
Abstract
Background:
Clinical practice is an important part of nursing education as it helps nursing students transition into competent health professionals capable of providing quality services. However, research studies convey their significant role as a stressor for nursing students when they encounter end-of-life situations during clinical practice. Furthermore, the perceptions of nursing students regarding end-of-life care (EOLC) have not been exhaustively studied in the Ugandan context.
Objective:
This study was conducted to understand nursing students’ perceptions about EOLC during clinical practice at Mulago National Referral Hospital.
Design:
This qualitative study employed a phenomenological approach and was conducted among fifteen nursing students from Makerere University who were assigned to clinical practice at Mulago National Referral Hospital, Kampala, Uganda in 2023.
Method:
Participants were purposively selected for the study from third- and fourth-year undergraduate nursing students. Data were gathered through semi-structured in-depth interviews which were audio-recorded, transcribed, and thematically analyzed using Atlas.ti version 6 software.
Results:
Three main themes emerged from the data: (i) reactions to the physical process of EOLC; (ii) changes in ideas about dying patients; and (iii) student attitudes toward dying patients. Participants described their reactions as chaotic, devastated, and scared during their first encounter with care for dying patients. They also highlighted how their attitudes evolved from unfavorable impressions to positive perceptions as they gained experience.
Conclusion:
In this study, nursing students exhibited divisive attitudes toward EOLC starting with uncertainty and fear, then often growing into confidence and compassion. These powerful experiences show how much EOCL can shape students personally and professionally, highlighting the need for greater support in their educational journey. Further research could help understand how this process unfolds in different settings.
Background
Caring for dying patients is one of the serious concerns of the healthcare systems and settings 1 globally due to the increased prevalence of chronic conditions and patients’ demand. 2 Each year, millions of people face end-of-life suffering, with only 14% of 53 million adults and 4 million children in need of palliative care receiving it. This unmet need is severe in low-income countries such as Uganda, where only 11% of those in need have access to it. 3 Nursing staff and student nurses are the most consistent providers of this type of care.4,5 The nurses provide care in health facilities or at home to help dying patients cope with physical limitations and protect their dignity. The purpose of caring for dying patients is not to prolong life but to control pain and other symptoms so that the quality of life is increased to experience a honorable and peaceful death. 6
Caring for dying patients also plays a central role in bridging communication between patients, families, and healthcare team members, one of the nurse’s key responsibilities. 7 A nurse’s awareness of patients’ values and preferences allows them to support effectively while facilitating communication with the rest of the care team. 8 In this context, the attitudes and perceptions held by nurses significantly influence the quality of end-of-life care provided. 9
Despite the importance of specialized training in preparing nurses for the emotional and professional demands of caring for dying patients, such education is limited for both practicing nurses and student nurses.10,11 Student nurses in particular often lack adequate exposure and training to develop confidence, compassion, and communication skills needed in end-of-life care. 12
Failure to provide end-of-life care to dying patients has adverse effects due to their vulnerability to complications, social isolation, and family abandonment. 13
In Uganda, there is limited research exploring student nurses’ experiences and perceptions regarding care of the dying, yet understanding these perceptions is vital to improving clinical training, encouraging timely palliative referrals and enhancing overall quality of care (Figure 1).
Context of end-of-life care in Uganda.
End-of-life care in Uganda is shaped by cultural beliefs, limited resources, and gaps in healthcare infrastructure. 14 While Uganda has been a leader in integrating palliative care into its national health policy, 15 access remains uneven, especially in rural areas due to a shortage of staff and essential medication like opioids.16,17 Cultural taboos surrounding death often limit open dialogue between patients, families, and providers, 3 and most care still occurs at home, relying heavily on family support. 18
In this context, understanding nursing students’ experience with end-of-life care requires a focus on both emotional and systemic challenges. Roy adaptation model explains how students respond to the stress of caring for dying patients, 19 while Kolcaba’s comfort theory highlights their role in offering relief within constrained settings. 20 Despite progress in policy, students often feel unprepared and emotionally overwhelmed. 18 A phenomenological approach helps reveal how they navigate these experiences and make meaning of their roles in Uganda’s complex care environment.
Preparing nursing students to provide compassionate and competent end-of-life care is a vital component of nursing education. Although several quantitative studies have demonstrated the effectiveness of educational interventions in improving knowledge and performance among practicing nurses, 21 there remains a lack of in-depth understanding regarding how student nurses perceive and internalize these experiences during their training. Additionally, assessment tools such as the Persian version of the program in palliative care education and practice questionnaire-German revised (PPCEP-GR) have contributed to evaluating educational outcomes in palliative care. 22 However, these instruments often focus on measurable outcomes and may not capture the complex emotional, cultural, and personal factors influencing students’ attitudes and perceptions. To address this gap, the present study employs a qualitative phenomenological approach to explore the lived experiences of student nurses, offering deep insight into their perceptions and attitudes toward the end-of-life care. There is a need for nursing students and future nurses to gain the knowledge, emotional readiness, and self-awareness to support dying patients and their families, especially in the Ugandan context, where palliative care access remains limited.23,24 Contributing factors include socioeconomic inequity, shortage of trained staff, and inconsistent access to essential medicines. Nurses’ clinical experience helps them recognize and respond to patients’ needs, often alleviating the burden of caregivers. 25 However, nurses and nursing students face personal, emotional, and cultural challenges in navigating the death experience. 26 The primary research question guiding this study was: How do student nurses perceive providing care to dying patients during clinical placement? The study aimed to document the perceptions and attitudes of nursing students caring for dying patients in the Ugandan context, providing data to inform targeted training and simulations in palliative care. Such interventions are essential to helping students reshape their attitudes and beliefs, ultimately improving the quality of care delivered at the end of life.
Materials and methods
The reporting of this study conforms to the Consolidated criteria for reporting qualitative studies (COREQ): 32-item checklist 27 (see Appendix A in Supplemental Files). A qualitative phenomenological approach was chosen to provide an in-depth exploration of the student nurses’ lived experiences regarding their perceptions and attitudes toward caring for dying patients during clinical practice at Mulago Hospital. This design was selected because it emphasizes understanding individuals’ subjective experiences and emotional responses, making it highly suitable for exploring complex and sensitive topics such as end-of-life care.
Study design
We employed a descriptive phenomenological design, as outlined by Husserl, to capture participants’ perceptions and attitudes toward caring for dying patients, while minimizing researchers’ bias through bracketing. This approach allowed us to describe the phenomenon in the participants’ own terms, free from our own conceptions, which is essential in phenomenological inquiry. 28
Study site
The study was conducted at Mulago Hospital, Uganda’s national referral and teaching hospital affiliated with Makerere University Faculty of Health Sciences. The hospital, with 1790 beds, admits over 140,000 patients and handles approximately 600,000 outpatient visits annually. It was chosen due to its diverse patient population and its role as a primary clinical site for nursing students at Makerere University, ensuring access to participants with relevant and recent experiences with end-of-life care.
Selection of participants
Participants were selected purposively to ensure that they met specific criteria relevant to the research objectives. Inclusion criteria required that they be third- or fourth-year undergraduate nursing students at Makerere University who had cared for dying patients within the last 6 months during clinical practice and who were available and willing to participate. Fifteen participants (nine male, six female) were interviewed, with data collection ceasing upon reaching saturation, the point at which no new insights were emerging. Nursing students who were unavailable or unwell during the study period were excluded.
Data collection
An interview guide (see Appendix B in Supplemental Files) was developed specifically for this study, pilot-tested, and validated by experts in qualitative research. In-depth semi-structured interviews were conducted between June 14 and June 24, 2023, in a private, quiet room at Makerere University’s Department of Nursing, located within Mulago Hospital, Kampala, Uganda. Physical interviews were conducted in English, audio-recorded, and lasted between 45 and 60 min. The lead researcher, who was a health tutor, and the researcher assistant, who was a registered nurse, experienced in qualitative methods, conducted the interviews, and participants signed informed consent forms prior to participation. Open-ended questions, such as “How did you feel and regard the encounter with caring for a dying patient?” encouraged participants to reflect on and describe their experiences in depth. Follow-up probing questions (such as “What do you mean?” and “Can you explain?”) were used to elicit detailed narratives. Field notes were also taken to capture nonverbal cues and contextual information.
Data quality control
To enhance data quality, interview recordings and field notes were reviewed immediately after each session to identify emerging themes. Transcriptions were completed by the lead researcher and expert assistants familiar with the study’s context to ensure accuracy and depth. 29
Trustworthiness (rigors)
The rigor of this qualitative study was ensured through multiple strategies, as outlined below. 30
Credibility
Member checking was used to validate findings, with participants invited to confirm the accuracy of their statements and offer feedback on their interpretations. Peer reviews and consultations with external experts provided additional perspectives and minimized potential biases
Dependability and confirmability
An audit trail documenting all research decisions and procedures was maintained. Peer debriefing sessions further enhanced the reliability of interpretations.
Transferability
We provided rich, detailed descriptions of the study settings, participants’ characteristics, and data collection procedures to allow readers to assess the applicability of findings to other contexts.
Authenticity
Participants were carefully selected based on defined criteria, and data were presented in a manner that accurately reflected the diversity and depth of their experiences.
Data management and analysis
The data were analyzed using thematic analysis, following the approach developed by Virginia Braun and Victoria Clarke. This method involves carefully exploring the data to uncover recurring themes, ideas, and patterns of meaning. The analysis followed six key steps: (1) Familiarizing with the data, (2) coding, (3) identifying themes, (4) reviewing themes, (5) defining and naming themes, and (6) writing up the findings. 31
Each transcript was opened in the Atlas.ti 6 program, and each statement was read and coded line by line. The coding was examined, with some codes being combined and others being modified to create themes. The development of a codebook was followed by the identification of main and subthemes.
Once the initial codes were established, they were carefully grouped based on similarities and connections. This step helped to organize the data into broader categories, which were then refined to develop key themes and subthemes. These themes provided a structured way to interpret the data, enabling a deeper understanding of recurring patterns and meaningful insights.
Ethical considerations
The study was approved by the Makerere University School of Medicine Research Ethics Committee (SOMREC) under Reference number MAK-SOMREC-2023-581. The participants gave written informed consent to participate in the study. The lead researcher informed the Nursing Department Chair at Makerere University and obtained written approval from all participants in the study. The participants were assigned pseudonyms, and the information that they provided was treated as confidential information, and used in a way that made it impossible to link responses to specific individuals. The research team treated respondents with respect, particularly respecting their opinions, including their right to end an interview when they felt uncomfortable.
Results
The results presented in this section were from 15 in-depth interviews conducted among fifteen third- and fourth-year nursing students between 14th and 24th June 2023 who had cared for the dying patients at Mulago Hospital. There were nine male and six female participants (as shown in Table 1).
Participants’ demographic data.

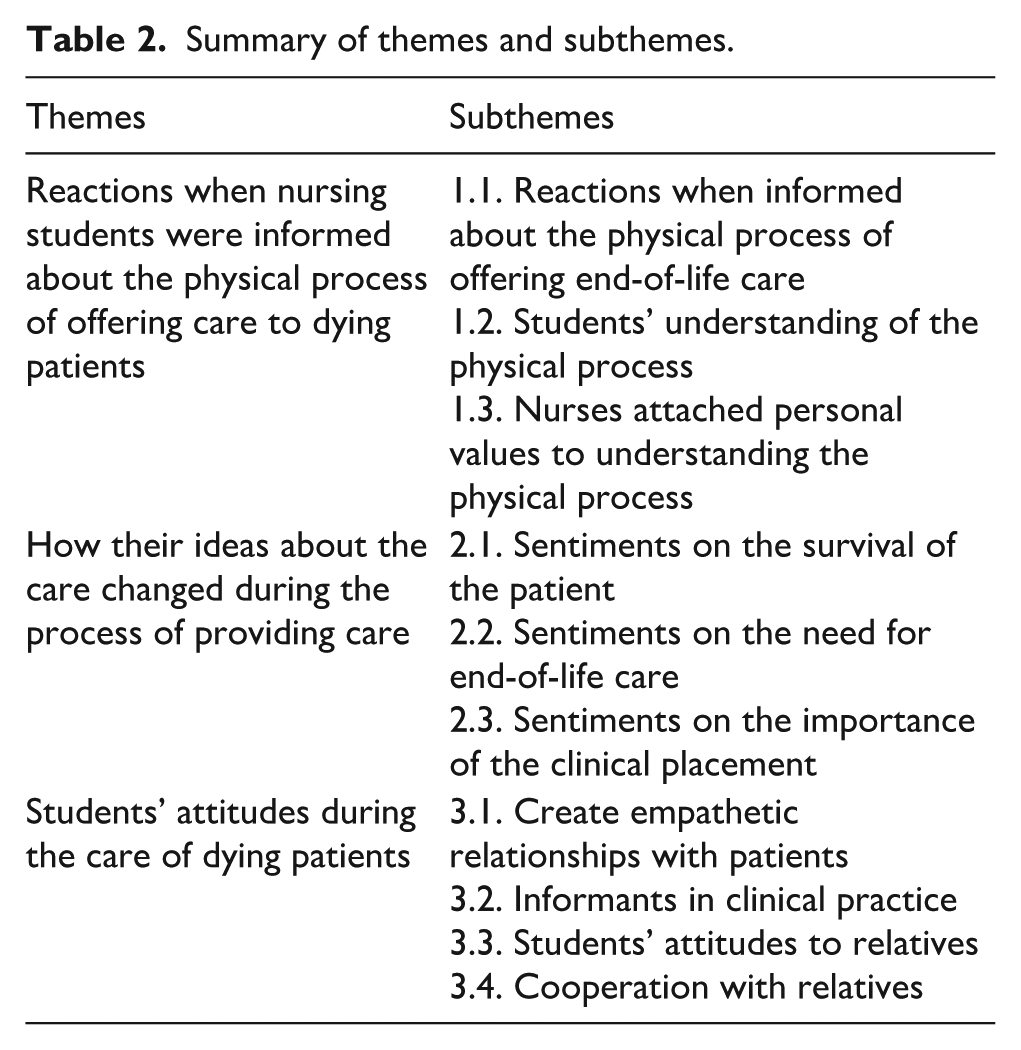
The nursing students’ statements reflecting perceptions and attitudes about the care of dying patients were grouped under three themes, which were derived from multiple codes. The themes that emerged were (1) reactions when nursing students were informed about the physical process of offering care to dying patients, (2) how their ideas about the care changed during the process of providing care, and (3) students’ attitudes during the care of dying patients (as seen in Table 2).
Summary of themes and subthemes.
Theme1: Being informed about the physical process of providing care for dying patient
This theme comprised three subthemes regarding the reactions, understanding, and personal values attached when nursing students were informed about the physical process, as described below:
Subtheme 1.1: Reactions when informed about the physical process of offering end-of-life care
The participants described their reactions as chaotic, devastating, and scared during their first encounters when informed about the care for dying patients. However, some students described positive reactions, including eagerness and expectancy to be part of the medical team.
. . . . chaotic. . . So, to me, I was like, now how am I going to do this to people who are already even giving up to this scenario which is coming ahead of them? How am I going to be able to explain to them it was like, also, even the patient was at that stage where he saw that nothing can be done any further to improve. . . . I thought I was not ready yet to do that. Because I felt I needed more time, you know so that I first watch people do it. And then with the time, I also first do it with assistance, and then at least maybe they can give me but then in my clinical rotation, it was I think, my first week there, and they just told me go and care for the dying patient. And that alone triggered a lot of things in my mind. Oh, yeah. . . . . (Participant 10, female, year 3)
Subtheme 1.2: Students’ understanding of the physical process
The participants had an understanding that the physical process required preparation to handle the situation and knowledge; however, during this clinical placement, they expressed that they were not adequately prepared, felt rushed, and were unsure of what to do during the physical process of caring for dying patients. The participants also thought it was a hard, torturous experience and undermined the relevance of care to the dying patients.
. . .And even like being my first time, first of all, figuring out what to do at that point, became a little hard for me. . . . . . . I felt like since someone’s dying, I felt at some point like, my, my efforts were going to be a little wasted. . . . (Participant 1, male, year 3)
Subtheme 1.3: Nurses attached personal values to understanding the physical process
The participants’ understanding of the physical process was also expressed in their mixed views of personal values. For instance, some participants with positive personal values felt respected, appreciated, trusted, and valued when informed about the physical process of care for the dying patients. Some participants perceived this call as indicating that they were not trusted by fellow health workers or the patient’s family, felt unworthy to care for other improving patients, devalued, not easily acceptable, and confused.
. . .someone has appreciated I value that, yes, I can only participate in this. So, I also feel my presence and the word that yes, if I’m called upon to participate in this caring for this patient who is actually going to lose his life. I felt valued and trusted. . . . (Participant, male, year 4) . . .I felt like they don’t have enough trust in me that I would do something with a patient. . . . (Participant 3, female, year 4)
Theme 2: Change in ideas before and after caring for dying patients
This theme relates to the various changes in views of students regarding caring for dying patients. That included sentiments on survival, need for care, and importance of clinical placement.
Subtheme 2.1: Sentiments on the survival of the patient
The participants revealed changes in their thoughts about the chances and possibilities of survival of dying patients, even though this was not the case before the clinical placement. Some participants who always thought there was something always to be done to alter the dying process got to acknowledge the fact and reality of death as inevitable in some situations.
The participants’ childhood thoughts and beliefs about dying patients also changed and were no longer adaptive to them, such as beliefs that dying patients are bad and can harm caretakers. After this clinical placement, the participants changed their view on this and understood that dying patients are not bad people but deserve care, they don’t hurt people, and caring for them will not kill other people.
. . . . I’ve never believed that somebody can really die when I’m seeing and really, they are dead, you know? So, for me, I thought maybe they were just sleeping. And maybe they would wake up sometime. I never cared much about dying patients. But after this experience, I learned that patients actually die. . . . . . . (Participant 10, female, year 3)
Subtheme 2.2: Sentiments on the need for end-of-life care
In their view of the significance of dying patients, participants reported that before clinical placement they thought this care was unnecessary and that dying patients did not need care after since they were going to die anyway. They were biased and thought the physical process of care is a waste of effort. However, after the clinical placement, their ideas on the need for this care changed, and they realized dying patients have a right to be cared for, and they deserve less painful and peaceful deaths. Hence, they began to handle the physical process of care as an obligation to relieve patients of pain as an offer of painless death.
. . . Initially, I believed that they were wasting time. Because the first patient I was assigned to care for died or was in the process of dying, they did not inform me. So, they just informed me when to modify the oxygen for that individual, when to give this medication, when to provide that, and then later, I had them discuss how the patient is dying and whether we should refer them to palliative care. Yes. . . And I was thinking, if you already know this guy is dying, why are you sending me there again to provide medication and so on? It’s probably best if we halt everything now that he’s already dying. I’ve never been very concerned about dying patients. But afterwards. (Participant 7, female, year 4)
The participants also regarded the physical process of care after clinical placement as a social responsibility, for instance, it provides consolation to family members and health professionals.
. . . . . . . There, you realize that everyone has value and is valued by their family members and so these people have a right to experience or to be treated better in their last days. . . . (Participant 3, female, year 4). . . .it causes breaks. Like many families, the progress of many families comes down, if really, the person that I’ve lost has been key has been the one standing. . . . (Participant1, male, year 3)
Subtheme 2.3: Sentiments on the Importance of the clinical placement
The participants also expressed their change in thoughts on the importance of the clinical placement, from torturous to realizing that it was a learning lesson, which built their confidence to care for similar patients. They acknowledged that the placement improved their nursing skills, and knowledge, and was an opportunity to offer holistic care and obtain great experience in the application of medical care.
. . . . . . . I never cared much about dying patients. But after this experience, I learned that actually dying patients need to be cared for. . . . . (Participant 10, female, year 3) . . .I was just hearing about central lines, but I had actually never cared for a patient with a central line. . .it was my first encounter. (participant 8, male, year 3) . . . . I kept on first of all, learning a lot. I learned a lot. And I kept also, interacting with my fellow students who were with me in their own. . . . (Participant 1, male, year 3)
Theme 3: Students’ attitudes to dying patients
This theme relates to the students’ approaches and attitudes toward the care of dying patients, including creating empathetic relationships, acting as informants in clinical practice, being sympathetic to relatives, and cooperating with relatives, as expressed below:
Subtheme 3.1: Creating empathetic relationships with patients
The participants continued to offer care as they viewed themselves as resourceful individuals, driven by empathy to relieve the patient’s pain and valued the responsibility of care for the sake of relatives. Their empathy was also motivated by mechanisms to overcome productivity shame (guilt feelings if they do not provide care), the desire to give their best effort, and the obligation to ensure a painless death. Participants additionally provided emotional and moral support to patients through positive reassurance and comforting conversations.
. . . . You can’t be avoiding the patient because everyone is busy. . . . So, you have to instead do little more beyond that team. . . . do the basic things because at least we don’t want that person to go in pain. . . . . .You don’t want the relatives to be like, these people didn’t really even do anything. . . . (Nurse participant 5, male, year 4)
Subtheme 3.2: Informants in clinical practice
Student nurses bridge communication gaps between patients and deep connection with relatives. The participants were a source of information for comfort to patients and a means to address loneliness and depression of lonely patients. On a negative note, at times when participants were uncomfortable performing some clinical procedures when overwhelmed by patients’ fragile condition, they preferred to avoid physical presence with dying patients.
. . . . . .It’s not easy when patients are reaching the end of their journey, and their condition is deteriorating rapidly. There was a patient who was nearing the end, and some of us felt unease about being present during those last moments. I remember a fellow participant saying, “I want to be there for them, but it’s hard to see them like this. I don’t know if I can hold myself together.” (Nurse participant, male, year 4) . . . . . . . . . . Our role is to provide care and support, but sometimes the reality hits hard. There was a patient who was really struggling, and we needed to perform a procedure to alleviate their pain. One of us expressed, “I want to help them, but I’m afraid I’ll make it worse or that I won’t be able to handle their pain. It’s so heart-wrenching to see them like this.” (Nurse participant 5, male, year 4)
Subtheme 3.3: Students’ attitudes to relatives
Create sympathetic relationships with relatives
In their sympathy, the participants were protective of the relative’s feelings and hence ensured continuity of care for their sake, so as not to demoralize them. They tried to be considerate in communication with relatives, offered consolation, and kept them hopeful to minimize the perceived impact of the patient’s dying process on the family (such as the loss of a person, breadwinner, family breakage, wasted family efforts), . . . . Relatives often felt so lost and overwhelmed, and it was our duty to help guide them through. I recall telling a family, “Your loved one’s journey is difficult, but we're here to make sure you’re not alone in this. Lean on us, and let’s face these challenges together.” (Nurse Participant 2, female, year 4) . . . . . . . . .Communication with relatives had to be gentle and compassionate. I remember a moment when a family was clearly distraught, and I reassured them, “We understand the pain you’re going through. Let’s focus on the positive memories and the time you have left to cherish together.” (Nurse Participant 3, female, year 4)
Subtheme 3.4: Cooperation with relatives
The participants tried to keep the relatives informed about the physical process of care and encouraged their participation and involvement in basic physical care, such as feeding the dying patient. On the positive note, the participants stated that the relatives were appreciative of the care provided when involved.
. . . . But these people made sure that everything that was needed was provided. . . . they supported the decisions emotionally, they bought all medications, they made sure they fed him, even when I would try to feed him, they would help me. . . . . . .family members even though they may be sad about their patient by eventually dying, they’ll at least appreciate the care that was offered to the patient. . . . (Nurse participant 3, female, year 4)
Discussion
The study highlighted the devastating and frightening reactions of nursing students when caring for dying patients.
The two themes on perceptions of students identified in this study were described as devastating and frightening reactions that contribute to negative consequences in the care of dying patients, especially during first-time encounters. This could be attributed to the limited clinical, physical, mental, psychological, and emotional preparation of the student nurses before exposure to the physical process of care of dying patients. This result is similar to another study that documented that caring for dying patients is a notable stressor for nursing students during clinical practice. 32
In this study, inadequate preparation may have influenced students’ understanding of the physical process as either a hard or torturous experience as expressed by students in this study which later undermined its relevance or positive contribution as a learning opportunity. Studies have documented that there is inadequate provision of end-of-life education to nurses and limited exposure of student nurses, even though early training could significantly prepare them for their future roles across various nursing units. 10
This concurs with a study conducted in Sweden that showed registered nurses struggled with understanding of palliative care and transfer of knowledge into clinical practice. 33 As noted in another study, nursing students need to comprehend how to handle a patient’s death, providing compassionate support to the patient’s family, friends, and loved ones as they grapple with death and psychological trauma 12 since they tend to spend more time at the bedside with patients than other healthcare professionals.
However, the exposure of students to the physical process of care is clearly described in this study as important for building confidence and improving knowledge and skills. This aligns with findings from a study in Australia which highlighted the relevance of exposing students to clinical environments and interpersonal encounters that evoke strong emotions. Such environments serve as effective learning strategies and formal support approaches for knowledge development and emotion management, fostering professional development and enhancing patient care. 34
Exposure of nursing students to the care of dying patients could therefore have positive implications for professional development among health workers which may also result from knowledge exchange and transfer through interactions with senior health workers on wards caring for dying patients. This finding aligns with a study done in Switzerland in 2020, which showed improvement in professional skills among nursing students exposed to care for terminally ill patients. 35
Additionally, understanding the physical process of care and the learning gains from such clinical placements appear to be linked to the personal values, such as respect and trust. For instance, some participants with positive personal values, who felt respected and trusted to care for dying patients, could apply more efforts and lessons learned than their counterparts who felt untrusted and devalued. A meta-analysis conducted in 2016 showed that a comfortable and dignified death is important and depends on nurses’ values regarding respect for privacy, respect, spiritual peace, and hope. 36 Additionally, the findings concur with other studies that emphasize the impact of religious beliefs and faith on attitudes toward death and dying patients, whereby faith in God and the afterlife is often associated with a more favorable stance on death and dying, held by nurses, physicians, and the general population. 37
Therefore, it is important to understand and consider nurses’ personal values and honor them to support nurses during clinical placement and assignments involving the care of dying patients.
In this study, there was a notable shift in ideas about the survival of dying patients, the need for end-of-life care, and the relevance of the clinical placement. The results are similar to findings from another study, which showed that although nursing students often feared dealing with dying patients, focused training and palliative care simulations helped students shift their attitudes and beliefs and improve the care they provided. 38
In this study, the student nurses appeared to come to terms with the reality of death after the clinical placement, unlike before, when they seemed to live in denial of the fact of death. This result concurs with a study 39 that recommended combining the students’ academic grasp of palliative care with their practical encounters with death and dying people can be instrumental in assisting the student to come to terms with the reality that dying and death are a natural part of life rather than something terrifying.
Findings from this study showed that student nurses recognized and valued the importance of end-of-life care after the clinical placement. This aligns with findings from another study conducted in the Seattle-Tacoma area, which showed that nurses perceived patients and families wanted their hopes to be supported at the end of life and often provided this support independently of interactions with physicians. 40
The nursing students in this study finally acknowledged the importance of the clinical placement for their skills improvement. This finding concurs with other studies that have documented consistent satisfaction in clinical placement experiences from student perspectives across semesters and years and significant learning of students in the areas of basic clinical skills, clinical documentation, and collaborative care. 41
Studies have documented that exposure to positive experiences in the care of end of life in a clinical setting yields expected learning outcomes for undergraduate nursing education while negative emotions decrease the quality of care delivered and increase attrition rates. 12
Student attitudes toward dying patients
In this study, nursing students displayed a compassionate attitude which steered them to act as informants for dying patients and cooperate with their relatives. In this study, the factors influencing student attitudes were not explored but some studies have shown that educational programs about death and care for dying patients improved students’ attitude. 26 Also age, earlier care experience, experiences of meeting a dying person, and place of birth affect students’ attitudes toward the end-of-life care. 42
In this study, the nursing students appeared to have developed empathic relationships with patients and relatives after frequent interaction with them, which may have contributed to their resilience as reflected in their continued care even after knowing the patient’s outcome. This is because the nursing students regarded themselves as resourceful persons driven by empathy to relieve the patient’s severe pain, and valued the responsibility of caring for the patient for the sake of the relatives. Empathic relationships between patients and nurses are likely to develop over time due to specific patient needs, nurses’ roles and attributes, and the patient’s reciprocity.
Additionally, the student nurses’ aspiration to provide comfort to dying patients and their spiritual beliefs may have influenced the empathic relationships observed in this study. Studies have shown that nurses tend to continue to do their “utmost” work to facilitate a dignified death by focusing on the patient’s comfort and supporting families, despite the complexities and emotional distress encountered during the end-of-life care and that religious beliefs influence nurses’ commitment and continuation of care. 43
Studies have shown that nurses who develop trusting relationships demonstrate a holistic approach to care, show their understanding of patients’ suffering, are aware of their unvoiced needs, provide comfort without actually being asked, and are reliable, proficient, competent, and dedicated in their care. 44 Similar to other studies, the nursing students in this study were a source of comforting information to dying patients as a means to address loneliness and depression. Nurses can convey consolation to patients to find peace and reconciliation in the final stages of dying, and in doing so may ease some of the existential and spiritual loneliness of dying as they accompany patients in their suffering.
However, it is important to note that information delivery may not always be smooth for nursing students, for instance, contrary to this study, a study in the United States showed that students faced challenges in communicating empathically due to dialectic tensions, the burden of carrying bad news, lack of skills for providing empathy, perceived institutional barriers, challenging situations, and perceived dissimilarities between the nurse and the patient care delivery. 45
This highlights the need to ensure adequate training and mentoring of nursing students in communication skills so that they can provide consolation to dying patients and their relatives. A study from Uganda in 2014 showed that communication challenges with patients and their relatives, staff shortages, and limited knowledge and resources were perceived as emotionally challenging to nurses and hindered their good performance in providing palliative care. 46
Studies have shown that dying patients’ needs beyond medical treatment revolve around empathy, sympathy, compassion, responsiveness to emotional needs, maintaining hope and a positive attitude, and providing comfort through touch as the emotional support to make them feel unique and special amidst their complex social situation. 47
Similar to other studies, the nursing students in this study expressed sympathetic concerns with relatives of dying patients. The participants in their sympathy were protective of the relatives’ feelings and hence ensured continuity of care for their sake in order not to demoralize them. Sympathy to relatives has been documented as a necessary dimension of care to ease the caregiver’s suffering and ensure compassion and satisfaction with the care provided. 48 Relatives tend to appreciate the sympathy given as emotional support, which has a positive impact on both the patient and their relatives, contributing to an improved quality of end-of-life care.
These findings have important implications for nursing education. Educators and curriculum developers can use this knowledge to better support students as they navigate emotionally intense experiences during end-of-life care. Structured debriefing, mentorship, and early exposure to the end of care could help easy initial uncertainty and fear, promoting the development of confidence and compassion. Furthermore, institutions should implement targeted training modules to build resilience and communication skills. Applying these strategies may not only improve students’ professional development but also improve the quality of care they provide to patients and families.
Strengths and limitations of the study
This study provides baseline data for future research in the Ugandan context. The limitation of this study pertains to the bias where by the responses provided by participants might have been influenced by social desirability bias, as well as their inclination to portray themselves positively. This potential influence could have implications for the accuracy and depth of the insights conveyed, potentially resulting in a less exhaustive comprehension of the perceptions and experiences under investigation
Conclusion
In this study, nursing students showed a mix of both positive and negative feelings about caring for dying patients. At first, many of them felt unsure, anxious, and fearful when they learned, they would be involved in the end-of-life care. However, as they gained firsthand experience, their outlook often began to shift. Some students described becoming more confident and developing a deeper sense of compassion for the patients they cared for. While not every student experienced this change in the same way, these insights highlight how meaningful and transformative caring for dying patients can be. These findings suggest a need for nursing programs to incorporate structured support and reflection opportunities to help students navigate these complex experiences. This would require commitment, technical, and financial support from the Ministry of Health, health facility administrators, and professionals for programs that support and meet both systems and patient-centered end-of-life care needs at various health facility levels in the country.
More research is needed to better understand how these experiences shape students’ perceptions over time and whether similar patterns would be seen in different settings.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251383085 – Supplemental material for Perceptions and attitudes of nursing students toward end-of-life care: A qualitative study at a tertiary hospital in Uganda
Supplemental material, sj-docx-1-pcr-10.1177_26323524251383085 for Perceptions and attitudes of nursing students toward end-of-life care: A qualitative study at a tertiary hospital in Uganda by Asha K. Nabirye, Ian G. Munabi, Aloysius G. Mubuuke and Sarah Kiguli in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251383085 – Supplemental material for Perceptions and attitudes of nursing students toward end-of-life care: A qualitative study at a tertiary hospital in Uganda
Supplemental material, sj-docx-2-pcr-10.1177_26323524251383085 for Perceptions and attitudes of nursing students toward end-of-life care: A qualitative study at a tertiary hospital in Uganda by Asha K. Nabirye, Ian G. Munabi, Aloysius G. Mubuuke and Sarah Kiguli in Palliative Care and Social Practice
Footnotes
Acknowledgements
We are grateful to the participants for their willingness to participate in the study and to the Makerere University Nursing Department authorities for allowing us to access the participants.
Ethical considerations
The study was approved by the Makerere University School of Medicine Research Ethics Committee (SOMREC) under REF MAK-SOMREC-2023-581.
Consent to participate
The primary investigator also obtained written approval from the Nursing Department Chair at Makerere University for everyone who participated in the study. The data from respondents were treated with confidentiality at all times. The research team treated respondents with respect, particularly by valuing their opinions, honoring their right to end an interview if they felt uncomfortable, and using careful questioning techniques, particularly when addressing deeply personal or sensitive topics. The purpose and methodology of the study were explained to the participants to seek their informed consent before participation in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The process of data collection was supported by the Fogarty International Center of the National Institutes of Health under Award Number lR25TW011213. However, the publication process was not funded, and the content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sources are not publicly available due to privacy and ethical restrictions. However, it can be accessed upon request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.