questionnaire survey was administered between June 2 and June 16, 2025. The survey targeted healthcare professionals in five occupational categories: physicians, nurses, pharmacists, psychologists, and social workers. A total of 749 individuals were approached: 180 physicians, 506 nurses, 35 pharmacists, 13 psychologists, and 15 social workers. Those who provided written IC were included in the study. No additional exclusion criteria were applied.
Questionnaire design
The questionnaire is provided as Supplemental File 1.
Sociodemographic factors
With respect to sociodemographic characteristics, data were collected on age, sex, current occupation, and years of experience. For analysis, age was dichotomized into “20s–30s” and “40s and above.” Occupation was categorized into three groups: “Physicians,” “Nurses,” and “Others,” which included pharmacists, psychologists, and social workers. Years of experience were dichotomized into “less than 10 years” and “10 years or more.”
Attitudes toward and experience of end-of-life care
Attitudes toward end-of-life care
Attitudes toward end-of-life care were assessed using the Japanese short form of the Frommelt Attitudes Toward Care of the Dying Scale, Form B (FATCOD-Form B-J-s).21,22 The scale consists of six items, each rated on a 5-point Likert scale from 0 (Strongly Disagree) to 4 (Strongly Agree), with negatively worded items reverse-scored. Total scores range from 0 to 24, with higher scores indicating a more positive attitude toward end-of-life care.
Experience with end-of-life care
Participants answered “Yes” or “No” to seven items about prior personal or professional experiences: (1) experience being involved in a medical decision that directly affected their own life expectancy; (2) experience being involved in a medical decision that directly affected the life expectancy of a loved one; (3) experience of bereavement involving a loved one; (4) experience providing end-of-life care for a patient under their care; (5) experience providing end-of-life care for a patient with dementia; (6) experience perceiving that “excessive medical intervention” may have compromised a patient’s quality of life (QOL) or quality of death (QOD); and (7) experience perceiving that “insufficient medical intervention” may have compromised a patient’s QOL or QOD.
Knowledge of legislation and key ethical concepts underlying medical decision-making
Items to assess knowledge were initially developed by the authors and later refined with input from a lawyer and an experienced geriatric psychiatrist specializing in clinical ethics.
Knowledge of legislation
Participants’ knowledge of legislation governing medical consent was assessed using two true/false items:
(L1) When a patient lacks decision-making capacity, the law permits family members to provide consent for medical procedures on the patient’s behalf.
(L2) When a patient lacks decision-making capacity, the law permits an adult guardian to provide consent for medical procedures on the patient’s behalf.
A Legislation Knowledge Score was calculated by summing the number of correct responses (range: 0–2).
Knowledge of ethical concepts
To assess participants’ knowledge of key ethical concepts in medical decision-making, six illustrative statements describing clinical situations were presented (E1–E6; see Table 1). Each statement was paired with a term, such as ACP, Do Not Attempt Resuscitation (DNAR), advance directive, or shared decision-making (SDM), and participants were asked to judge whether the assigned term was appropriate.
Knowledge score for legislation and ethical concepts..
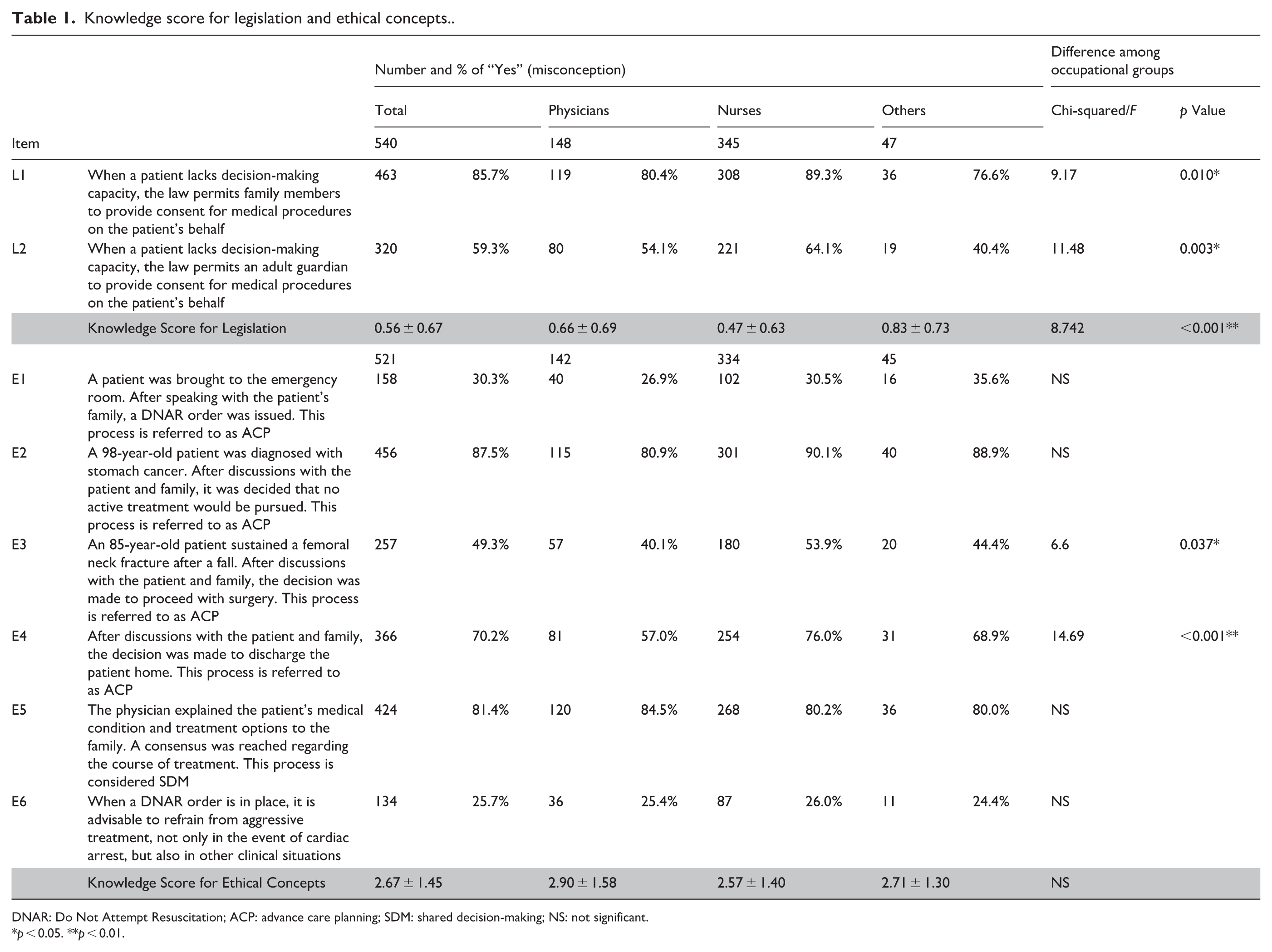
DNAR: Do Not Attempt Resuscitation; ACP: advance care planning; SDM: shared decision-making; NS: not significant.
p < 0.05. **p < 0.01.
An Ethical Concepts Knowledge Score was calculated by summing the number of correct responses (range: 0–6).
Practice of medical decision-making
Clinical Vignette A
Clinical Vignette A was initially developed by the authors and subsequently refined with input from an experienced geriatric psychiatrist specializing in dementia. To ensure realism and maintain neutrality, the vignette was reviewed by 7 physicians and 20 certified nurses who evaluated its clinical plausibility and impartiality. Formal statistical validation was not conducted.
Participants were presented with a case involving an 82-year-old woman, Ms. A, diagnosed with incurable gastric cancer with multiple liver metastases. They were asked to choose one of three treatment options: (a) chemotherapy to slow disease progression; (b) gastrectomy to prevent anemia and tumor-related bleeding; or (c) best supportive care (BSC), with no active intervention. Participants responded to four questions as the scenario progressed from A1 to A4.
Scenario A1: If you were Ms. A, which treatment option would you choose?
Scenario A2: Ms. A clearly stated that she did not want any active treatment. If you were the healthcare professional in charge of Ms. A’s care, which treatment option would you choose for her?
Scenario A3: Following Scenario A2, Ms. A’s son strongly insisted on chemotherapy. In this situation, which treatment option would you choose for her? At this time, Ms. A’s decision-making capacity was not in doubt.
Scenario A4: Following Scenario A3, Ms. A was found to have impaired recent memory and orientation to time. After psychiatric consultation, she was diagnosed with dementia. Her son strongly insisted on proceeding with chemotherapy, arguing that her wishes should not be followed given her dementia diagnosis. In this situation, which treatment option would you choose for her?
For details, see Supplemental File 1.
In each scenario (A1–A4), participants were asked to select a treatment option, and responses were compared across occupational groups.
In addition, in Scenarios A3 and A4, participants were asked to rate how strongly Ms. A’s and her son’s preferences influenced their final treatment decisions. These scores, referred to as influence ratings, were measured on a 4-point Likert scale ranging from 0 (no influence) to 3 (strong influence), with higher scores indicating a greater perceived influence for each individual assessed independently.
To analyze these data, two types of comparisons were performed: a within-scenario comparison examined whose preferences carried greater weight within each scenario, and a between-scenario comparison assessed how a dementia diagnosis affected decision-making by comparing changes in influence ratings for each individual between Scenario A3 (no dementia) and Scenario A4 (with dementia).
Clinical Vignette B
Vignette B was adapted from Wikstøl et al. 23 and revised to reflect the Japanese context. Formal statistical validation was not conducted.
The scenario described an 80-year-old man, Mr. B, living with advanced Alzheimer’s disease in a nursing home. Following a progressive decline in oral intake and persistent refusal to eat, tube feeding was started. The facility staff assessed Mr. B as lacking decision-making capacity.
The participants were presented with two scenarios:
Scenario B1: Prior to his dementia diagnosis, Mr. B had clearly expressed that he did not wish to be kept alive if he were to develop an incurable condition. This preference was documented in his medical record.
Scenario B2: Two years after his dementia diagnosis, Mr. B moved into a nursing home. At the time of admission, he explicitly expressed his wish to receive full treatment, which was documented in the institutional record.
Further details are provided in Supplemental File 1.
After reviewing each scenario, participants were asked to rate their agreement with the following statements using a 5-point Likert scale (1 = Not at all agree; 5 = Strongly agree): (Q1) If you were in Mr. B’s condition, would you consider it acceptable to have fluids and nutrition withdrawn? (Q2) Do you consider it acceptable to withdraw fluids and nutrition? (Q3) Do you consider it acceptable to withhold potential future treatment? Responses were dichotomized into “Agree” and “Do not agree,” and compared across occupational groups for each scenario.
Statistical analysis
All analyses were performed using SPSS Statistics for Windows, Version 29.0.1.0 (IBM, Armonk, NY, USA). Comparisons of continuous variables among occupational groups were tested using ANOVA with Bonferroni-adjusted pair-wise comparisons. Categorical data were analyzed via chi-squared tests.
To explore the factors associated with respect for patient autonomy, linear regression was performed. Significance was set at p < 0.05.
Reporting guidelines
This study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cross-sectional studies. The STROBE checklist is provided as Supplemental File 2.
Results
Demographic characteristics of participants
The participants’ sociodemographic characteristics are shown in Table 2. A total of 549 responses were collected, yielding an overall response rate of 73.3%. Response rates by profession were as follows: physicians (82.8%, n = 149), nurses (69.6%, n = 352), pharmacists (60.0%, n = 21), psychologists (92.3%, n = 12), and social workers (100.0%, n = 15).
The participants’ sociodemographic characteristics.
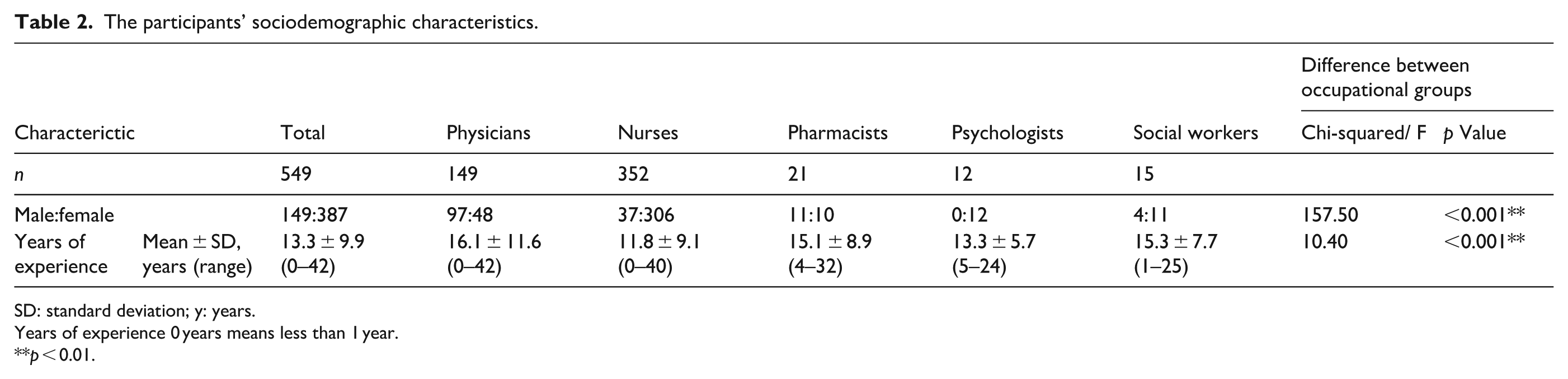
SD: standard deviation; y: years.
Years of experience 0 years means less than 1 year.
p < 0.01.
The male-to-female ratio of the participants was 149:387. The average years of experience in the current profession was 13.3 ± 9.9 years (range: less than 1–42 years). Significant differences were observed across occupational groups: nurses had significantly fewer years of experience than physicians (p < 0.001). The proportion of male participants was significantly higher among physicians (p < 0.001).
Participants’ attitudes toward and experience with end-of-life care
Attitudes toward end-of-life care
Table 3 summarizes the FATCOD-Form B-J-s scores. Physicians consistently showed higher attitudes toward end-of-life care than other groups, as indicated by FATCOD-Form B-J-s scores (p = 0.026–0.037).
FATCOD-Form B-J-s scores.

CI: confidence interval; FATCOD-Form B-J-s: Frommelt Attitudes Toward Care of the Dying Scale, Form B.
p < 0.05.
Experience with end-of-life care
The results are presented in Table 4. Of the participants, 16.9% had experience being involved in a medical decision that directly affected their own life expectancy (1), and 32.1% had been involved in a decision affecting the life expectancy of a loved one (2). In addition, 74.7% had experienced the bereavement of a loved one (3), 82.5% had provided end-of-life care for a patient (4), and 71.2% had provided such care for a patient with dementia (5). Of the participants, 81.6% reported having felt that “excessive medical intervention” may have compromised a patient’s QOL or QOD (6), and 46.5% reported experiences in which “insufficient medical intervention” may have had a similar impact (7).
Experience with end-of-life care.
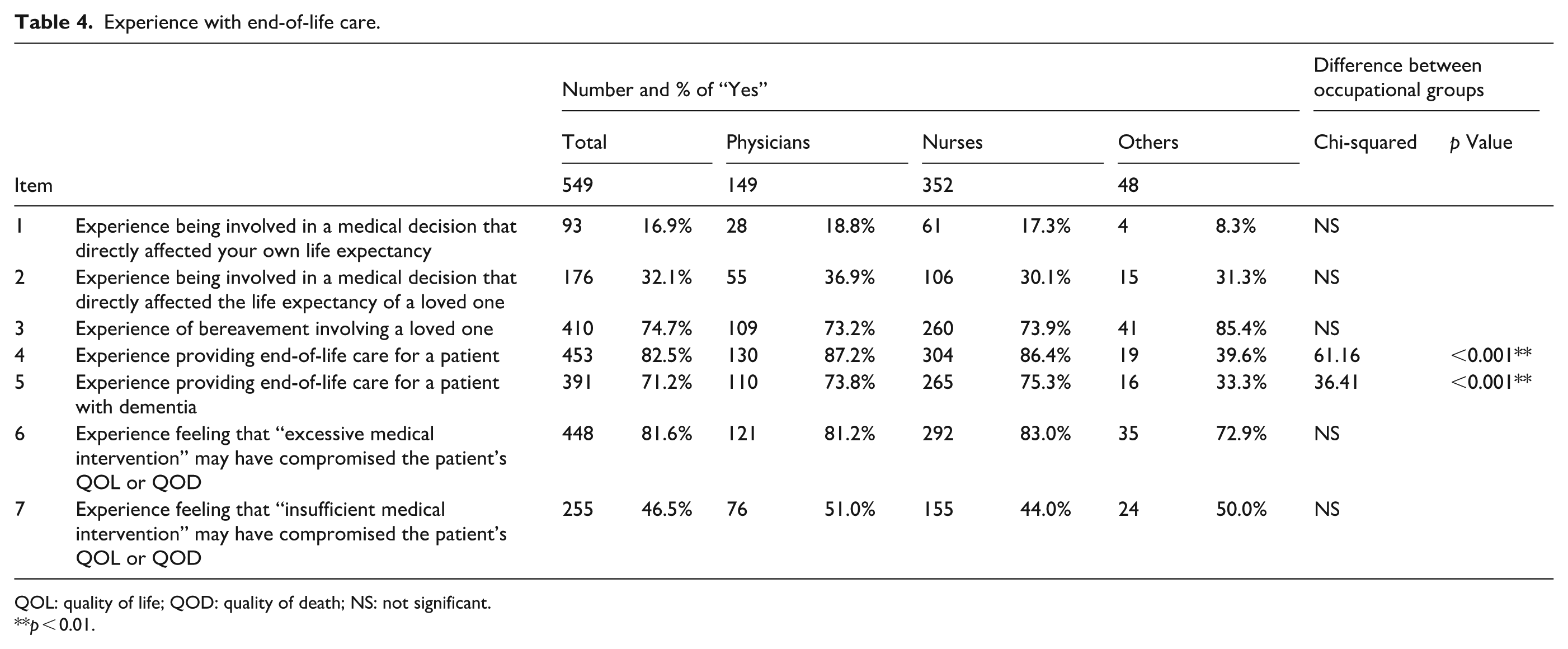
QOL: quality of life; QOD: quality of death; NS: not significant.
p < 0.01.
A significant difference among occupational groups was observed regarding experience with end-of-life care. Participants categorized as “Others” were significantly less likely to have provided end-of-life care, both for patients in general and for patients with dementia, compared with other groups (p < 0.001).
Knowledge of legislation and key ethical concepts underlying medical decision-making
Knowledge of legislation
Participants’ understanding of legislation is summarized in Table 1 (L1–L2). A total of 85.7% of participants incorrectly believed that family members are legally authorized to provide IC on behalf of adults lacking decision-making capacity. In addition, 59.3% mistakenly assumed that adult guardians hold such authority. These misunderstandings varied by occupational group. For family proxies, a significant difference was observed between “Nurses” and “Physicians” (p = 0.037). For adult guardian proxies, a significant difference was observed between “Nurses” and “Others” (p = 0.006).
Knowledge of ethical concepts
Participants’ understanding of ethical concepts related to medical decision-making is also presented in Table 1 (E1–E6). Several misconceptions were observed: 30.3% misidentified a DNAR order issued after family consultation as ACP (E1); 87.5% mistakenly considered the discussion with patient and family that concluded to forgo active treatment to be ACP (E2); 49.3% mistakenly considered the discussion with patient and family that concluded to proceed to surgery as ACP (E3); 70.2% incorrectly believed discussions with patient and family to decide where to discharge constitute ACP (E4); 81.4% incorrectly identified family-only discussions as SDM (E5); and 25.7% misunderstood the scope of DNAR, believing it applies beyond cardiac arrest (E6).
There was a widespread misconception across occupational groups that a discussion resulting in a decision to forgo active treatment constitutes ACP (E2). Overall, 38% of participants labeled as ACP only those discussions that concluded to forgo active treatment, but not those that concluded with proceeding to such treatment. Notably, nurses were significantly more likely than other groups to also interpret discussions concluding in a decision to proceed with active treatment as ACP (E3, p = 0.037), suggesting a broader tendency to equate any current treatment-related discussion with ACP.
Furthermore, “Nurses” more frequently engaged in discussions to decide where to discharge as ACP than other occupational groups (E4, p < 0.001). These findings point to subtle but important variations in how ACP is conceptualized based on professional role, highlighting the need for clearer, shared definitions across clinical disciplines.
Practice of medical decision-making
Vignette A
Treatment choice across occupational groups
Table 5 summarizes the percentage of participants selecting BSC and its variations across occupational groups. In Scenario A1, where participants indicated the treatment they would choose for themselves, “Physicians” were significantly less likely to choose BSC (66.4%) and more likely to choose chemotherapy (20.1%) or gastrectomy (13.4%) than other groups (p < 0.001).
Results of the vignette study A: Percentage of participants selecting BSC.

BSC: best supportive care; NS: not significant.
p < 0.01.
No significant differences across occupational groups were observed in Scenarios A2, A3, or A4. When Ms. A clearly expressed her wish to forgo active treatment (Scenario A2), 94.0% of participants believed BSC is preferable. This rate decreased to 89.3% in Scenario A3, in which her son strongly insisted on chemotherapy, and further decreased to 79.4% in Scenario A4, which introduced a diagnosis of dementia.
Within-scenario comparisons of influence ratings
Table 6 presents the within-scenario comparisons of influence ratings for Ms. A and her son in Scenarios A3 (no dementia) and A4 (with dementia), respectively. Influence ratings represent how strongly each person’s preferences influenced their final treatment decisions. These scenarios specifically evaluated how the handling of a person’s preferences changes after a diagnosis of dementia, independent of any changes in the patient’s actual decision-making behavior.
Results of the vignette study A: Within- and between-scenario comparisons of influence ratings for Ms. A and her son.

NS: not significant.
p < 0.05.
In Scenario A3, 80.2% of participants assigned greater influence ratings to Ms. A’s preference than to her son’s, whereas only 5.7% assigned greater influence ratings to her son’s preference. In Scenario A4, after Ms. A was diagnosed with dementia, 56.7% of participants assigned greater influence ratings to Ms. A’s preference, whereas 15.0% assigned greater influence ratings to the son’s preference.
Overall, Ms. A’s preferences remained more influential even after the dementia diagnosis, with only 15.0% of participants assigning greater influence ratings to the son’s preference than to Ms. A’s. A significant occupational difference appeared only in Scenario A3: “Nurses” were more likely to assign lower influence ratings to Ms. A’s preference, with 6.6% assigning greater influence ratings to the son’s preference (p = 0.029).
Between-scenario comparisons of influence ratings
Table 6 shows the between-scenario comparisons. After the dementia diagnosis (Scenario A4), 27.8% of participants reported decreased influence ratings for Ms. A, whereas 27.2% reported increased ratings for her son. However, 69.5% reported no change in the influence ratings assigned to Ms. A, and 66.4% reported no change in the influence ratings assigned to her son. No significant differences were observed between occupational groups.
Vignette B
Responses to Vignette B showed a sharp contrast between participants’ personal preferences and their professional decisions regarding the withdrawal of life-sustaining treatment, as well as differences among occupational groups in the practice of documented ACP (Table 7). In Scenario B1, Mr. B, now considered to lack decision-making capacity, had previously expressed a wish to forgo active treatment, whereas in Scenario B2, he had clearly stated a preference for full treatment.
Results of the vignette study B..

NS: not significant. *p < 0.05.
Scenario B1: Mr. B had previously expressed a wish to forgo aggressive treatment. Scenario B2: Mr. B had clearly stated a preference for full treatment. (Q1) If you were in Mr. B’s condition, would you consider it acceptable to have fluids and nutrition withdrawn? (Q2) Do you consider it acceptable to withdraw fluids and nutrition? (Q3) Do you consider it acceptable to withhold potential future treatment?
When asked in Q1 whether they themselves would accept the withdrawal of fluids and nutrition if in Mr. B’s condition, 69.5% of participants in Scenario B1 and 41.0% in Scenario B2 agreed. A significant difference between occupational groups was observed in Scenario B2 (p = 0.009), with “Physicians” more likely to endorse withdrawal of treatment for themselves than other groups.
However, when participants considered similar decisions for patients, levels of agreement were markedly lower. In Scenario B1, 40.2% agreed that withdrawal of fluids and nutrition was acceptable (Q2), and 53.5% agreed that withholding future treatment was acceptable (Q3). No significant occupational differences were observed.
In Scenario B2, in which Mr. B had requested full treatment, agreement rates decreased even further: 8.3% of participants agreed to withdrawal (Q2), and 16.4% agreed to withholding future treatment (Q3). Significant occupational group differences were observed for withholding (Q3, p = 0.024), with “Physicians” again showing higher agreement than other groups, although the overall proportions remained low.
Factors associated with respect for patient autonomy
Univariate analysis
To examine factors associated with respect for patient autonomy, the influence ratings for Ms. A and her son in Scenario A4 (with dementia) were set as the dependent variable. The responses were dichotomized into “Prioritizing the patient’s preference” (Ms. A’s preference ⩾ son’s preference) and “Not prioritizing the patient’s preference” (son’s preference > Ms. A’s preference).
Linear regression analyses were performed with the following independent variables: age, sex, occupation, years of experience, seven items of experience with end-of-life care (coded as yes/no), and three continuous variables: the Legislation Knowledge Score, Ethical Concepts Knowledge Score, and the total score of the FATCOD-Form B-J-s.
As shown in Table 8, higher Ethical Concepts Knowledge Scores (p = 0.029) and prior experience of feeling that “insufficient medical intervention” may have compromised a patient’s QOL or QOD (p = 0.029) were both significantly associated with greater respect for patient autonomy.
Results of the univariate analysis.
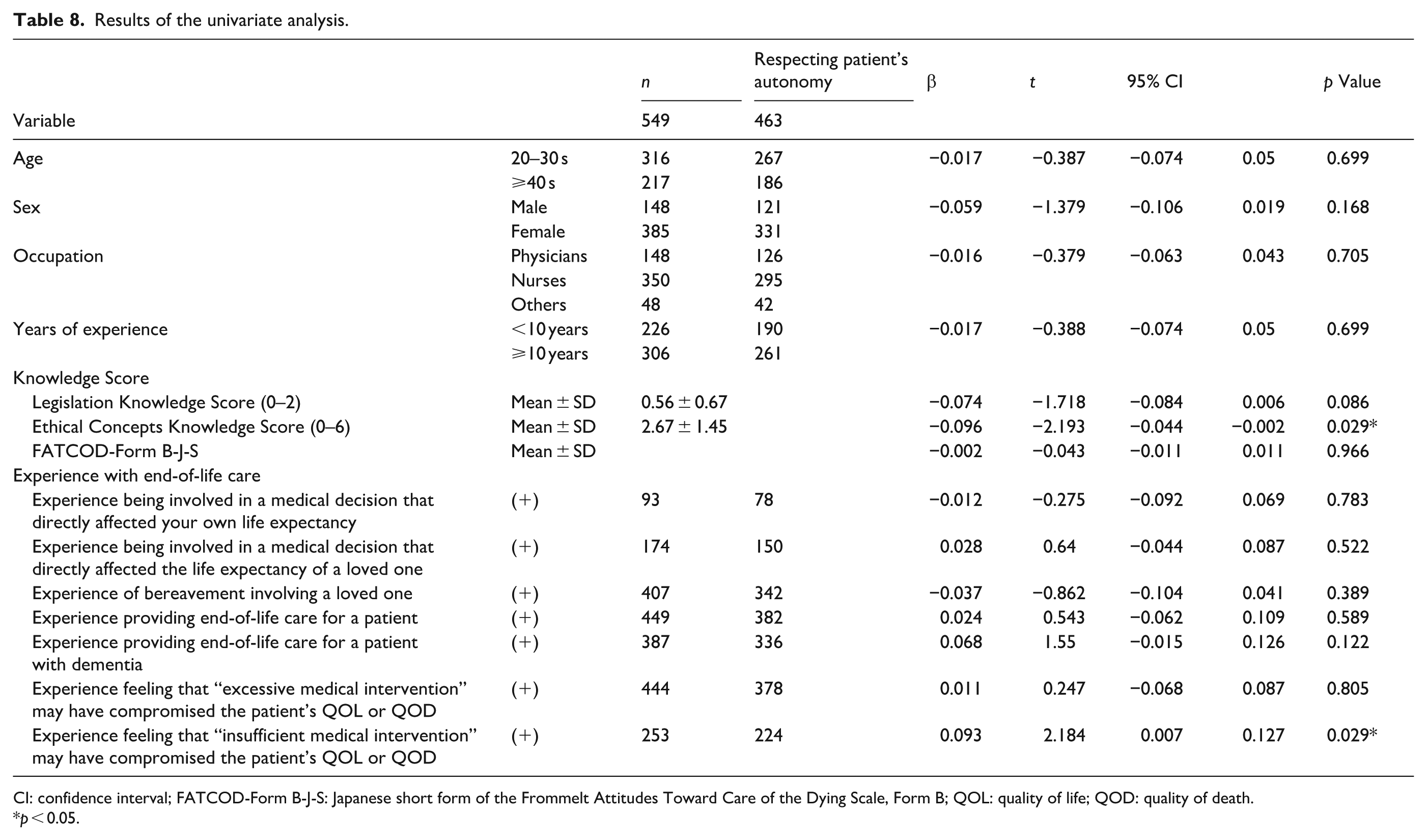
CI: confidence interval; FATCOD-Form B-J-S: Japanese short form of the Frommelt Attitudes Toward Care of the Dying Scale, Form B; QOL: quality of life; QOD: quality of death.
p < 0.05.
Multivariate analysis
A linear regression analysis was conducted using the same dependent variable as in the univariate analysis, with two factors previously identified as being associated with respect for patient autonomy entered as independent variables. In Model 1, sex, occupation, and years of experience were entered; in Model 2, the Ethical Concepts Knowledge Score was also entered; and in Model 3, experience perceiving harm from insufficient medical intervention was further added.
As shown in Table 9, in Model 2, higher Ethical Concepts Knowledge Scores were significantly associated with respect for patient autonomy (p = 0.032). In Model 3, prior experience feeling that “insufficient medical intervention” may have compromised a patient’s QOL or QOD was significantly associated with respect for patient autonomy (p = 0.012), whereas higher Ethical Concepts Knowledge Scores retained a marginal association (p = 0.061).
Results of the multivariate analysis.

QOL: quality of life; QOD: quality of death.
p < 0.1. **p < 0.05.
Discussion
Persistent gaps between policy and practice
This study identified a substantial gap between Japan’s growing policy emphasis on ACP and healthcare professionals’ knowledge and conceptual understanding of medical decision-making. A particularly notable misunderstanding concerned the scope of ACP. Many participants equated ACP with decisions about current treatment rather than its intended focus on future care. Though it is true that discussions about future care often include current treatment options in geriatric medicine, 24 the present findings suggest a fundamental lack of clarity regarding key concepts. Moreover, although ACP is not intended to be synonymous with withholding or withdrawing treatment, 25 38% of participants equated ACP solely with decisions to forgo active interventions. In a context in which policy incentives promote ACP, but decision-making authority remains ambiguous, such misinterpretations risk narrowing ACP into a procedural step to justify treatment limitation rather than a framework for respecting patient autonomy across the continuum of care. Without conceptual clarification, ACP may drift away from its ethical foundation and fail to ensure meaningful patient involvement in decision-making.
Ethical complexities in end-of-life decision-making
The vignette studies illustrated two distinct dimensions of ethical complexity.
Vignette A, in which patients clearly expressed their preferences, showed encouraging trends: most participants prioritized patient wishes even when challenged by family opposition or a dementia diagnosis. However, the absence of explicit ethical reasoning suggests that decisions were often based on intuitive judgment rather than principled understanding. This risks inconsistent interpretation of key terms such as autonomy, IC, and ACP, leading to variations in how patient and family preferences are balanced in practice. For instance, “Nurses” were more likely than other professionals to give weight to family opinions, perhaps reflecting their close daily involvement with both patients and families. Whereas such relational ethics can be a cultural strength, they must not overshadow patients’ right to have their values and choices respected.
Vignette B revealed deeper ethical tensions. Nearly 70% of participants reported that they would personally accept withdrawal of life-sustaining treatment if they were in the same condition, yet only 53.5% judged such withdrawal ethically acceptable for the patient, even when prior wishes supported it. This tendency to agree more readily to withdrawal for oneself than for others echoes findings from previous studies. 23 When prior wishes favored full treatment, support for either withdrawal or withholding decreased sharply, with significant differences observed among occupational groups. Physicians were more likely than other professionals to endorse treatment withdrawal under these circumstances, although overall agreement remained low.
Notably, the greater resistance to withdrawing rather than withholding treatment observed in Vignette B reflects a well-documented phenomenon, despite the fact that these actions are generally regarded as ethically equivalent. 26
These findings highlight the challenges of applying ACP in real-world practice. The present study suggests that healthcare professionals recognize projecting one’s own preferences onto the patient as insufficient, yet rigid adherence to prior statements may also be ethically problematic when clinical circumstances change. Emotional factors are also known to influence medical decision-making. 27 As Morrison et al. emphasize, end-of-life decisions are rarely simple, linear, or purely rational; they are complex, emotionally charged, and highly sensitive to changing conditions.28,29 National survey data further show that many Japanese citizens do not necessarily expect advance directives to be followed without exception. 30
Applying the four principles of medical ethics, autonomy, beneficence, nonmaleficence, and justice,31,32 helps explain why such cases defy straightforward answers. Autonomy requires honoring prior wishes; beneficence and nonmaleficence demand weighing the benefits and burdens of treatment; and justice calls for fair allocation of limited healthcare resources. End-of-life decisions inevitably involve balancing these principles 33 and rarely yield a single “correct” answer. For this reason, interprofessional discussion is recommended 5 ; however, the present findings indicate that the conceptual foundation necessary for such deliberation remains insufficient.
Factors associated with respect for autonomy
Multivariate analysis identified two factors independently associated with greater respect for patient autonomy: (1) greater knowledge of ethical concepts; and (2) personal experience witnessing harm from insufficient medical intervention.
The second finding is particularly noteworthy. In Japan, public discourse on end-of-life care has historically focused on concerns over excessive treatment since the 1970s, intensifying in 2010. 34 Yet the present results suggest that witnessing harm from insufficient medical care may foster greater sensitivity to patient rights and autonomy.
Such experiences cannot easily be replicated in training programs. Ethical knowledge, however, is teachable. The present findings highlight the need for structured, cross-professional education on the ethical and legal foundations of medical decision-making as a patient’s right, complemented by opportunities for reflective learning grounded in real-world experiences.
Implication for education
This study identified three key findings with direct relevance to healthcare education in Japan. First, there is widespread confusion regarding the concept of ACP, particularly its conflation with current care planning or the assumption that ACP equates to withholding active interventions. Moreover, healthcare professionals appear to use ACP-related terminology based on differing conceptual understandings. Second, although patient autonomy is generally respected, a dementia diagnosis alone can shift decision-making authority away from the patient, a pattern likely extending to other mental health conditions. Third, the application of ACP in clinical practice often triggers ethical dilemmas around withholding or withdrawing treatment. ACP does not resolve these conflicts and, in some cases, may introduce new ones. Notably, professionals with personal experience of harm from insufficient medical intervention showed greater respect for patient autonomy, suggesting that experiential learning shapes ethical awareness.
Taken together, these findings highlight the need for formal education to clarify the ethical foundations of medical decision-making, including ACP, so that healthcare professionals understand that medical decisions ultimately concern patient rights, 35 recognize ACP as a tool to respect autonomy rather than a means to eliminate all ethical conflicts, and appreciate that critiques of overtreatment presuppose access to adequate care, whereas the primary duty of healthcare professionals remains the provision of appropriate treatment.
Limitations
This study has several limitations. First, data were collected from a single hospital, which may limit the generalizability of the findings. However, since the institution is a nationally recognized leader in geriatric care and was listed among Newsweek’s World’s Best Hospitals 2025 in the geriatrics category. 36 Given this background, the participating professionals are likely to possess relatively high levels of knowledge and ethical awareness. Therefore, if anything, the present findings may underestimate the challenges that exist in other clinical settings or in general practice. These results can thus be interpreted as reflecting structural and ethical issues that are broadly relevant to geriatric care in Japan. Second, the reliance on self-reported data and hypothetical vignettes may not fully capture real-world clinical behavior. In practice, patient preferences are often less clear than in the scenarios presented, and decision-making contexts are more complex. Though the vignettes provide valuable insights into conceptual understanding and attitudes, they may not directly correspond to actual clinical actions.
Third, a formal power analysis for sample size determination was not performed, as all eligible participants who consented during the survey period were included. This may limit the statistical power to detect small differences among subgroups.
Conclusion
This study revealed a persistent gap between Japan’s policies promoting autonomy-based decision-making and healthcare professionals’ understanding of its ethical and legal foundations. Whereas patient preferences were often respected, misconceptions about ACP, IC, and proxy authority risk reducing ACP to a procedural formality rather than an ethically meaningful practice. To safeguard patient autonomy, particularly for individuals with impaired capacity, systematic, cross-professional education is essential, integrating legal literacy, ethical reasoning, and reflective learning. Without such efforts, ACP may fail to fulfill its intended role, highlighting the urgency for healthcare systems to align policy mandates with ethical and cultural competencies in clinical care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251413285 – Supplemental material for Advance care planning in Japan: Gaps between policy, ethical understanding, and its translation into clinical practice
Supplemental material, sj-docx-1-pcr-10.1177_26323524251413285 for Advance care planning in Japan: Gaps between policy, ethical understanding, and its translation into clinical practice by Kae Ito, Shuji Tsuda, Keisuke Shimizu, Rika Iwakiri, Go Nakajima, Ayumi Hida and Ko Furuta in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251413285 – Supplemental material for Advance care planning in Japan: Gaps between policy, ethical understanding, and its translation into clinical practice
Supplemental material, sj-docx-2-pcr-10.1177_26323524251413285 for Advance care planning in Japan: Gaps between policy, ethical understanding, and its translation into clinical practice by Kae Ito, Shuji Tsuda, Keisuke Shimizu, Rika Iwakiri, Go Nakajima, Ayumi Hida and Ko Furuta in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors would like to thank the staff of the Tokyo Metropolitan Institute for Geriatrics and Gerontology for their participation and the research team members for their collaboration.
Ethical considerations
This study was approved by the Institutional Review Board and Ethics Committee of the Tokyo Metropolitan Institute for Geriatrics and Gerontology (approval number: R24-126; March 11, 2025).
Informed Consent
Before the survey began, the aim of the study was explained to all participants in written form, and written informed consent to participate was obtained from each participant. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable, as the manuscript does not contain any individual person’s data in any form (including individual details, images, or videos).
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Health Labour Science Research Grant by the Japanese Ministry of Health, Labour and Welfare (No. 25GB0101). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.