
Abstract
Amyotrophic lateral sclerosis (ALS) leads to death on average 2–4 years after the onset of symptoms. Although many people with the disease decide in favour of life-sustaining measures, some consider hastening death. The objectives of this review are to provide an insight into the following questions: (1) How do people with amyotrophic lateral sclerosis (PALS), their families and health care professionals (HCPs) communicate about life-sustaining and life-shortening options? (2) What are the challenges for all involved in decision making and communication about this topic? To answer these questions, we searched eight databases for publications in English and German on end-of-life issues of PALS. We included texts published between 2008 and 2018, and updated our search to May 2020. Sources were analysed in MAXQDA using deductively and inductively generated codes. After the final analysis, 123 full texts were included in this review. We identified a wide range of communicative challenges and six different and, in part, opposite communication patterns: avoiding or delaying communication on end-of-life issues, openly considering dying and actively seeking assistance, ignoring or disregarding patients’ wishes, discussing and respecting the patients’ wishes, engaging in advance care planning and avoiding or delaying advance care planning. The literature reveals a very heterogeneous response to end-of-life issues in ALS, despite several good-practice suggestions, examples and guidelines. We derive a strong need for harmonization and quality assurance concerning communication with PALS. Avoiding or delaying communication, decision making and planning, as well as ignoring or disregarding the patient’s will by HCP can be judged as a violation of the ethical principles of autonomy and non-maleficence.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) is an incurable neurodegenerative disease, which leads to progressive muscle weakness and spasticity, and problems with mobility, swallowing, speaking and breathing. While 5–10% of people with amyotrophic lateral sclerosis (PALS) have a life expectancy of more than a decade, most of them die on average 2–4 years after the onset of symptoms due to respiratory failure. Cognitive dysfunction, ranging from language deficits to frontotemporal dementia with behavioural and functional impairment, is developed by 5–50% of PALS. 1 Nonetheless, many PALS retain their capacity to make decisions about their care until death. Although a curative therapy is not available, PALS have several options for sustaining life, alleviating symptoms and also hastening death. These options require in-depth discussions and counselling with patients, families and health care professionals (HCPs) in order to make an informed and well-considered decision. 2
Experts and scholars from various countries have developed guidelines for counselling on treatment options and treatment withdrawal, for talking about and planning the end of life3–6 and also for dealing with wishes to die.5,7–11 However, anecdotal and empirical evidence indicates that communication between HCP and PALS about treatment options or the possibilities of hastening death is partly inadequate.12–15 It seems that the recommendations from guidelines or good-practice suggestions are not yet applied in everyday practice in many countries, health care systems and institutions. Therefore, further research on the current practice and implementation of such recommendations is needed, considering especially the view of the people affected. In preparation for a more extensive research project on the experiences and needs of PALS on counselling concerning life-sustaining and life-shortening options, we conducted a scoping review on a range of research questions. Our goal of this entire review was to identify the scope of the literature and existing gaps in knowledge, and to describe the characteristics of different concepts related to our subject. Thematically, in the entire review, we focused on (1) the phenomenon of the wish to die in PALS, (2) its determinants and motives as well as (3) related communication of HCP on life-shortening and life-sustaining options and its professional management. In a previous review article, we gave an overview on steps (1) and (2) in ALS. 16 Here, we present the results on step (3) concerning the communication about life-shortening and life-sustaining options. Therefore, we defined the following research questions for this article:
RQ1. How do PALS, their families and HCP communicate about life-sustaining and life-shortening options?
RQ2. What are the challenges for all involved in decision making and communication about these topics?
Methods
According to the manual of the Joanna Briggs Institute (JBI), scoping reviews can be conducted for various reasons. For us, relevant reasons were to identify research gaps and especially to detect ‘key characteristics or factors related to a concept’ 17 which in this analysis is the end-of-life communication with PALS. Relevant aspects for our project are presented not only in the scientific literature but also in grey literature, newspapers and magazines, for instance, individual experiences of PALS on end-of-life communication. Since we did not want to miss these facets, we decided to include all types of texts, which are also methodologically covered by scoping reviews. 17 We developed a review protocol to guide our work, in which we specified the following inclusion criteria:
(a) Content-related criteria
● Publications on death wishes and life-shortening measures in ALS in general (discontinuation of therapy, voluntary stopping of eating and drinking, suicide, assisted suicide, euthanasia, palliative sedation)
(b) Information sources
● Original studies, reviews, guidelines, conference abstracts and posters, case reports and comments, editorials, grey literature, newspaper and magazine articles
(c) Languages
● German and English
(d) Year of publication
● Initially 1998–2018, then changed to 2008 until May 2020
(e) Origin of publications
● Worldwide
Information sources and search strategy
We searched for research articles, reviews, guidelines, conference abstracts and posters, case reports and comments, editorials, grey literature, newspaper and magazine articles in order to achieve an overview of our topic. We selected eight databases with adapted algorithms to cover the perspectives of multiple disciplines: PubMed, LIVIVO, Cochrane Library, PsycINFO, CINAHL, CareLit (nursing), BELIT (bioethics) and ProQuest Social Sciences (Table 1).
Search strategy.

Screening
The number of records was reduced from 1306 to 1091 by excluding duplicates. Two researchers screened the abstracts of 109 (10%, randomized sample) publications independently to assess the eligibility. They discussed the differences in their assessments until they came to an agreement and the differences were resolved. Titles that did not meet all five inclusion criteria were excluded. The full abstract screening process was continued with one researcher each and resulted in 722 titles being excluded. During the screening process, we gained the insight that palliative care and medical options for PALS have changed considerably over the past 20 years, as have the legal situations and the ethical debates in several countries. For example, a new law on advance directives (ADs) was set up in Germany in 2009. Since we wanted to cover the discussions around this change in legislation, we chose 2008 as a cut-off and decided to limit the review to publications from the last 10 years (2008–2018). By a later update (2018–May 2020), we extended the time period to nearly 12 years. This screening process resulted in 197 remaining publications for full-text screening and 213 publications after the update till 2020, respectively (see below).
Data extraction and eligibility assessment
We imported 197 full texts and linked biographical data into MAXQDA 2018. Thirty-nine full texts provided no relevant information concerning the research questions and were, therefore, excluded. After full-text screening, 158 eligible studies remained. In addition, we screened the reference lists of the reviews and guidelines included for further relevant articles, resulting in the inclusion of 15 additional publications. A search update in May 2020 resulted in a total of 40 additional publications so that we analysed a total of 213 texts for the entire review (Figure 1 and Online Supplemental Table). Relevant passages were labelled with codes that we generated deductively and inductively. For this analysis, we refer to 123 texts which were assigned at least once to the main code ‘Communication about life-sustaining measures’ or its subcodes (Table 2). From the subcodes, we developed six different communication patterns, which we present in the following.

Review process.
Overview of text types and study designs included.

Results
Challenges in the communication about life-sustaining and life-shortening options and decision making
The communication about the disease progression, therapy options, end-of-life issues and related decisions is challenging for all involved for several reasons. Representative examples of challenges for patients, family members and HCP as identified in the publications are linked to the topics shown in Table 3.
Challenges for patients, family members and HCPs identified in the publications.

HCPs, health care professionals; PALS, people with amyotrophic lateral sclerosis.
The topics in the first column do not present codes of data analysis but were developed afterwards in order to categorize the challenges. Superscripts refer to the publication that contained the challenge described. Some publications did not clearly specify which of the groups concerned faced the challenge. We had difficulties in consistently assigning these challenges to the three groups of people. In our opinion, it would be also misleading, because if a challenge is reported for one group, the challenge may well exist for another group, although we did not find any evidence of this.
This extensive list reveals severe challenges concerning communication and decision making about end-of-life situations in ALS. Besides, our data analysis shows that various stakeholders use different communication patterns in these situations. By the neutral term ‘pattern’, we understand on one hand more or less reflected active strategies and on the other hand a rather unintentional behaviour. We identified the following different communication patterns in the publications:
Avoiding or delaying communication;
Considering dying and actively seeking assistance;
Ignoring or disregarding patient’s wishes;
Respecting the patient’s wishes;
Engaging in advance care planning (ACP);
Avoiding or delaying ACP.
Avoiding or delaying communication
Since communication about future physical deterioration is accompanied by feelings of loss, fear and grief,46,57,58 communication about it is sometimes avoided by physicians, patients and family members. 46 Instead, a wait-and-see strategy is sometimes pursued.51,59,60 It is reported that decisions on therapy options are only discussed when symptoms occur12,51,61 or when, in the eyes of the people involved, a time is reached 15 and communication is almost inevitable. Consequently, decision making in ALS is focused on present problems rather than on future deterioration and long-term preparations. 4 In addition, some patients refuse to talk about therapy options or delay their decision making until it is too late.62,63 As a result, family members sometimes have to make a substitute decision, for example, about mechanical ventilation. 64 Some patients try to live in the present, deny any change, do not want to think about the consequences of their illness and focus on the positive things in life.4,65–67 Talking about death between patients and their families may also be avoided because it is associated with a loss of hope and a negative attitude. 64 The avoidance of communication is also apparent in the fact that family carers sometimes take the role of a gatekeeper to protect the patient from ‘negative’ information from the HCP 65 or they themselves withhold negative information about the true medical condition of the patient, 38 which leads to interference with the autonomy of the patient. 11
In the publications, several examples of avoiding behaviour by physicians can be found. Practitioners report, for example, that their patients were only told ‘to go home and get their affairs in order’ 68 ,p.2303 by physicians disclosing the diagnosis. In addition, in the context of therapy options such as ventilation, some physicians seem to avoid direct discussions with the patient, and sometimes family carers are asked to convince the patient. 69 Matuz70,71 refers to several studies which reveal that physicians avoid the communication about invasive ventilation (IV) because they assume a negative quality of life (QoL) and fear ethical conflicts or legal consequences if the patient subsequently requests the withdrawal of IV. Mattulat 13 cites a German study from 2003 in which 81% of patients on IV had not been informed about the pros and cons of mechanical ventilation before they were tracheotomized and only 29% had the opportunity to discuss end-of-life issues with their physicians. Crimi et al. 72 describe in their review that physicians do not always consider the preferences of PALS regarding tracheostomy. While some patients are content with their decision, only a minority voluntarily opts for it. Being asked for assisted suicide is another challenge to which some HCPs respond by ending the conversation. 39 According to Johnston et al., 39 it is ethically problematic when physicians reject talking with PALS who request assisted suicide. Even if a physician does not agree morally with suicide assistance, he or she should never abandon a patient but fulfil the moral obligation for the care of this patient. Instead, a good strategy would be to ask the patient what makes life undesirable and to figure out what lies behind the wish to die. 39
Not only physicians but also other HCPs avoid communication about end-of-life options. 73 Besides, such communication sometimes starts late in the course of the disease. The time from diagnosis to the beginning of end-of-life discussions was measured in a quantitative study from Canada. It takes an average of 356 days (SD = 451) to the start of such discussions and 427 days (SD = 475) until, for example, a do-not-resuscitate order is signed. 74 The wide scope indicates that counselling about end-of-life options is not handled in a standardized or uniform manner.
The reasons presented for avoiding and delaying the conversation about life-sustaining and life-shortening options are summarized in Table 4.
Reasons to avoid or delay conversation about life-sustaining or life-shortening options.

Considering dying and seeking assistance
Publications show that patients consider31,62,76–82 and express their desire to die to families and HCPs. Many of them focus on the refusal69,79,83–85 or the withdrawal of mechanical ventilation.28,39,84,86–95 But patients also express suicidal thoughts,54,62,77,78 the desire for assisted suicide1,31,96–100 or the request for euthanasia,1,61,100,101 and the desire for voluntary stopping of eating and drinking,51,54,97,102 for palliative sedation100,103,104 and for not being resuscitated.15,64,88,105 The proportion of PALS who have ever thought of (assisted) suicide or euthanasia is indicated with different rates in the studies. According to a German study, 17% of PALS have already thought of suicide and 10% gathered information about assisted suicide. 62 Another study of PALS from Germany and Switzerland revealed that 42% of the patients interviewed have already thought of suicide and one in two considers assisted suicide. 30 Although PALS think about (assisted) suicide or gather information on how to shorten life, a serious wish rarely arises from it.71,106 However, in the US states of Oregon 98 and Washington, 52 PALS are, after cancer patients, the second most frequent group requesting assisted suicide within the ‘Death with Dignity Act’ since its implementation. Furthermore, according to the data of both combined cohorts, PALS take the prescribed lethal substances more often (77.1%) than the all-cause cohort (66%). 52
Patients generally appreciate talking about end-of-life issues with their physician; for physicians, in turn, certain triggers such as the evolution of the disease, distress or the expressed patient wish are suggested to initiate such discussions by an ALS research group in 2005.31,41 However, there is also some evidence that only a few patients really voice their thoughts on dying to their doctors.30,107 Some PALS prefer to talk about these issues to their family, friends, a lawyer, pastor or a notary,12,30,41,91,93 and involve their family in decision making.67,99 However, a US study with 50 PALS published in 1996 demonstrated that patients who had completed an AD were significantly more likely to have communicated their wishes to their physician and family members.36,75 This result corresponds to the findings from an online survey of people with motor neurone disease (MND) in the United Kingdom: in this study, 75% had completed an AD and 43% had discussed end-of-life issues with a physician or a nurse. 78
There are also individual case reports of patients who, furthermore, participate in campaigning groups 79 or take legal action for their right for assisted suicide. 29 As a magazine article reveals, they talk to politicians or journalists in order to draw attention to their situation. 54 In one case, a British patient gave an interview in the newspaper The Guardian about his intention to commit suicide in order to protect his wife from any suspicion after his death. 108
Ignoring or disregarding patient’s wishes
In some cases, PALS’ wishes (expressed directly or in advance) regarding treatment options or their wishes to die are ignored.13,51,54,64,105,109 Some authors, for example, report that the desire to stop eating and drinking has been disregarded, 102 an original plan to refuse non-IV (NIV) or long-term IV has not been accepted,110,111 a request for assisted dying under the Death with Dignity Act in Oregon has been denied by a church-sponsored nursing home 96 or a will not to be resuscitated has not been respected.15,36,38,64,105
Veronese et al. 69 report that some patients who decided against IV change their mind and agree during an emergency situation because they are only offered the alternative of dying without being informed about the potentials of palliative care. Some studies reveal that family members or HCP influence therapy decisions so strongly that the patient’s will is disregarded.38,93,110 In some cases, family members do not accept the PALS’ wish to die and do not support them.39,54 A reason for not complying with an AD or other ACP tools is that HCPs are not aware of them, for example, during hospital admission. 109 In addition, the legal framework can prevent the patient’s will from being enforced, for example, if certain options are not covered by law in the respective country, such as the termination of ventilation in Poland and Japan.95,112,113 Rabkin et al. 95 reveal in a comparative study on the role of neurologists in the decision-making process for IV that 71% of the US neurologists surveyed asked their patients for situations in which the IV should be terminated, whereas only 8% of the Japanese neurologists surveyed did so. Being requested for withdrawal of ventilation, 78% of the US neurologists agreed, but most Japanese neurologists explained to their patients that the termination is (legally) not an option. 95 These differences presumably reflect that legal regulations may cause the patient’s will not to be considered.
Respecting the patient’s wishes
In contrast to the violation of autonomy reported, some publications show respect of the patient’s preferences by HCP. For example, some publications indicate efforts to inform patients about palliative care22,33,62,79 or ventilation, including the option of a future withdrawal.32,86,94,95,114 If assisted dying is requested and legally allowed, as in Oregon, some patients get full legal information and support from their HCP,26,96 but there may also be conflicting regulations of local institutions inhibiting such activities, as a controversial case study shows. 96
Patients and families appreciate a well-organized process, especially if the withdrawal of ventilation is desired, which is described in detail for Germany by Meyer and Kettemann.86,115 An ethics committee is sometimes consulted87,95 or a case conference with the whole care team is held. Experts from palliative care, psychiatry and nursing are consulted24,27,28,87,98,115,116 if, for instance, the team is uncertain about the patient’s decision-making capacity. 52 In one case report from the United Kingdom, legal advice was sought in order to secure the legality of the withdrawal. 28 But the termination of ventilation is not always prepared systematically. The NICE (National Institute for Health and Care Excellence) Guidelines 4 provide evidence that the involvement of team members is judged as still not sufficient. The same guideline indicates that cognitive and behavioural changes are assessed only sporadically.
A publication from Brazil illustrates the ‘narrative competence’ 89 of HCP by presenting a case of a PALS with a locked-in syndrome and resulting communication deficits. Narrative competence is the ‘ability to acknowledge, to absorb, to interpret, and to respond to a person’s story’. 89 Such a competence enables HCP to respond appropriately to a wish to die by reflecting its seriousness and talking about its underlying motives, as shown in a case study by a palliative care nurse. 117 According to another case study, the chaplain’s perspective focuses more on the patient’s beliefs about life and death, his or her understanding of suffering and what that means for his or her spirituality. 96
Carefully assessing the stability of a patient’s wish to die is denoted as an important issue by Murray and Butow 36 since there is evidence that some PALS change their mind during their disease trajectory. Therefore, according to Dreyer et al., 94 the patient’s final decision to terminate IV is proven repeatedly after requesting discontinuation to ensure its durability. A computer-based declaration of the patient’s motivation regarding the withdrawal of ventilation is suggested for reassurance for PALS with communication deficits. 86 In a case study from LeBon and Fisher, 28 the patient was asked to confirm his wish to withdraw ventilation by email witnessed by his HCP.
Several studies reveal that the patient’s wishes are accepted by family members.88,108,109,117,118 A survey of the families of 95 deceased patients from Oregon who had asked for assistance in dying reveals a high level of agreement with the item, ‘I have accepted his death’. 99 According to a longitudinal study by Stutzki et al., 30 family caregivers can well imagine helping the patient to hasten death (31% at baseline and 29% at follow-up), supplying their partner with a fatal drug (70% and 90% over time) and even administering the fatal drug (45% and 67% at follow-up). Family members sometimes feel an obligation to fulfil the patient’s wishes 109 and to communicate them to the HCP.94,105,109 They promote and facilitate the patient’s autonomy, 11 for example, when they seek information about the illness, the end-of-life phase 55 or the possibilities of assisted suicide, 62 in order to prepare the decision-making process. 119 Sources of information are the Internet, self-help groups, HCP or consulting colleagues.103,119
Engaging in ACP
ACP is particularly important for PALS who suffer from diminished abilities to communicate and wish to discontinue life-sustaining treatment under certain conditions, especially in IV users 120 or people with reduced decision-making ability due to frontotemporal dementia.44,90 Therefore, 16 publications mention different tools for ACP offered to PALS (including ADs or other documents, such as a preferred priorities for care document, end-of-life care plan or letter for future care).14,42,60,61,64,70,73,78,87,93,107,109,110,121–123 However, the guidance to conclude such a document is sometimes more61,87,103,115 and sometimes less sufficient. 47 Prevalence rates for completed documents vary according to the time of data collection and national context. In quantitative studies from the United States and Canada, the finalization of ADs is reported between 70% and 90%, as Murray and Butow 36 reveal in their review. A rate of 52.2% is reported for preferred priorities of care documents used for ACP documentation in a UK study 124 and five out of eight patients completed an advance decision to refuse treatment in another UK study. 111 According to Stutzki et al., 30 the proportion of study participants who had written an AD in Germany and Switzerland increased from the baseline (49%) to follow-up (82%), 30 possibly because an AD is more likely to be written in later stages of the disease or because of a raised awareness triggered by study participation. Another study from 2008 in Germany shows a completion rate of 69% for AD. 62 A possible reason for this lower rate may have been that the law on AD was not enacted until 2009 in Germany. In a qualitative British Australian study from 2012, 36 only 2 out of 13 PALS had an AD, 64 but this sample is too small to generalize the results. In Japan, only a few clinics had introduced ACP by 2012. 40
The topics defined in the respective documents are the general refusal of life-sustaining therapy options,12,13,88,125 the rejection or withdrawal of ventilation,38,39,62,84,94,103,107,126 artificial nutrition and hydration,39,93,103,104,107 antibiotic therapy93,127 or resuscitation,66,84,93,107,109,110,117,121,128,129 and the specification of a prospective point in time when ventilation or artificial nutrition should be terminated due to the progress of the disease.104,130
Concerning counselling on ACP, patients and their family members prefer HCP with an established relationship.4,109 The German study from Burchardi et al., 12 albeit grounded on data from 2002 to 2003 before the formal act on ADs, indicates that patients do not want to talk about ADs with their physicians because they associate AD with the renunciation of life-sustaining options and conceive of the doctor as an advocate of life. As case reports from Germany and the United Kingdom reveal, legal advice 103 or the expertise of nurses is sometimes sought. 109 It also occurs that decisions are taken without professional advice or based mainly on other factors. 131 Specialized multidisciplinary clinical ALS services provide a supportive environment for decision making, disease-specific information about therapy options, print and Internet resources, and the opportunity to discuss ACP with experts.4,22,60 However, if the decision-making process is not well organized, for example, if different disciplines repeat the same information several times, patients and families can feel overloaded or confused. 55 There are also supporting online decision aids (‘Making your wishes known’) to generate an AD or prepare the ACP process and discussion with family members and HCP. In a study by Levi et al., 120 computer-based decision aids were introduced to improve end-of-life communication about treatment preferences. The intervention resulted in a significantly higher concordance between the patients’ wishes and treatment decisions of the clinicians, evaluated by clinical vignettes. The clinical teams felt more confident about the accuracy of their treatment decisions; patients felt more satisfied with the decision support, showed better knowledge of ACP and presented lower levels of decisional conflicts and higher levels of self-determination. 120 However, ACP requires time for HCP to schedule, which can be particularly challenging when a patient’s condition progresses rapidly. 4 The practice to simply hand out an AD form to patients without giving further information or advice is not appreciated by one participant in Markarian’s study. 18
The time to start ACP is handled differently. In a British study, 9 out of 11 PALS had completed preferred priorities of care document between 2 and 12 months before death, mostly in the presence of family members and an HCP (MND specialist, district nurse). It was considered helpful that patients were able to communicate verbally and without a speech computer at that time. 109 A study with 10 neurologically ill patients from Hong Kong, 7 of whom had MND, revealed that 8 patients completed an AD at the first consultation with the neuropalliative care team. 107 These studies indicate a relatively late timing of document completion in the course of the disease.
Avoiding or delaying ACP
In a contrary pattern, some physicians recommend not writing an AD until an advanced stage of the disease when certain, for example, respiratory symptoms appear 12 or suddenly worsen. 59 On one hand, physicians fear that the connotation of the AD with death could frighten the patient at an early stage of the disease. On the other hand, they are concerned that patients are not yet prepared to deal with complex treatment decisions concerning the end of life. Therefore, they do not initiate the conversation until the patient sends out appropriate signals considering end-of-life issues. 12 Murray et al. 67 confirm that patients and their families are sometimes not yet ready for end-of-life discussions. In this study, the family members interviewed pointed out that an early initiation of these issues could be too confrontational and emotionally burdensome and could destroy hope. Some HCPs come to similar conclusions by reflecting that various patients want to retain their positive attitude and belief in healing. 114 It is reported in a case study that one patient rejected all attempts for ACP as she pursues a ‘living in the moment’ coping strategy and gradually adapts to her losses. 66 In another case report, a patient was asked to specify when he would like to stop further treatment, but he did not reply. Instead, he continued his active disease management and rejected discussing end-of-life issues. 28 Seeber cited a study by a multidisciplinary ALS team in which only 20% of the patients completed ADs. 59 Some patients are not convinced of the benefits or doubt whether their AD and articulated patient preferences are really taken into account when making decisions. 105 Another possible reason that may prevent PALS from completing an AD might be the difficulty of deciding between life and death. 41 In a German interview study with 15 patients, PALS only considered drafting an AD when hope for recovery had been abandoned. 12 The completion of an AD is also delayed by patients who do not expect cognitive impairment. 85 The difficulty of anticipating suffering in later disease stages and the belief that the evaluation of life-prolonging measures can still change during illness trajectory should also be considered. 85 The reasons of PALS for avoiding or delaying an AD are summarized in Table 5.
Possible reasons of PALS for avoiding or delaying an AD.
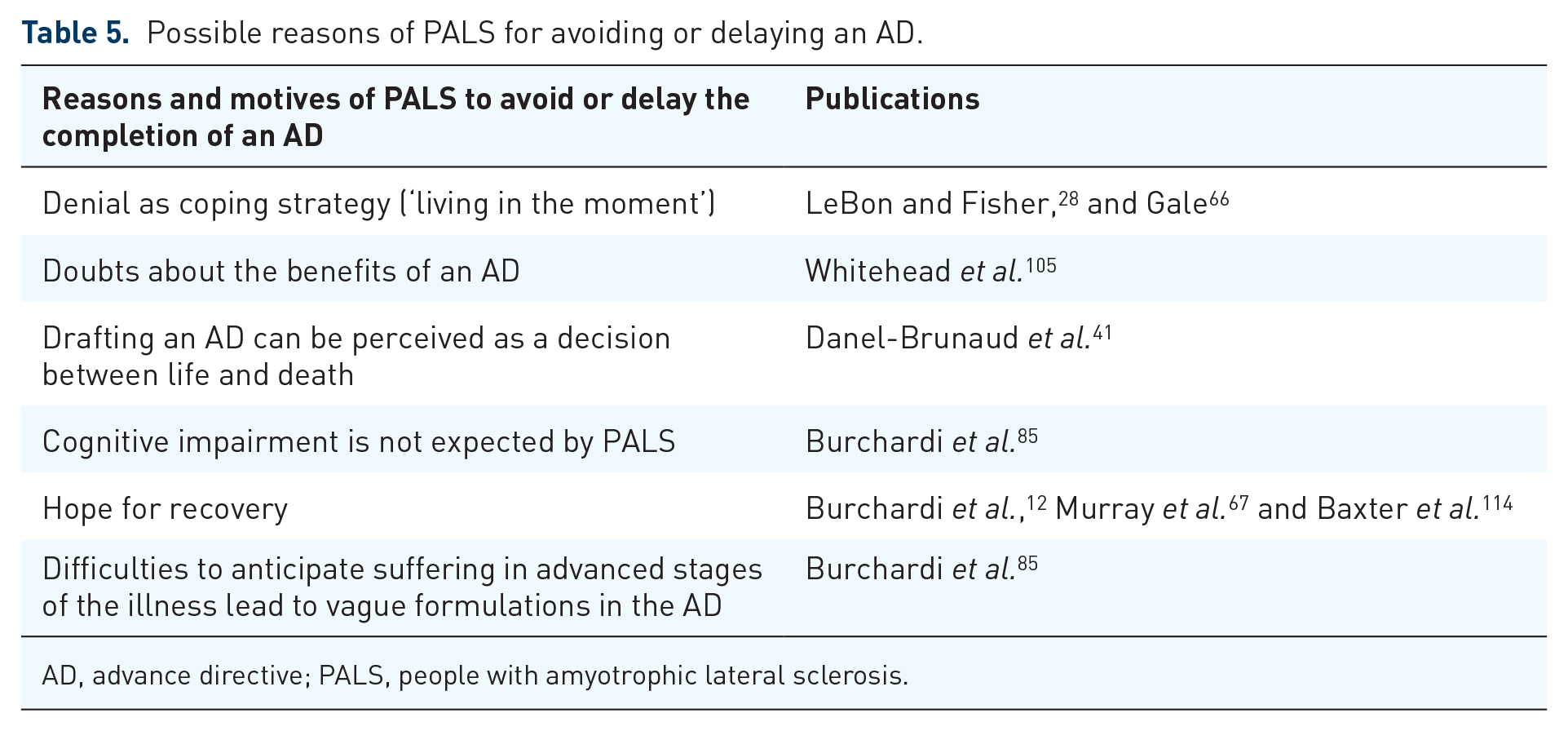
AD, advance directive; PALS, people with amyotrophic lateral sclerosis.
Discussion
This scoping review shows that communication and decision making about end-of-life issues in ALS are characterized by numerous challenges for all involved. Regarding HCP, these challenges relate to different communicative needs of patients, the difficulty of anticipating QoL in later stages of the disease and providing an accurate prognosis, the process of discussing and deciding about life-sustaining measures and end-of-life issues with patients and families, and dealing with the wish to die. We identified six different and, in part, conflictive patterns or strategies used for communication in the literature. They vary due to different reasons: different health care systems and legal regulations, the degree of acceptance of ACP and AD, and personal attitudes of patients, their caregivers and HCP.
We found several guidelines and best practice recommendations for communication about treatment options, ACP, termination of therapy3–6 or the wish to hasten death,5,7–11 in our search for this review3,4,11 and beyond.5–10 Nevertheless, our review demonstrates that some HCPs do not meet the challenges adequately and pursue strategies such as avoiding or delaying communication, and ignoring and disregarding the patient’s wishes. As demonstrated, good practice still coexists with strategies that interfere with patient autonomy. The reasons for this gap between theory and practice should be investigated further because the avoidance of communication, or ignoring or disregarding the patient’s wishes results in a possible harm to the patient. Exemplarily, a patient reports in a qualitative study that the impossibility of talking about assisted suicide with an HCP led him to feel isolated and initiated to take his own actions with potentially dangerous consequences. 79 Another patient stated in an interview that not being involved in decision making had a negative effect on her self-worth. 105 One caregiver indicated that more information and the opportunity to discuss available options would have altered some decisions his wife made. 67 In addition, ignoring or disregarding patients’ wishes is a source of disappointment for caregivers. 64 A severe, negative consequence of the avoidance to inform patients about therapy options, such as IV, is that death is expected much earlier and the patient loses many years of a potentially meaningful life.
The strategy of avoiding or delaying ACP sometimes leads to emergency intubation85,120 against patient preferences. 69 In addition to unwanted treatment, other consequences of unknown patient preferences/wishes are the associated financial burden on families and society and the moral stress associated with unwanted treatment for all concerned, as Levi et al. 120 reveal with reference to several publications.
The empirical results show that avoiding or delaying timely communication, decision making and planning, as well as ignoring or disregarding the patient’s will by HCP can violate patients’ rights considerably and is in conflict with the ethical principles of autonomy and non-maleficence. 132 These principles, along with the principles of justice and beneficence, have been introduced by Beauchamp and Childress as a framework for medical ethics and are widely accepted in medicine. In end-of-life communication and decision making, the principles of autonomy and non-maleficence play a significant role for ethical reflection. 133 In addition to this ethical argument in favour of timely counselling on future care, empirical findings about the value of ACP support our argumentation.
The value of ADs in ALS is described with terms such as autonomy, security, control, courage, dignity 67 and independence. 4 The documents are empowering, comforting 67 and reassuring for patients and families. 4 They can serve as a catalyst for discussions within the family about the patient’s wishes and help families to protect them from uncertainty and disagreement when decisions are suddenly required in emergencies. A study with former caregivers pointed out that an AD simplifies the decision-making process by clear input from experts. 67 The completion of an AD also facilitates the acceptance of the illness and inevitable death, 67 and shortens a suffering anticipated by the patients. 13 In addition, talking to others about an AD can encourage patients when they realize that they do not have to face the disease alone. 67 Regarding HCP, clearly documented patient wishes and their regular review include the possibility of checking the validity and applicability of these wishes. 42 All these benefits show that communication about documents, such as an AD, possibly integrated in a more complex process of ACP can be considered as an expression of professional care, which is in accordance with the ethical principle of beneficence. 132
Due to these advantages, a timely communication, decision making and planning is considered advisable and should be recommended. If the patient follows a coping strategy of denial, communication should, nevertheless, be offered whenever an opportunity occurs until the patient is ready to discuss these issues. As a recent US study shows, hospitalization of PALS is a good opportunity for ACP counselling and setting goals of care. The likelihood of completing an ACP document increased significantly with involvement of specialized palliative care consultants in the hospital. 134 However, Hogden et al. 11 presented a model to optimize the decision-making process of PALS by taking into account their cyclic decision-making patterns and the involvement of caregivers. This model incorporates the step-by-step process of coping with the illness of patients and families when counselling on critical decisions during the disease trajectory and seems to meet the communicative challenges for HCP. Further research should examine the effects of different communication strategies on patients and their families. The application of, for example, the Hogden model would be of paramount interest.
Limitations
This scoping review is limited to English and German publications. Consequently, we missed relevant literature in other languages. In addition, our results are based on texts from 2008 to 2020, and within this long period of time, the legal situation and ethical debate have changed in many countries. Due to these multiple changes, we were not able to trace whether or how changes in the legal situation and ethical debates, the publication of guidelines, and changes in palliative care and medical options have had an impact.
In order to obtain a comprehensive overview and reflect, for example, individual experiences of PALS, we have also included non-scientific sources as newspapers or magazines. Such articles can only underline the results from scientific studies; the containing information does not have the same reliability as those from scientific literature. Therefore, the conclusions made in this article always refer to the results of the scientific literature and are not derived from the non-scientific papers. However, the reader should keep in mind that the publications included differ regarding their evidence levels.
Conclusion
The results clearly demonstrate that different approaches towards end-of-life issues in PALS exist. They vary over time not only between countries and health care systems but also due to the individual attitudes, assumptions and convictions of caregivers and patients. We conclude that there is a strong need for harmonization and even standardization, with the aim of quality assurance of end-of-life communication. Although some promising recommendations and suggestions for communication with PALS exist, there still seems to be a vast gap between theory and practice. The individual preferences and values of patients and family caregivers should be of paramount importance. Communication should help to reveal and develop preferences and decisions accordingly.
The existing research suggests that avoiding or delaying communication and decision making on life-sustaining and life-shortening options, and ignoring or disregarding the patient’s expressed will are incompatible with the ethical principles of autonomy and non-maleficence. Therefore, these strategies cannot be ethically justified, even though such communication is challenging and time-consuming for all concerned. HCP should apply existing guidelines for dealing with wishes to die and ACP in their daily practice. Discourses on regional, national and international levels should be continued, and good-practice examples and guidelines on communication with PALS should be extended, especially in countries where such guidelines have not yet been developed. Further empirical studies are needed to detect additional individual or organizational barriers which hinder communication.
Supplemental Material
sj-xlsx-1-pcr-10.1177_26323524221083676 – Supplemental material for Talking about the end of life: communication patterns in amyotrophic lateral sclerosis – a scoping review
Supplemental material, sj-xlsx-1-pcr-10.1177_26323524221083676 for Talking about the end of life: communication patterns in amyotrophic lateral sclerosis – a scoping review by Anke Erdmann, Celia Spoden, Irene Hirschberg and Gerald Neitzke in Palliative Care and Social Practice
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This scoping review is part of the study, ‘PALS-HD: Preferences and needs of patients suffering from ALS concerning options of hastening death’, funded by the German Federal Ministry of Education and Research (BMBF; Grant No. 01GY1715).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.