
Abstract
Background:
Death literacy can act as a public health asset that enables individuals and communities to navigate end-of-life care with confidence and competence. It encompasses knowledge, skills, experiential learning, and social action. In the United Kingdom, low levels of death literacy may hinder equitable care and contribute to avoidable harms.
Aims:
The study had three aims: (i) to assess death literacy in the East of England using the Death Literacy Index (DLI) to inform applied policy research; (ii) to explore sociodemographic and experiential factors associated with DLI scores; and (iii) to examine how various knowledge domains function as community assets or indicate areas in need of targeted intervention.
Methods:
We conducted a cross-sectional survey with adults aged 18 years and over across six areas in the East of England. The survey included sociodemographic questions, the 29-item DLI, and free-text responses. Quantitative analysis used ordinary least squares regression to identify associations between DLI scores and covariates. Qualitative data were analysed using a framework approach, integrating the Quintuple Aim for health care improvement and DLI domains, including an added Relational Knowledge domain to the death literacy framework dimension for the purposes of the analysis.
Results:
Of 1725 respondents, 1224 completed the survey. The mean DLI score was 5.8/10. Experiential Knowledge was the highest scoring DLI domain (mean = 7.3/10); Factual Knowledge scored lowest (mean = 4.7/10). End-of-life training and recent bereavement were strong predictors of higher DLI scores. Qualitative themes highlighted under-resourced support systems, need for improved coordination of statutory services, and importance of Relational and Community Knowledge.
Conclusion:
The DLI can act as a pragmatic tool for guiding civic action and informing public health strategy. Mobilising death literacy requires relational approaches, community engagement, and equity-focused commissioning. Recognising death literacy as both a public health asset and a civic capability can contribute to population health and support sustainable end-of-life care systems. Social capital and collective action are essential to mobilising death literacy at scale.
Plain language summary
Death literacy means having the knowledge and confidence to make informed choices about end-of-life care, both for ourselves and others. This research used the Death Literacy Index to survey adults in the East of England, aiming to understand how well communities are equipped to handle issues around dying, death, and bereavement.
Results show that while many people have valuable personal experience, there are still significant gaps in knowledge and community support. Those who have received training or have cared for someone at the end-of-life tend to feel more confident and capable. The study linked improved community connections, clear communication with health and care professionals, and easy-to-access information to better death literacy.
Participants called for better resources, more public education, and easier access to support services. These findings can help local health teams and community groups design practical support, training, and education programmes that build confidence and understanding around end-of-life care. The research recommends that health services work closely with communities to build trust, share knowledge, and create supportive environments for people facing end-of-life situations. By strengthening death literacy, we can help ensure that everyone receives compassionate, informed care when it matters most. However, it is important to note that most participants were women and from White British backgrounds, which may limit how well the findings reflect the views and experiences of the wider population.
Keywords
Introduction
Death literacy is defined as, ‘a set of knowledge and skills that make it possible to gain access to, understand, and act upon end-of-life and death care options’ (p. 32). 1 When viewed through a public health lens,2–5 promoting death literacy is a necessary component of population health management. 6
Conceptually, death literacy is analogous to health literacy. Death literacy is dynamic and interactive, emphasising the sharing of experiential knowledge across networks of care.7,8 This sharing serves relational and emotional functions by reducing avoidable harms that can accompany dying and grieving, such as loneliness and social isolation. 9 Death literacy acts as a public health asset with social value.10,11
Death literacy represents action-focused ‘know how’ that is socially situated (embedded in specific cultures and places) and operates at both individual and population levels. 1 Understanding its impact therefore requires evaluating both of these contexts. For example, context-specific death literacy attuned to local needs can promote social cohesion (strong social connectedness) and salutogenesis (promotion of health). Since the emergence of the term death literacy, several related concepts have evolved, most notably grief literacy, which elaborates on addressing social understanding and responses to grief and bereavement. 12
Death Literacy Index
Death literacy can be measured with the internationally validated Death Literacy Index (DLI), a 29-item scale. It covers four knowledge domains: Factual, Practical (including Talking support and Hands-on care subscales), Experiential, and Community (including Accessing help and Community support subscales). Each domain is scored separately and then aggregated. Knowledge domain scores along with the total death literacy score are calculated using a scaled mean out of 10. 13 A maximum score denotes high levels of confidence and competence across all four knowledge domains. There have been subsequent iterations of the DLI with adjustments to language and length, 14 and international translations.15–17
International studies report average DLI scores ranging from 4.8 to 6.9 out of 10,15–20 with the first UK survey (2022) showing a mean of 4.76. 18 Higher death literacy has been associated with older age16,18,21 and with end-of-life (EoL) experiences such as providing EoL care, working in health care/palliative care, or volunteering in EoL support roles.14,16,18–20,22,23
Global context
Globally, ageing populations are increasing EoL care needs, with annual deaths projected to rise by over 50% from 61 million in 2023 to 92 million by 2050. 24 Public engagement is essential to sustaining progress in EoL care,25,26 particularly as health systems struggle to meet needs of older people with complex chronic conditions.27,28 The Lancet Commission on the Value of Death highlighted over-medicalisation of dying, especially in high-income countries, where families and communities have been marginalised. 3 It called for a ‘realistic utopia’ in which death literacy empowers individuals and communities to navigate complex death systems and support population well-being.3,10,25,29
Known challenges to mobilising death literacy at a population level
Despite growing need, significant barriers remain. Global uncertainties following the COVID pandemic, international conflict, economic instability, climate change, and declining trust in institutions have formed an ‘uncertainty complex’ that undermines cooperation and preparedness for collective action.30–32 Societies that are reluctant to engage with death create a social dilemma, echoing Ostrom’s concept of balancing self-interest with collective good.33,34 Individuals may avoid EoL discussions or contributing to caregiving in a community context, despite benefiting from community support.33,34 Health systems must address avoidant behaviours and increase opportunities for meaningful participation to enable collective engagement and community action.
National context
UK health policy aims to shift care from hospital to community, analogue to digital, and reactive to preventative. 35 This aligns with the Quintuple Aim for population health management (Figure 1): (i) improve the health and well-being of the population; (ii) improve resource use; (iii) enhance experience of receiving care; (iv) increase well-being and engagement of the workforce (including volunteers); and (v) advance health and care equity. 36 Enhancing death literacy supports all five aims and highlights the societal cost of low preparedness versus the benefits of confident, informed communities. 29 National guidance, including the Ambitions for Palliative and EoL Care framework, promotes community partnerships, particularly through Ambition Six: Each community is prepared to help.37,38 This ambition encourages local systems to build capacity by improving public understanding, confidence, and participation in EoL and bereavement care. 38 It frames EoL care as a shared responsibility.
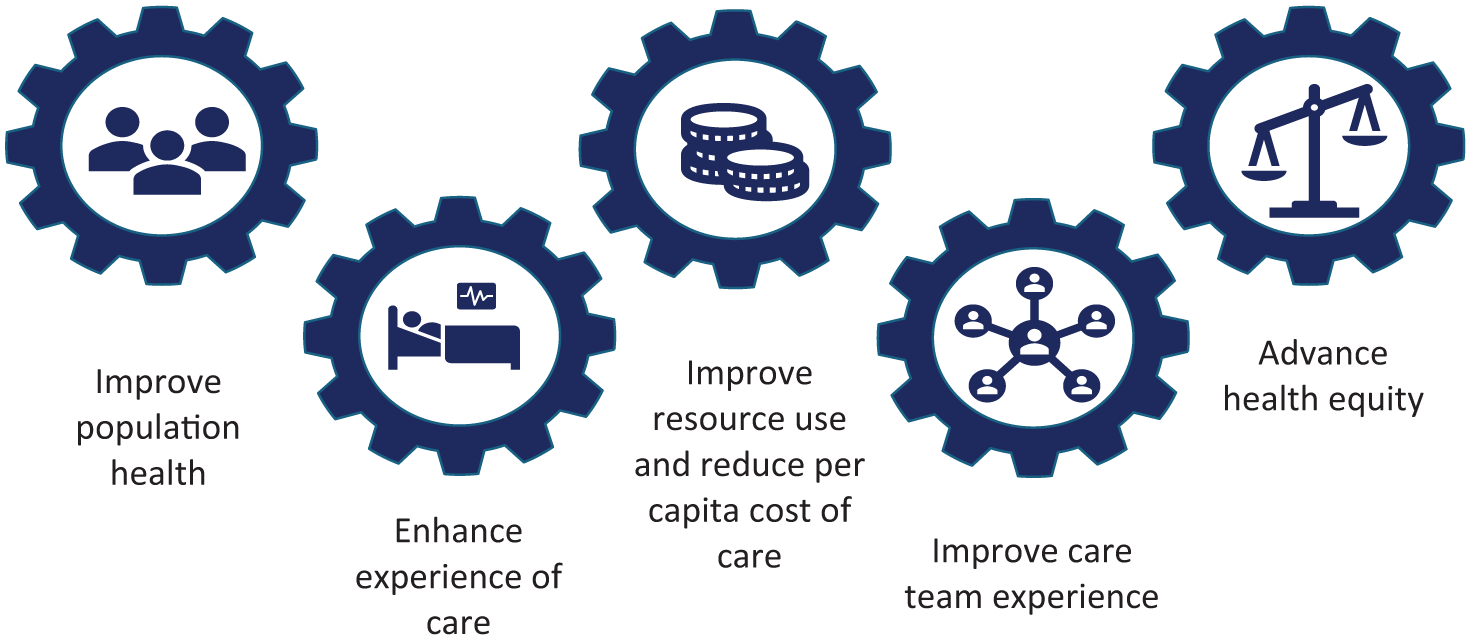
The Quintuple Aim for health care improvement. 36
Building social capital through bonding, bridging, and linking networks that foster trust, reciprocity, and reputation is essential to realising Ambition Six.33,34,39–41 National guidelines reinforce this ambition through Integrated Care Systems (ICSs), regional partnerships of National Health Service (NHS) bodies, local authorities, and community groups.42,43 ICSs are expected to ‘contribute to and encourage public involvement in developing compassionate, understanding communities’ (p.14), 42 yet many have struggled to implement this, underscoring the social dilemma (balancing public value with perceived individual cost) of community engagement around EoL care.34,44
Regional context
This study was conducted in the East of England (EoE) as part of a funded research initiative. The EoE has approximately 6.4 million residents and one of the UK’s oldest populations.45,46 Life expectancy is above average (84 for women, 80 for men), 50 and the population is predominantly White British (85%), with urban pockets of increased diversity. 47 In 2024, the region accounted for over 60,800 deaths: more than 10% of all deaths in England and Wales. 48 Despite relative affluence, the EoE faces persistent inequalities, particularly in rural and coastal areas where poor transport and digital access limit service availability and social cohesion.49,50
Aims
This cross-sectional survey with supplementary qualitative component had three aims: (i) to assess death literacy across the EoE using the DLI to inform applied policy research; (ii) to explore sociodemographic and experiential factors associated with DLI scores; and (iii) to examine how various DLI knowledge domains function as community assets or indicate areas in need of targeted health-promotion and harm-reduction strategies.
Methods
Study design, population, and setting
We employed a cross-sectional survey design with a supplementary qualitative component. Adults aged 18 years or over residing in the six NHS ICS localities in the EoE region were eligible to participate: (i) Bedford, Luton, and Milton Keynes; (ii) Cambridgeshire and Peterborough; (iii) Hertfordshire and West Essex; (iv) Mid and South Essex; (v) Norfolk and Waveney; and (vi) Suffolk and North-east Essex. People under the age of 18 years and those living outside of the EoE region were excluded from the study.
The survey comprised 40 questions divided into three sections. The first 10 questions gathered participant characteristics, including sociodemographic, geographic, cultural, health, and socioeconomic information. They also included questions exploring personal and professional experiences with bereavement and EoL care. These were followed by the 29-item DLI (DLI-29), validated in a UK context, 18 structured into four knowledge domains. As an optional supplementary qualitative component, participants were invited to suggest ways to enhance EoL care knowledge and skills locally using a free-text response. At the end of the survey, participants were presented with their total DLI score and each domain score. All scores were presented alongside UK benchmark data to allow the participant to make a comparison. 18 Participants were then directed to further death literacy information resources. An abridged copy of the survey is given in Supplemental File 1. The survey was piloted with support from the NHS EoE Strategic Clinical Network (n = 5 pilot responses). We prepared the article in accordance with the CROSS (Consensus-Based Checklist for Reporting of Survey Studies) guidelines. 51
Data collection, sampling, and reporting
An invitation to the web-based survey was advertised via social media (X, formerly Twitter). The survey was hosted using Qualtrics XM (Qualtrics, Provo, UT, USA) between 20th October 2023 and 16th August 2024. An extended duration was chosen to allow all ICS areas time to meaningfully participate. Data were collected anonymously. A convenience sample was used with no formal sample size calculation. Anyone accessing the survey self-assessed their eligibility criteria. The home page introduced the study. Participants were asked to read the linked information sheet that was approved in the ethical review process (further details below) before providing their consent to begin the survey using a checkbox. Each survey response was assigned a unique Response Identification code. Qualtrics included a Q_RecaptchaScore to detect possible automated responses.
Statistical analysis
Univariate associations and ordinary least squares regression models were used to examine associations between death literacy and covariates. Within the regression models, bootstrapping with 5000 replications was used to produce 95% confidence intervals and associated p values. Outcomes analysed included the total DLI score and the four knowledge domain scores, all rescaled out of 10.
Covariates included: sociodemographic data (age, gender, sexual orientation), living area, main language, ethnicity, education, and employment; health status (current status and presence of long-term/life-limiting conditions); and EoL experience (through training, or personal experience with others at EoL). Cross-tabulations, and associated measures of association, were used to select between covariates expected to have high correlations to reduce potential for collinearity in the regressions (see Supplemental File 2). Consequently, ‘volunteering or professional experience in EoL care’ was excluded from the analysis; all other variables were included. However, as a sensitivity analysis, we repeated the total DLI regression, replacing the training variable with a form of this variable. We utilised a complete-case statistical analysis conducted in Stata MP 18. 52
Framework approach to qualitative data analysis
We applied framework analysis to the free-text responses due to its systematic and adaptable approach and relevance to applied policy research. 53 It incorporates both deductive reasoning (applying a pre-existing or developed framework to code data) and inductive reasoning (generating new themes or patterns through data-driven analysis and interpretation). 53 It was used here to determine salience and connections in the qualitative data to guide contextual and strategic policy design for population health. The framework approach is not aligned with a particular epistemological viewpoint and takes a broadly realist ontological stance. 54 The five-stage process involves: (i) Familiarisation; (ii) Identifying and developing a conceptual framework; (iii) Indexing data according to the framework; (iv) Charting (presenting evidence summaries); and (v) Interpretation (drawing associations between key themes and concepts identified in the dataset). 53
Familiarisation and identifying a conceptual framework
The first two stages of the framework approach occurred iteratively. Initially, we assessed how well the data fit with the separate elements of the Quintuple Aim. 36 The data mapped adequately with strongest alignment with ‘Enhancing the experience of care’ and ‘Improving population health’. We then explored how well the data mapped onto the four knowledge domains in the DLI: Practical, Factual, Experiential, and Community. The qualitative data mapped onto all DLI knowledge domains.
To improve the fit of the framework, we added a further death literacy domain for the purposes of the analysis: Relational Knowledge. Relational Knowledge acted as a cross-cutting domain reflecting the relevance of death literacy at an individual and collective level. It captured emotional, interpersonal, and communicative understandings about navigating death and dying with others. The justification for adding Relational Knowledge was to highlight the social action feature of death literacy more explicitly. 1 There was a connection with other knowledge domains in the DLI, especially Practical Knowledge involving ‘Talking support’ and ‘Hand-on care’, and Community knowledge involving ‘Accessing support’ and ‘Community groups’. However, Relational Knowledge reflected the dynamic features of death literacy mobilisation involving interdependent human relationships and social interaction. 1
We synthesised the final analytical framework by integrating the Quintuple Aim with the death literacy dimension (including Relational Knowledge), developing a cross-tabulated structure that enabled us to systematically examine the intersection between knowledge, skills, capabilities and values, with internationally accepted aims for health system improvement. 36 The synthesised framework was judged as a good fit for the objectives of the study and provided a clear construct to code the qualitative data.
Indexing and charting
Using a deductive approach, one member of the research team (G.P.) reviewed the dataset multiple times and then indexed using the synthesised framework. Responses ineligible for analysis were quantified and excluded (Figure 2). A second member of the research team (J.B.) independently coded a subset (25%) of transcripts. We compared codes to ensure consistency in the interpretation. We generated evidence summaries using a frequency matrix, and a cross-tabulated chart illustrating the intersection between death literacy domains and Quintuple Aim domains using RAWGraphs. 55 Table 1 lists the indexing framework dimensions and domains. Participant comments that contained references to multiple indexing domains were categorised accordingly.

Participant flow diagram for statistical analysis.
Indexing framework.

Thematic analysis and interpretation
To complement and enhance the interpreted meaning across the dataset, two members of the research team (J.B. and G.P.) coded free-text responses independently within NVivo software (QSR International: Burlington, Massachusetts, USA). After comparing coding matrices, we generated themes inductively from the data. 56 We created a visual summary of the thematic analysis using the Flourish data visualisation platform (Canva, London, UK). Participant comments that applied to more than one of the generated themes were categorised accordingly. We then generated recommendations for contextually sensitive, strategic, localised action at a policy and community level in line with population health management and Ambition Six: Each community is prepared to help.6,38
Results
Participant characteristics
We first explored the characteristics of the survey participants, followed by an analysis of DLI scores and their relationship to key demographic and experiential variables. Among the 1725 participants who initiated the survey, 1224 (71%) completed it and formed the focus of our analysis. Unless otherwise specified, percentages take 1224 as their denominator. Figure 2 details exclusions and missing data.
Table 2 summarises participant characteristics: most were women (84%), and the majority were aged 41–70 years (69%). The most selected ethnicity was ‘White’ (90%), and English was the main language for the vast majority of participants (98%). The largest group of respondents were from Norfolk and Waveney (38%); mapping of response rate by outward code of the postcode is shown in Figure 3. Most participants did not have formal training (58%) and just under half had no personal experience with EoL care (45%).
Participant characteristics (n = 1224).

EoL: end-of-life.
Due to small sample sizes, participants: aIdentifying as a gender other than man or women were grouped together with men; bReporting their main language as any language other than English were grouped together under ‘Other main language’; cIdentifying with sexual orientations other than ‘Heterosexual/straight’ were grouped together under ‘Other sexual orientation’; dReporting ethnicities other than ‘White’ were grouped together under ‘Other ethnicity’; eHighest educational qualification achieved by either or both parent(s); fIncludes those in self-, part-time, and full-time employment; gIncludes students and those unable to work due to illness; hSample size reduces to n = 1220 due to missing data.
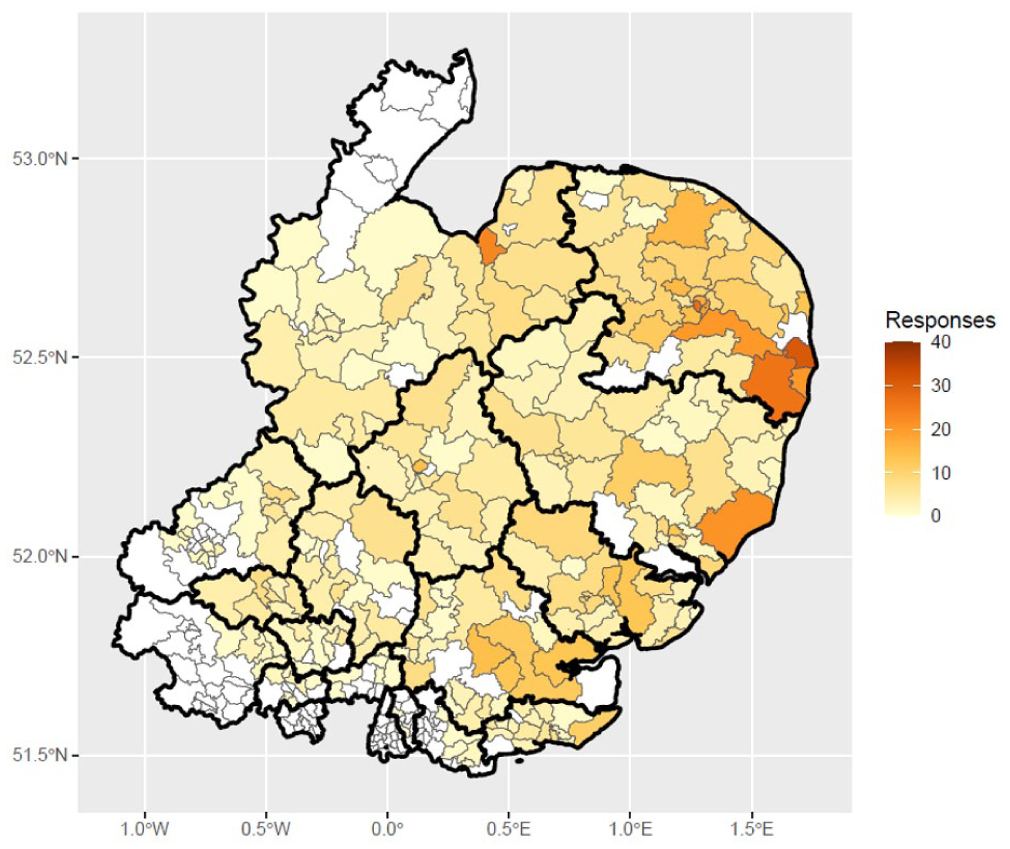
East of England map showing number of respondents (n = 1224) by area ‘outward code’ of respondent postcode.
Table 3 summarises participants’ unadjusted DLI knowledge domain and total DLI scores. The mean total DLI score across the sample, rescaled to a score out of 10, was 5.8 (SD: 2.0). On average, the sample performed best in the Experiential Knowledge (mean: 7.3; SD: 2.0) domain, and least well in the Factual Knowledge domain (mean: 4.8; SD: 3.0).
Descriptive statistics for unadjusted total DLI scores and its knowledge domains (n = 1224).
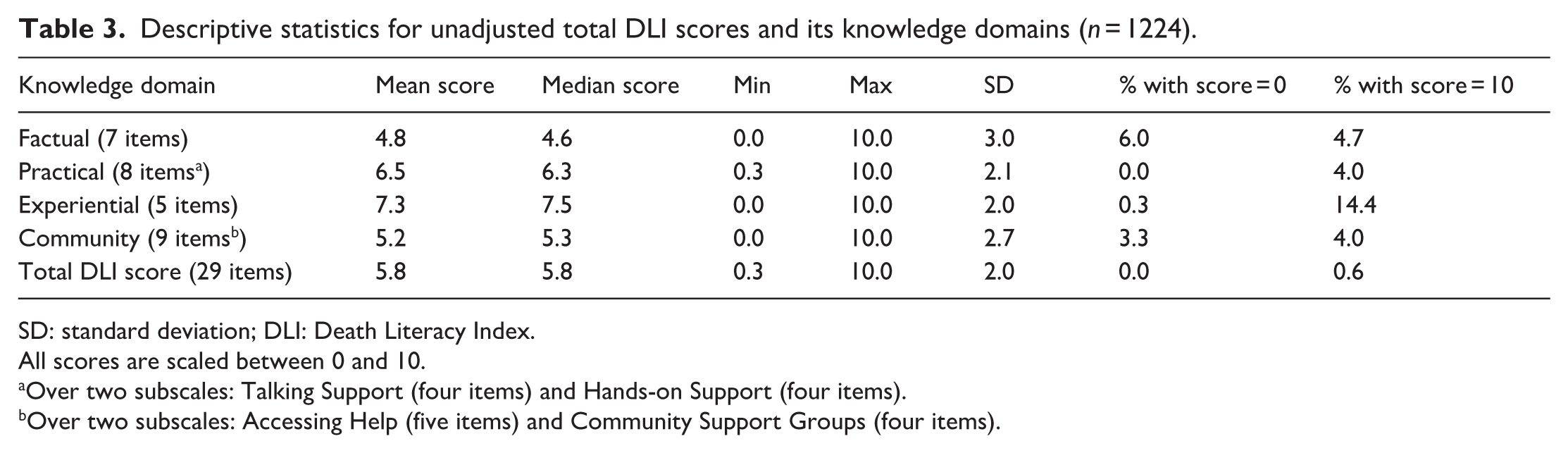
SD: standard deviation; DLI: Death Literacy Index.
All scores are scaled between 0 and 10.
Over two subscales: Talking Support (four items) and Hands-on Support (four items).
Over two subscales: Accessing Help (five items) and Community Support Groups (four items).
Univariate associations
We next explored univariate associations between participant characteristics and DLI scores. Supplemental File 2, Table S2.1 shows univariate tests of association between the covariates and total DLI and the individual knowledge domains. On average, women scored higher than men or other genders (means: 5.9 vs 5.4; p = 0.002). Scores generally increased with age to 51–60 and declined thereafter (significant differences – p < 0.001). There was significant (p = 0.011) variation in scores by area, with highest scores in Hertfordshire and West Essex (mean = 6.4), followed by Suffolk and North-east Essex (6.0), and the other area means ranging 5.5–5.8. However, due to uneven regional representation, this result should be interpreted with caution. Figure 4 shows geographical variation in mean total DLI at a more granular level (participants grouped by outward code of their postcode). Scores broadly increased with improving general health status (significant differences – p < 0.001). EoL formal training was associated with the largest and significant difference in average scores (means: 7.0 vs 4.9; p < 0.001).

East of England map showing total DLI scores by area for n = 1224 participants.
EoL personal experience was significantly associated with total DLI score (p < 0.001). Intuitively, those experiencing someone dying in the last 2 years had on average higher scores (means = 6.0 and 6.4). However, individuals with no personal EoL experience had higher scores (mean = 5.7) than those whose experience was limited to being with someone at EoL who had not yet died (mean = 5.2). Mean differences between levels on main language, sexual orientation, highest parental qualification, and long-term/life-limiting conditions were small (<0.3) and non-significant (all p > 0.1). Differences in ethnicity were larger, but only significant at the 10% level (p = 0.085).
Analysis of the separate knowledge domains revealed similar patterns of mean level differences and statistical significance as observed for the total DLI score. However, differences by area were not significant for Practical Knowledge (p = 0.205) or Experiential Knowledge (p = 0.426). In contrast to the total DLI score, stronger and statistically significant associations were found between Factual Knowledge and both sexual orientation (p = 0.022) and highest parental qualification (p = 0.033).
Adjusted associations between total DLI and covariates
We conducted multivariable regression analyses to examine adjusted associations between participant characteristics and total DLI scores. Table 4 summarises the regression model relating covariates to total DLI score. After adjusting for other covariates, 6 of the 12 covariates had statistically significant associations with total DLI: (i) gender (χ²(1) = 4.8, p = 0.028); (ii) age (χ²(6) = 40.0, p < 0.001); (iii) ethnic group (χ²(1) = 7.9, p = 0.005); (iv) general health status (χ²(4) = 12.8, p = 0.012); (v) EoL training experience (χ²(1) = 407.1, p < 0.001); (vi) EoL personal experience (χ²(3) = 32.8, p < 0.001).
Adjusted total DLI score, OLS regression (n = 1224; r² = 0.32; adjusted r² = 0.31).

OLS: ordinary least squares; DLI: Death Literacy Index.
Due to small sample sizes, participants: aIdentifying as a gender other than man or woman were grouped together with men; bReporting their main language as any language other than English were grouped together under ‘Other main language’; cIdentifying with sexual orientations other than ‘Heterosexual/straight’ were grouped together under ‘Other sexual orientation’; dReporting ethnicities other than ‘White’ were grouped together under ‘Other ethnic group’; eAchieved by either or both parent(s); fIncludes those in self-, part-time, and full-time employment; gIncludes students and those unable to work due to illness irrespective of current personal experience (0.48 vs 0.49). Only personal experience of someone currently dying was associated with a non-significant reduction in DLI score of 0.3 (95% CI: −0.6, 0.1; p = 0.105).
On average, women scored higher by 0.3 (95% CI: 0.03, 0.6) compared to men or other genders. Broadly, DLI scores increased with increasing age group, barring the oldest age group (over 80 years), for whom it declined. However, with only 20 respondents over 80, the latter result should be interpreted cautiously. Compared to other ethnic groups, those identifying as White had 0.5 higher DLI score (95% CI: 0.2, 0.9). As general health status improved, DLI score also improved. EoL formal training experience improved DLI score by 2.1 (95% CI: 1.9, 2.3). This was the largest association observed. Personal experience of someone dying in the past 2 years improved DLI scores by similar amounts,
In the sensitivity analysis, we replaced the binary training variable with professional or volunteering experience (see Supplemental File 2, Table S2.2 for levels): missing data on this variable reduces sample size to n = 1220. Professional or volunteering experience is significantly associated with total DLI (χ²(3) = 494.1, p < 0.001). Compared to no experience, any experience is associated with increased scores: grief and loss experience increased scores by 0.5 (95% CI: 0.2, 0.9; p = 0.002); experience with care of people at EoL increased scores by 1.3 (95% CI: 0.9, 1.6; p < 0.001); experience with both increased scores by 2.5 (95% CI: 2.3, 2.7; p < 0.001).
Adjusted analysis of separate knowledge domains and their association with covariates
To further understand how different factors influence specific aspects of death literacy, we examined adjusted associations across the individual knowledge domains. Summaries of the regression models relating covariates to each of the knowledge domains are reported in Supplemental File 2, Tables S2.3–S2.6, with a simplified presentation of statistically significant associations across these models given in Supplemental File 2, Table S2.7. Generally, where a covariate had a significant association with a knowledge domain, the covariate also had a significant association with total DLI score. Age, EoL training experience, and EoL personal experience were significantly associated across all knowledge domains and have similar differences as seen with the total DLI score.
Broadly, scores increased with age, but for some knowledge domains scores start declining in older age groups.
Gender was only significantly associated with Experiential Knowledge: women scored on average 0.5 points higher than men and other genders (95% CI: 0.2, 0.8; p = 0.003; Supplemental File 2, Table S2.5). Ethnicity was significantly associated with Factual Knowledge (p = 0.009) and Community Knowledge (p = 0.004): individuals identifying as White scored on average 0.7 points higher for Factual Knowledge (Supplemental File 2, Table S2.3) and 0.8 points higher for Community Knowledge (Supplemental File 2, Table S2.6) compared to other ethnicities. General health was not significantly associated with Factual Knowledge (χ²(4) = 4.1, p = 0.383) but was on the other knowledge domains, in which scores increased with improved health status. Geographical area/Integrated Care Board (ICB) locality (χ²(5) = 13.1, p = 0.024) and Employment status (χ²(2) = 8.5, p = 0.014) were not significantly associated with total DLI but were with Community Knowledge.
Qualitative findings
We received 267 free-text comments on ways to enhance EoL care knowledge and skills in the participant’s area in the EoE. A total of 14 comments were excluded from the analysis (n = 6 were ineligible, and n = 8 could not be indexed against the framework), leaving 253 for further analysis (Figure 2). We generated a word cloud and tree map illustrating the frequency of words with a length of four letters or more across the dataset, see Supplemental File 3, Figures S3.1 and S3.2. The word that occurred most frequently in the responses was ‘support’, which occurred 106 times across the data set and in 77/253 (30%) individual responses.
Indexing and charting
The synthesised framework represented a good fit to the data. Free-text responses included in the analysis were indexed against the Quintuple Aim dimension 470 times, and the death literacy dimension 611 times. The indexing frequency distribution is given in Table 5 along with example quotations. Figure 5 illustrates how Relational and Community Knowledge had the strongest mapping against the Quintuple Aim dimension. The chart depicts Relational Knowledge as a fundamental cross-cutting domain. Relational Knowledge indexed comments involved connecting, collaborating, and communicating between people and institutions.
Indexing frequency across framework dimensions and domains with example quotes (Quintuple Aim n = 470, DLI n = 611).

DLI: Death Literacy Index.

Cross-tabulated indexing frequency of free-text comments mapped across the Death Literacy and Quintuple Aim framework dimensions (Quintuple Aim dimension n = 470, Death Literacy Dimension n = 611).
In parallel, ‘Enhancing experiences of care’ and ‘Improving population health’ were the Quintuple Aim domains that mapped most prevalently against all death literacy knowledge domains (Figure 5). This observation reflects the perceived individual as well as collective benefits to increasing death literacy at a population level. 3
The indexing frequency data and example quotations (Table 5) demonstrate the importance of cohesive community networks and the provision of family-centred support. Responses relating to the Quintuple Aim domains: ‘Improve resource use and reduce costs’, ‘Advance health equity’, and ‘Improve staff and volunteer experience’ were indexed less. This should not be interpreted as diminished importance. Instead, it is more reflective of the subjective and experiential nature of participant comments, and the self-selecting nature of the participant sample.
Thematic analysis and interpretation
We generated four overarching themes with a series of sub-themes within each. An example quotation is given for each sub-theme.
1: Resourcing care appropriately
Current community infrastructure was described as under-developed, under-resourced, and under-promoted. Members of the public described a chronic lack of structured support, and a lack of recognition of the role of family carers in the EoL care system.
Sub-theme 1a: Improving care resources and availability
“When looking for help and support in the past regarding this issue all I got was ‘we don’t deal with that, you need to contact blah, blah’ and I’d get the same response from blah blah, so I gave up.”
Sub- theme 1b: Supporting family caregivers and peer networks
“I know the systems, I also know how stretched those systems are. There is a difference between theoretical knowledge and ability to access support at the time of need. And support groups are of no help to carers who cannot get respite to attend them.”
2: Lost in the system
Participants reported feeling excluded, confused, overwhelmed, and unsupported when trying to navigate a complex system of care.
Sub-theme 2a: Improving awareness of services and access points
“Not enough publicity in terms of what support there is – you have to search for it when you are at your most vulnerable.”
Sub-theme 2b: Connecting fragmented services
“It is a mine field, involving different services who do not talk to each other, with lack of funding, compassion and support.”
3: Cultural readiness for death
This theme highlighted a cultural readiness to discuss death and dying that health and care systems may not match. Participants frequently suggested adopting a narrative approach to expanding death literacy: one that goes beyond simply providing factual information.
Sub-theme 3a: Promoting death literacy in everyday life
“I think it should be covered in schools regard[ing] care, hospice, community, etc. as this teaches the child and the parent and opens discussion on life and death.”
Sub-theme 3b: We need to talk about dying, death, and loss
“Encourage people to accept that [death] is a natural end to life rather than a failing of the medical profession.”
4: Communication, care, and dignity
This theme demonstrated communication failures, where a lack of clarity from clinicians had a negative influence on EoL experiences. Participants reported experiences of clinician discomfort with holding EoL care conversations and system pressures that resulted in a person’s wishes not being discussed or not being followed. The role of hospices was discussed frequently. They were portrayed as needed institutions for EoL and bereavement care infrastructure, offering important support services beyond the confines of their physical premises. Participants commented that after death care needs equitable access with enhanced factual and practical support.
Sub-theme 4a: Dignified, family centred dying
“I have supported both parents as they approached end-of-life. [The] GP did not listen to care home advice that my mother was dying that night and was insistent on giving further meds. Mother had [a] LPA [Lasting Power of Attorney] with her with capacious [made with full mental capacity] decision that she should not be resuscitated. [The] GP for [the] care home absolutely refused to accept it.”
Sub-theme 4b: Supporting bereavement and after death care
“I work as a social prescriber within [a rural area]. I have had quite a few patients who are suffering bereavement and quite frankly the services are inadequate within this area of [rural area]. Services that do exist are mainly online and this is not helpful for anybody with learning disabilities or of an older age who cannot access the internet. Since the pandemic more and more services have become telephone based, this is not acceptable. People, especially those grieving, need the human touch and this is severely lacking.”
Sub-theme 4c: Highlighting hospice expertise and role
“Promote hospice services as experts in E of L [end-of-life] skills rather than dying. A wide range of services are available, but as it’s all funded by charity – it needs strengthening!”
Sub-theme 4d: Training professionals for sensitive conversations
“As a student (nurse, paramedic, etc.) I think we need more training on dealing with end-of-life patients – one 1hr skills session isn’t enough to prepare for practice!!!”
Detailed results from the thematic analysis and how themes mapped onto the Quintuple Aim and death literacy framework domains are presented in Supplemental File 3, Table S3.1 along with a short interpretation. Theme titles and descriptions alongside additional example quotations are listed in Supplemental File 3, Table S3.2, and a scaled visual summary of the themes is presented in in Supplemental File 3, Figure S3.3.
Discussion
Death literacy encompasses knowledge, skills, experiential learning, and social action.1,21 This study explored death literacy across six NHS ICS areas in the EoE, using the DLI as a pragmatic tool to inform public health strategies aligned with the Quintuple Aim. 36 We evaluated sociodemographic and experiential factors associated with DLI scores and examined whether certain death literacy knowledge domains function as community assets or indicate areas in need of targeted intervention.
Quantitative findings summary
Current findings echo existing literature and previous UK benchmarking.14,15,18,19,22 Experiential Knowledge consistently scores highest, reflecting how prior experiences prompt self-reflection and influence future approaches to EoL care.1,15,16,18–20,57 Factual Knowledge is frequently lowest scoring, highlighting the need for greater public awareness of, and easy access to, legal, bureaucratic, and pragmatic aspects of palliative and EoL care to reduce current levels of system complexity.16,18,20 Practical Knowledge, involving hands-on care and support, generally scores second highest, especially in cultures with strong family involvement or where training supports confidence and self-efficacy.1,15,16,18–20 Community Knowledge is often low scoring in systems with strong institutional health care or where there is limited peer-led support structures.15,17,18
Demographic, experiential, and training-related associations with death literacy
Higher death literacy was observed among older adults, females, individuals of White ethnic background, those with better self-rated health, and those with formal training or personal experience in EoL care. Structured and experiential learning showed the strongest associations with higher DLI scores. However, the predominance of female and White British participants, and uneven regional representation, limits generalisability. Nevertheless, these findings are consistent with existing literature and highlight the need for inclusive, targeted knowledge mobilisation strategies that actively harness and share learning gained through caregiving or bereavement experiences, or professional exposure to EoL care. While demographic factors are sometimes associated with DLI scores, the evidence indicates that experiential learning and exposure are more consistently predictive of higher DLI scores across diverse populations.14,16,18–23
Qualitative analysis summary
‘Support’ was the word that occurred most frequently in participant responses, emphasising the communal nature of dying and the need for collaboration among individuals, families, and communities (Supplemental File 3, Figures S3.1 and S3.2). Mapping Quintuple Aim elements to DLI domains bridged individual, public, professional, and system-level factors, showing death literacy as both a prerequisite and pathway to improved population health, equity, and resource use.
Adding Relational Knowledge to the analysis framework illustrated the dynamic, action-oriented nature of death literacy (Table 5). 1 Relational Knowledge reflected how death literacy is enacted, acting as a composite across DLI and Quintuple Aim domains (Figure 5). Its prevalence demonstrates the need to mobilise death literacy primarily through human interaction, stimulating social capital and collective action via horizontal associations between policy, practice, and family-centred care.34,58,59
Support needs
Findings indicate that informational resources alone were insufficient for participants navigating the death system. That said, a need to improve Factual Knowledge surrounding a person’s localised death system is a key finding from the survey data. The quantitative results indicate that participants who had received formal palliative and EoL care training were associated with higher levels of death literacy. This suggests training methods are effective in improving death literacy. However, to mobilise death literacy at both individual and collective levels, health and care systems should prioritise supportive relationships across care networks. 29 Four overarching themes generated from participant responses provide insight into how death literacy operates across personal, social, and systemic levels (Supplemental File 3, Tables S3.1, S3.2, and Figure S3.3).
Implications for practice
Principles for mobilising death literacy
Mobilising death literacy knowledge and skills is fundamentally a process and product of social action and social exchange, requiring a system perspective that recognises the complexity, dynamism, and contextual sensitivity of EoL care. 60 Death literacy is shaped iteratively by experience, feedback, and learning within local and cultural contexts.1,20 Health and care policies should therefore prioritise the development of social learning capabilities that enable communities to adapt and respond to the evolving needs around dying, death, and bereavement. 61
While the DLI-29 and its derivations offer a robust and validated means of measuring aspects of death literacy,1,19,20,23 the concept itself extends beyond what any single metric can capture. The DLI provides a valuable framework for assessing knowledge and capability, yet death literacy also encompasses relational, cultural, and civic dimensions that are not easily quantified.34,38 As with many complex social constructs, there is a risk (as cautioned by Goodhart’s Law) that when a measure becomes a target, it may lose its value as a measure. Death literacy mobilisation requires collective community action and the integration of diverse forms of knowledge, including lived experience, practical skills, and emotional insight.
Implementation and system-level recommendations
The recommendations presented in Table 6 are designed to guide a coordinated, equity-driven approach to death literacy mobilisation, aligned with the Quintuple Aim. 40 They are underpinned by a salutogenic ethos to foster confidence, coherence, and capacity within communities, and to reduce stigma and uncertainty around palliative and EoL care. Social capital theory and Ostrom’s framework for collective action highlight the importance of trust, reciprocity, and relationship-building in sustaining cooperation across the death system.38,43 These principles are embedded in the recommended actions, which span community engagement, education, workforce development, and culturally responsive practices.
Recommendations to mobilise death literacy in accordance with the Quintuple Aim.

EoL: end-of-life.
Implementation should be embedded within local and regional ICS health and well-being strategies, with health care infrastructure, local authorities, hospices, voluntary organisations, and educational institutions playing key roles in delivery through partnerships, training, and public education. Framing death literacy as a generative and actionable public health asset enables a complexity-informed response to dying, death, loss, and long-term caregiving. By investing in death literacy mobilisation, stakeholders can enhance preparedness, reduce avoidable harms, and advance equity in EoL care. Embedding these recommendations into practice offers a timely and feasible opportunity to improve outcomes, reduce pressure on formal services, and ensure that each community is better prepared to support its members through death and bereavement.
Two domains of the Quintuple Aim featured less in participant responses: Advancing equity and Improving resource use. 40 It is important to acknowledge that social inequities shape dying. 62 How resources are deployed to reduce structural barriers that limit choice and access to support for people experiencing dying, death, and loss is a key priority. 63 There is a need to bolster peer-based navigation capacity. 63 Death literacy initiatives attuned to the local context are shaped by socioeconomic realities of the present day, as reflected in the UNDP reports.30,31
There is a wealth of death literacy experiential knowledge in the public domain that could be incorporated more systematically to support death literacy mobilisation. In this context, knowledge gained through lived experience can be regarded as a community asset. Facilitating targeted knowledge exchange through social events, community gatherings, intergenerational exchanges contribute to Ambition Six: Each community is prepared to help. 38
In parallel, local authority directories of services enable people at home to know what support opportunities are available in their neighbourhood. In the survey, there were multiple requests for a ‘one stop shop’ to help equip people with what they need in a palliative, EoL, and bereavement context to foster social cohesion and reduce the risk of families feeling overwhelmed or reaching crisis point. Non-clinical infrastructures, such as libraries or community centres can act as resource hubs to support death literacy mobilisation. To monitor progress, a robust systematic evaluation framework is needed that is meaningful to communities and service providers alike.
Strengths and limitations
As a cross-sectional tool, we provide useful data across a large region of England to stimulate collective action in a public health context. By employing supplementary qualitative methods, we incorporated lived experiences to explore interrelated influences of death literacy at personal, social, and systemic levels. The quantitative and qualitative analyses reinforced each other. The framework approach involving deductive and inductive analysis added granularity to the interpretation. The integration of the Quintuple Aim with the DLI domains provided a robust analytical framework. Use of social media enabled access to geographically dispersed populations (Figure 3) suggesting that participant responses are likely to reflect EoE regional views. There are some generic strategic suggestions that could be applied in areas that are deemed culturally similar. However, generalisability and transferability of the results should be treated with caution.
We acknowledge limitations of the study:
(i) The cross-sectional design limits causal inference. Future studies seeking to evaluate death literacy implementation should involve prospective longitudinal designs or experimental designs to strengthen understanding of causal pathways.
(ii) Our regression model accounted for 31% of the variance (Table 4) suggesting there are additional factors needed to further explain determinants of DLI scores.
(iii) A convenience sample may have excluded certain individuals, limiting broader applicability.
(iv) The sample was predominantly female and White British, limiting gender and ethnic diversity.
(v) There was underrepresentation of foreign-born individuals and culturally and linguistically diverse communities.
(vi) The use of an online convenience sample may have limited representation of individuals from certain socioeconomic backgrounds.
(vii) There may have been self-selection bias. Participants more open to discussing death may have been more interested in completing the survey.
(viii) Despite extending the opportunity to participate some postcodes in the EoE were not represented (Figure 3).
(ix) The analysis was conducted on a complete-case dataset (n = 1224), excluding incomplete responses (n = 501). While this approach ensures internal consistency, it does not address potential non-response bias from individuals who did not complete the survey or chose not to participate.
More research is needed to explore how levels of death literacy relate to advancing health equity and improving staff/volunteer experience. These areas require more explicit attention in future evaluations.
Conclusion
This study demonstrates the value of the DLI as a practical, theory-informed tool for identifying community assets and informing public health strategy. Mapping death literacy across the EoE led to 10 actionable recommendations aligned with the Quintuple Aim, providing a clear framework for enhancing EoL care. While improving factual knowledge is important; our findings suggest that informational resources alone are insufficient. Supportive relationships and care networks are essential for meaningful change. Aligning knowledge mobilisation strategies with specific DLI domains enables a more effective, theory-driven response across policy and community sectors. These findings lay the groundwork for collaborative efforts to make death literacy a core component of compassionate, equitable, and sustainable care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524261443547 – Supplemental material for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy
Supplemental material, sj-docx-1-pcr-10.1177_26323524261443547 for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy by Guy Peryer, Krishnan Puri Sudhir, Adam P. Wagner and Jessica Blake in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524261443547 – Supplemental material for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy
Supplemental material, sj-docx-2-pcr-10.1177_26323524261443547 for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy by Guy Peryer, Krishnan Puri Sudhir, Adam P. Wagner and Jessica Blake in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524261443547 – Supplemental material for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy
Supplemental material, sj-docx-3-pcr-10.1177_26323524261443547 for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy by Guy Peryer, Krishnan Puri Sudhir, Adam P. Wagner and Jessica Blake in Palliative Care and Social Practice
Supplemental Material
sj-docx-4-pcr-10.1177_26323524261443547 – Supplemental material for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy
Supplemental material, sj-docx-4-pcr-10.1177_26323524261443547 for Mapping death literacy in the East of England: A cross-sectional survey with qualitative insights to inform public health strategy by Guy Peryer, Krishnan Puri Sudhir, Adam P. Wagner and Jessica Blake in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank: Beverley Pickett, Professor Stephen Barclay, and Dr Eva Lew from the NHS East of England Strategic Clinical Network; Professor Morag Farquhar and Dr Caroline Barry at NIHR ARC East of England; Dr Allan Clark at UEA Medical School; the East of England Macmillan Palliative and End-of-life Transformation Leads, Francesca Light at St Christopher’s Hospice, and the Norfolk and Waveney Compassionate Communities group for supporting the study and enabling manuscript submission.
Ethical considerations
Ethical approval for the study was obtained from the Faculty of Medicine and Health Sciences Research Ethics Committee at University of East Anglia on 14 February 2023 (ETH2223-1343).
Consent to participate
Participants were provided informed consent to participate prior to commencing the survey.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.P.S., A.P.W., G.P., and J.B. were supported by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration East of England (NIHR ARC EoE) at Cambridgeshire and Peterborough NHS Foundation Trust. J.B. was also supported by NHS Norfolk Community Health and Care Trust. In addition, G.P. was supported by NIHR via a Knowledge Mobilisation Advanced Fellowship (Award ID: NIHR302539). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data reported in this article are available from the corresponding author* upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.