
Abstract
Introduction:
The prevalence of Parkinson’s disease (PD) in India is roughly 10% of the global burden, which is a considerable public health concern. The burden on healthcare services in India is substantial due to the variations in PD prevalence and the country’s large population. The unique cultural, ethnic, and social differences in India give rise to distinct needs among PD patients and their caregivers. Neuropalliative care (NPC) is an emerging subspecialty with a holistic approach that requires a unique skill set and the involvement of allied healthcare professionals who play a crucial role in providing integrated services.
Aim:
The objective of this study is to explore the experiences and perspectives of the primary and allied healthcare professionals working with persons with PD in India.
Methods:
The current study employed a qualitative, exploratory, inductive research design, using in-depth interviews with 15 primary and allied healthcare professionals who had more than 5 years of experience working with persons with PD. Participants worked in varied settings such as academic hospitals, rehabilitation services, and tertiary care hospitals.
Results:
The mean years of work experience for the participants were 7.5 ± 3.26 years with a mean number of 30.8 ± 14.8 patients with PD per month. Thematic analysis of the data revealed 5 main themes and 20 subthemes. The major themes revealed were understanding of NPC, the needs of patients and caregivers of PD, barriers and challenges, interventions for patients and caregivers, facilitators, and components of NPC for PD.
Conclusion:
To provide a structured stepped-care approach to managing PD, there is a need to understand the psychosocial and palliative care aspects of PD in patients and caregivers in the Indian context. Adequate training and resource allocation are needed for NPC to be adopted in clinical care.
Plain Language Summary
We intend to explore Neuro-Palliative Care for Parkinson’s Disease in India: A Qualitative Exploration of Healthcare Professionals’ Perspectives. The prevalence of PD in India is roughly 10% of the global burden with a considerable public health concern. The burden on healthcare services in India is substantial due to the variations in PD prevalence and the country’s large population. The unique cultural, ethnic, and social differences in India give rise to distinct needs among PD patients and their caregivers. Neuro-palliative care (NPC) is an emerging subspecialty with a holistic approach for that require a unique skill set with the involvement of allied healthcare professionals who play a crucial role in providing integrated services. The main objective was to comprehensively explore the experiences, perspectives, and challenges faced by primary and allied healthcare professionals in providing care for individuals with Parkinson’s Disease (PD) in India. The current study employed a qualitative, exploratory, inductive research design, using in-depth interviews with fifteen primary and allied health care professionals who had more than 5 years of experience of working with persons with Parkinson’s disease. Participants worked in varied settings like academic hospitals, rehabilitation services, tertiary care hospitals. The mean years of work experience for the participants was 7.5 ± 3.26 years with a mean number of 30.8 ± 14.8 patients with PD per month. Thematic analysis of the data revealed 5 main themes and 20 subthemes. The major themes revealed were understanding of neuro-palliative care, needs of patients and caregivers of PD, barriers and challenges, interventions for patients and caregivers, facilitators, and components of NPC for PD. We concluded that in order to provide the structured stepped care approach in managing PD there is a need to understand the psychosocial and palliative care aspects of PD in patients and caregivers in the Indian context
Keywords
Introduction
Parkinson’s disease (PD) is a complex neurodegenerative disorder that affects a significant number of individuals worldwide, making it the second most common neurodegenerative movement disorder. It is estimated that approximately 0.3% of the world population (i.e., 10 million people) are found to be affected by PD, and in people above 60 years, the prevalence is about 1%. 1 The prevalence of PD in India is roughly 10% of the global burden, making it a considerable public health concern.2,3
The impact of PD extends beyond the physical domain, affecting patients’ psychological and social well-being, resulting in a lower quality of life (QOL), which is influenced by disease stage, severity, duration, and financial security.4,5 The burden on healthcare services in India is particularly substantial due to the variations in PD prevalence and the country’s large population. Furthermore, the unique cultural, ethnic, and social differences in India give rise to distinct needs among PD patients and their caregivers. 6 There is a need for more research focused on the contextual and psychosocial aspects of the illness to better understand the disease in the Indian population. This understanding will lead to the development of treatment options tailored to the specific needs of PD patients in India.
Neuropalliative care (NPC) is an emerging subspecialty with a holistic approach for people with neurologic illnesses requiring a unique skill set. Offering adequate palliative care services is necessary to provide holistic care to the varied and evolving needs of persons with PD and reduce the burden of care for caregivers. 7 This requires the involvement of allied healthcare professionals, such as psychologists, social workers, occupational therapists, art therapists, and speech therapists, who play a crucial role in providing integrated services. The objective of this study is to explore the experiences and perspectives of the primary and allied healthcare professionals working with persons with PD in India to develop and strengthen NPC services for persons with PD and their caregivers.
Methods
The current study employed a qualitative, exploratory, and inductive research design, using in-depth interviews. A semi-structured interview schedule was developed based on the literature review and the research team’s clinical experience. A pilot interview was conducted, and minor changes to the schedule were made. Demographic information was recorded using a simple questionnaire. The study was approved by the institutional ethics committee of the institute where the study was conducted (Proposal No.: IEC-IEC-IHBAS 2022/9/29/V-2).
Participants
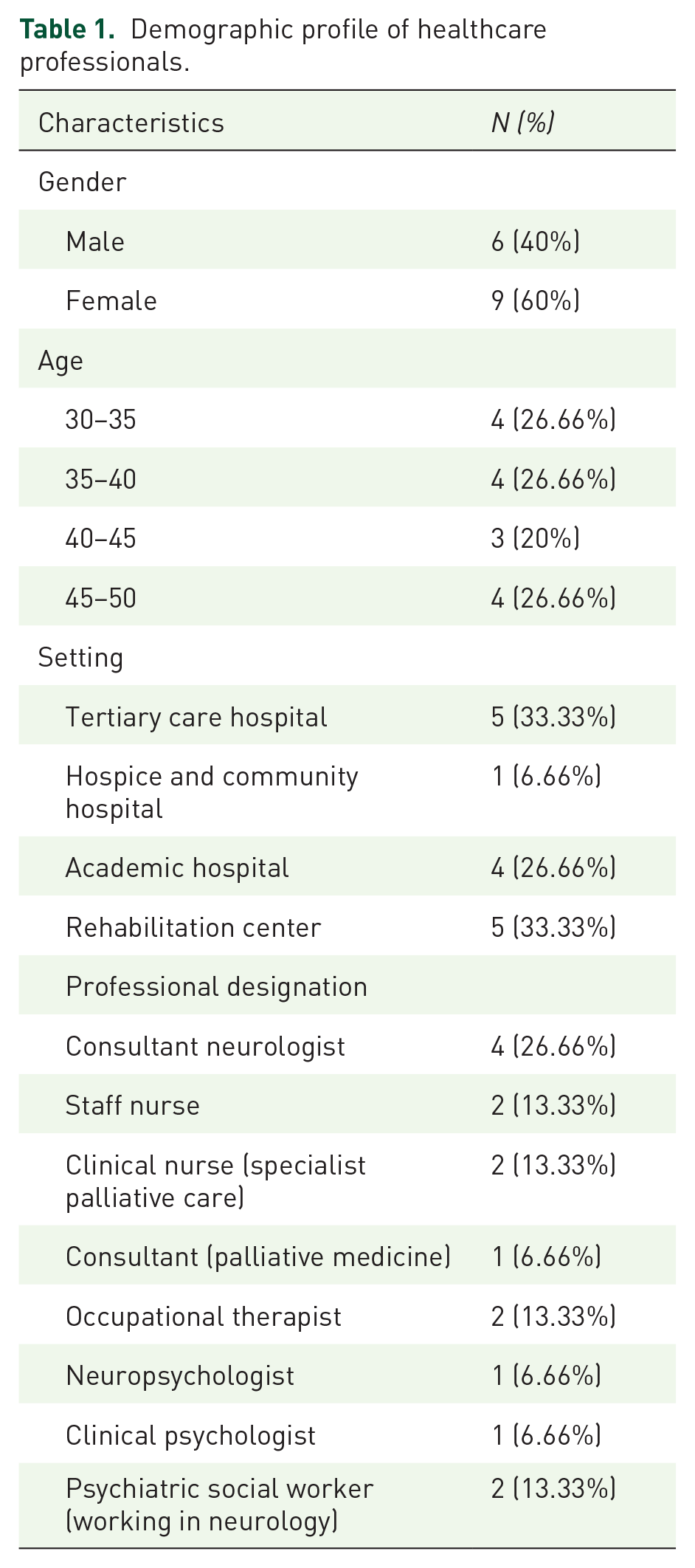
Fifteen primary and allied healthcare professionals who had more than 5 years of experience working with persons with PD participated in the study (Table 1). We used a sample size that balanced the likelihood of thematic data saturation and study feasibility, and allowed the representation of a range of allied health disciplines. The study participants included neurologists with an interest in NPC, psychiatric social workers with experience working in neurodegenerative disorders, neuropsychologists, clinical psychologists involved in the rehabilitation of persons with neurodegenerative diseases, occupational therapists, nursing care staff (providing care for persons with neurodegenerative illness), and palliative care consultants. Participants who provided consent were assured of confidentiality and anonymity and encouraged to express their views freely. The data was collected from September 2022 to May 2023. Participants were contacted personally via email or telephone by a researcher who was not known to any of the participants before this study; this limited personal influence in recruiting participants.
Demographic profile of healthcare professionals.
Procedure
Interviews were conducted by a licensed clinical psychologist with expertise in qualitative research methodology. The interviewer had training in eliciting participant responses and encouraging disclosure and different opinions with gentle probing. With the participant’s consent, discussions were audio recorded and transcribed verbatim. Based on the literature review and clinical experience, our interdisciplinary research team (composed of clinicians in neurology, clinical psychology, and psychiatric social work) developed and iteratively modified the semi-structured interview guide before conducting the interviews. One other neurology expert reviewed the guide to improve clarity and reduce bias. The semi-structured interview schedule consisted of open-ended questions about the definition, experiences, current understanding and practices, needs of patients and caregivers, challenges, barriers, facilitators, interventions and specialized services in Parkinson’s management, and improvement opportunities (Table 2). Each interview lasted from 45 to 60 min.
Interview schedule.
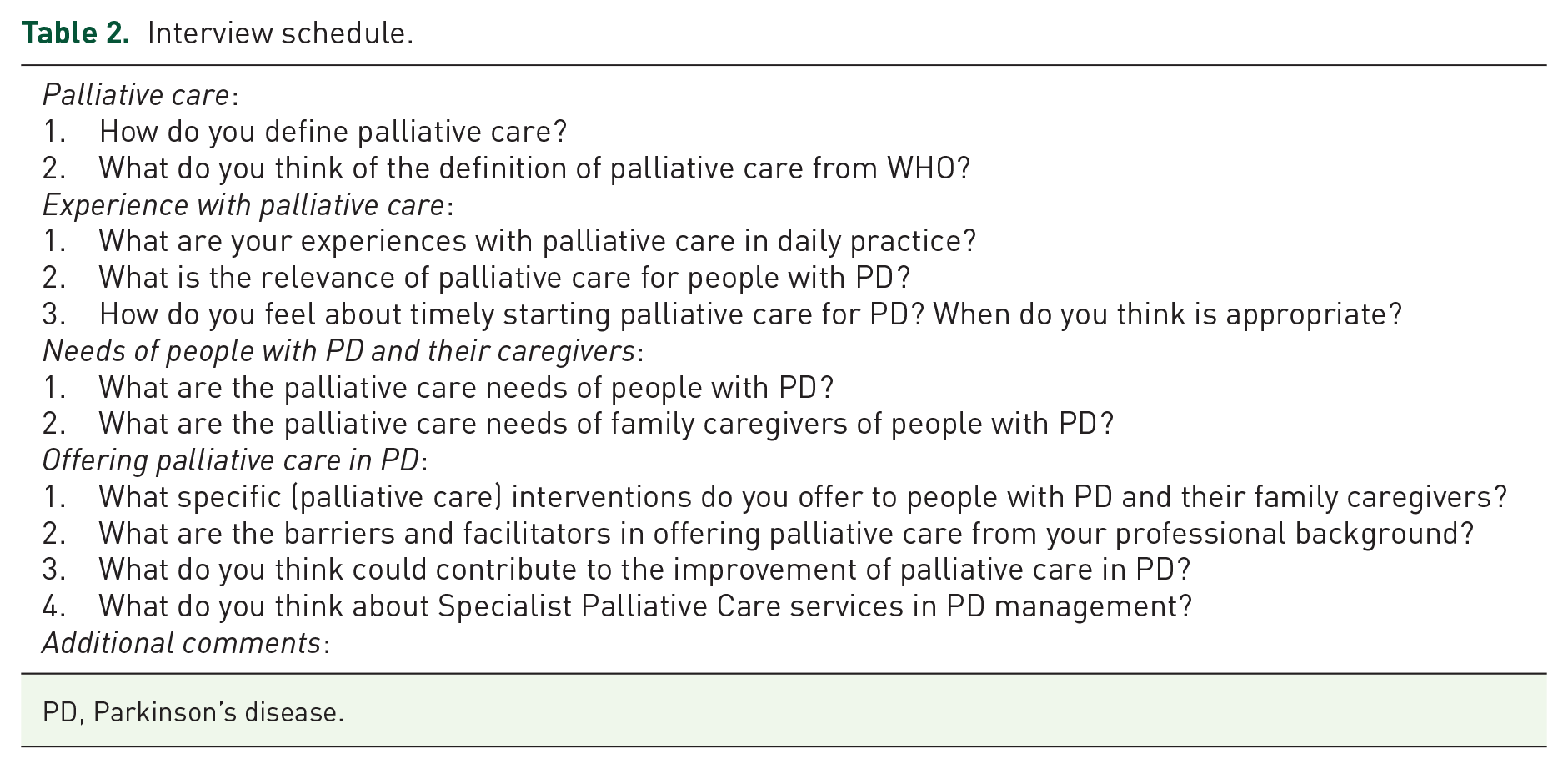
PD, Parkinson’s disease.
Data analysis
We used a thematic analysis approach and analyzed data using the constant comparison method. Two members of the team developed a coding scheme inductively. Using qualitative data analysis software (Lumivero NVivo 10) to maintain an audit trail, team members independently coded anonymized transcriptions (as outlined by Mays & Pope, thereby enhancing interrater reliability). 8 Codes were added, modified or merged iteratively on the coder agreement, and a third researcher resolved discrepancies. For quality assurance purposes, a third researcher reviewed a random sample of 20% of the transcripts and the resulting data coding. Coded data was examined to identify themes and selected reflective quotes for each that best reflected the meaning of each theme. Data were analyzed and reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Results
A total of 15 healthcare professionals were considered for in-depth interviews. Participants worked in varied settings such as academic hospitals, rehabilitation services, and tertiary care hospitals. One participant worked as a palliative care specialist in a hospice center in the community (Table 1). The mean years of work experience for the participants was 7.5 ± 3.26 (range 5–15 years). 14 Participants reported seeing an average of 30.8 ± 14.8 people with PD per month (range 16–50), excluding one participant who sees mostly the same patients in hospice every day. The setting in which NPC was delivered was dependent on the awareness among the professionals to manage the patient on the principles of palliative care and the willingness to refer the patient to allied healthcare professionals for supportive care. Some professionals had the opportunity to avail themselves of such services embedded in the tertiary care center where speech, occupational, and psychological therapies were delivered. However, these services were sought only through referrals made by clinicians rather than functioning within a single team to deliver all services.
Thematic analysis of the data revealed 5 main themes and 20 subthemes, and more than 200 codes were generated. Table 2 shows the interview questions used together with information from the experts. Table 3 shows the major themes and subthemes that emerged from the analysis. Excerpts from the interview transcription that exemplify these themes are outlined in the section below. Appendix 1 in the Supplemental File provides a detailed description of each theme with corresponding subthemes or categories and codes with the relevant excerpts from the verbatim of the experts.
Themes and subthemes.

NPC, neuropalliative care; PC, palliative care; PD, Parkinson’s disease.
A detailed description of themes, subthemes, and excerpts follows.
Theme 1: Understanding NPC
To understand NPC, it is important to reflect on how palliative care was viewed earlier, the evolution of NPC, and the current understanding of the NPC by healthcare professionals.
Subtheme 1.1: Earlier perception
Most professionals held the view that the earlier perception of PC was only about cancer and end-of-life concerns. All professionals viewed the nature of neurological illnesses as very different from cancer, and hence palliative care needs may be looked at differently. They recognized caregiver burden as more in neurological illnesses since the trajectory of the illness is progressively deteriorating. Some professionals held the view that in neurological illness, the focus of palliation was on neurorehabilitation services only and caring for individuals at the advanced disease level.
Previously we had the belief that palliative care is restricted to oncological illnesses, basically to the end-of-life care of cancer patients.—Neurologist Treatment is not time-limited like cancer. There is no start and end to the treatment in neurological disorders.—Neuropsychologist
Subtheme 1.2: Current understanding and practice
Most clinicians opined that NPC is an emerging concept in India, an ever-expanding field that deals with noninvasive, supportive care to improve the QOL. Neurological diseases require more care for longer periods; hence, providing relief from suffering and caring for patients and family members becomes an integral part of NPC. It was opined that the previously held understanding of PC should be redefined, and it must start with conveying the diagnosis to advance care planning so that the dignity of life is protected.
WHO definition has all aspects of care and I think it also includes the interdisciplinary team approach that we should follow in caring for an individual. It must also include the family members as well, so caring for them is also as important as caring for the patient.—OT-Neurorehab So it’s a holistic approach taking care of the family, making life as comfortable as possible with appropriate control of symptoms and giving them dignity of life.—Palliative care specialist
Subtheme 1.3: Objectives of NPC in PD
The main goal of NPC recognized by most professionals was to identify the needs of the patients at every stage of their illness and meet them. Some clinicians emphasize non-pharmacological interventions, which are well-being-focused, not illness-focused. The role of caregivers in the management of PD, pain management for patients, and the importance of advanced care communication skills are also emphasized.
Providing relief than cure, comfort care to lessen the burden. The overall objective is to improve QOL at the terminal stage, delay of deterioration by supportive care, decreased mortality.—Palliative care specialist
Subtheme 1.4: Current practice, referrals, and role of professionals in PD
In the Indian context, NPC relies on referrals to various specialties based on the needs of the patients and the availability of the services. Referrals are made to mental health services in case of burden of caregiving, or when more information is needed about psychosocial management of the illness and family, behavioral problems associated with the illness; to allied health professionals for neurorehabilitation needs and neuropsychologists if disruption of activities of daily living is present. Clinicians recognize the need for NPC, but no such mechanism exists where it is embedded in the current neurological practice. Patients are not looked after by specialized palliative care teams; however, need-based referrals are made to other specialties. Even though it is viewed by neurologists that the current practice is largely pharmacological, there is an awareness regarding the role of other healthcare professionals.
Neurologists refer cases to me to find out the psychosocial needs of the patients. Sometimes they also refer to reduce the caregiver burden and to provide some illness-related information, welfare benefits if there are any, especially in case of poor patients or disability-related.—PSW Patients are usually referred for diagnosis and management but in the current scenario particular referral for palliative care is not there largely because the concept of palliative care is still not inculcated in neurological practice.—Neurologist
Subtheme 1.5: When does PC start in PD?
There is an uncertainty around when must PC start in case of PD. While most of the clinicians believed it must start at the inception of the diagnosis and recognized it as different from end-of-life care, some were of the view that it can start at any point in time during treatment, at mid-stage of PD-4th-5th stage, at last stages of PD—more advanced stage or when higher order interventions such as surgeries fail. A few viewed it as an integral part of the treatment, starting from the diagnosis to end-of-life care.
Subtheme 1.6: Prerequisites of NPC in PD
For Neuropalliative to function as a full-fledged care approach in PD certain prerequisites are identified such as a sensitization for primary care professionals, a dedicated specialists’ team, training, specialized care for non-neurological functions by incorporating various modalities of care, residential palliative care set up, timely needs assessment, changes in a home environment, regular physical therapy, physiotherapy, occupational therapy, and PD-specific nutrition.
Theme 2: Needs of patients and caregivers
Subtheme 2.1: Needs of patients
The needs are defined mostly in the domain of physical, emotional, and spiritual. As the disease progresses, patients have evolving physical needs—they need support for Activities of Daily Living. There are psychosocial needs—psychological and spiritual counseling, tailored nutrition, relaxation, and social participation. Pain management is a huge need of the patients recognized by the professionals. Especially in the face of cognitive decline when a patient is unable to vocalize the pain.
Apart from the physical pain we as professionals need to explore, the emotional pain of what life used to be for the patient and the spiritual needs that are important to build resilience.—Clinical psychologist Non-motor symptoms constitute an important part of the disease. Patients suffer from pain, fatigue, mood changes, stress, anxiety, and depression impacting the patients and caregivers too. The need for psychological intervention and addressing family care needs is important.—PSW
Subtheme 2.2: Needs of caregivers
The caregiver’s needs vary depending on the family milieu and nature of the illness, but largely they have emotional needs and require social and spiritual support needs. The participants discussed the need for effective communication with physicians in the form of conveying prognosis, empathy, and respite from caregiving. Most talked about preparedness for handling illness and training for home management. One professional highlighted the need for grief counseling and bereavement services.
Seeing someone deteriorating in front of their eyes is tough. Supportive psychotherapy sessions are needed for the caregivers even after patients are gone. The emotional needs to be catered to right from the beginning.—Clinical psychologist Psychoeducation is the foremost need since most of the caregivers come with hope and options like DBS is offered only to a few, in most cases counseling helps to reduce the burden of care & reduce the burnout.—Palliative care nurse
Theme 3: Barriers and challenges
Most professionals are of the view that the doctor-patient ratio is poor and physicians have a pharmacological orientation largely; hence, awareness regarding psychosocial interventions is low. Interventions such as supportive psychotherapy and rehabilitation are also limited. Lack of privacy to ventilate the emotional concerns in tertiary care setups with a huge burden of care, lack of residential services for palliative care, high treatment cost, poor accessibility, and lack of government policies or insurance provisions were perceived as barriers. Some of the challenges that were voiced are delayed help-seeking on the part of individuals due to poor awareness of illness. Caregivers’ burden is seen as a challenge since adaptation to illness at home is a difficult task. Specialist care is not accessible to all; hence, even though physicians may feel the need to refer to other allied healthcare professionals, the services are not easily available.
Lack of awareness about palliative care, lack of training as to what needs to be catered to and when is unclear.—Neurologist The cost of the treatment and the accessibility is the biggest barrier. Because of the affordability issues many times the patients only want to spend on the necessary medications than other specialized care.—Neurologist
Theme 4: Interventions for patients and caregivers
Subtheme 4.1: Intervention for patients
Apart from pharmacotherapy, the professionals advocated for psychosocial interventions such as bio-psycho-social strategies for pain management, movement therapies, expressive art therapies, and support groups to provide complete care along with intervention strategies that inform modifications in a home environment and diet modification. Social workers practice art therapy predominantly to help with tremors and musical instruments such as djembe for stress reduction. Neuropsychologist uses cognitive stimulation, activity scheduling, and movement-related therapies in practice.
One of the therapies I propose is dance movement therapy which brings change in the psychological well-being of persons with PD. I do suggest my clients to move around even if in a wheelchair, let them hear some music and make some movements to improve their efficiency level, physical, psychological social as well as emotional functioning.—PSW Regular physical exercise, and occupational therapy linked to their routine tasks can go a long way.—OT Rehabilitation is a huge part which also includes behavioral therapies, inculcating alternative therapies for pain reduction.—Neurologist
Subtheme 4.2: Intervention for caregivers
Caregiver burden can be reduced with the use of self-care strategies, stress management, spirituality, preparedness to handle the ups and downs of illness, psychoeducation, and support groups. Context-driven support for caregivers was highlighted since patients and families from poor socioeconomic status may have different needs.
The interventions that we must provide to the patients as well as caregivers should be focused on the well-being not the illness paradigm Support group in the community as well as in the hospital setting to enhance their well-being.—PSW Assessing the caregivers’ burden from time to time, facilitating relaxation techniques like JPMR, yoga, meditation or referral to a mental health professional to deal with the burden is recommended.—OT
Subtheme 4.3: Specialized care for PD patients
The need for a specialized team with a multidimensional approach was emphasized, along with the need for specialized training resonating with the principles of palliative care. Starting from providing specific education and communication skills to healthcare professionals. Addressing evolving needs of patients and caregivers, accessible rehabilitation services. The concept of a one-stop center provides all care at a nominal cost; other domains of health care need to be incorporated into the treatment regime, which could include DBS, telephonic calls, and specialized nursing care training focusing on the specific needs of PD. There must be a care plan where the patient is reached out to by the medical team in the form of home visits or telecheck-ins.
Theme 5: Facilitators of NPC for PD
Subtheme 5.1: Facilitators
Training and education of all stakeholders, shifting attitudes of primary care physicians, and strengthening the referral care pathways were identified as enablers of NPC. Feedback from beneficiaries, tele-counseling support, the role of NGOs, and palliative care associations were also highlighted. On a policy level, context-driven guidelines, funding, advocacy, and research to enhance NPC emerged as the focal areas.
Some people from remote villages who lack access to healthcare could be linked with govt. programs for financial assistance facilitated by social workers or support groups for PD people at primary level clinics locally.—PSW Palliative care associations for neurological disorders which facilitate 3-6 months courses which undertake training and capacity building of professionals.—Neurologist A tertiary care hospital may be receiving a large number of referrals hence a palliative care unit can facilitate a better quality of care linked to home services.—OT Neurorehab
Discussion
The study delved into the experiences and viewpoints of healthcare professionals working in PD to propose a roadmap for understanding NPC for persons with PD in India. The use of qualitative, exploratory, inductive research design with in-depth interviews involving healthcare professionals from various disciplines with more than 5 years of experience facilitated a deep understanding of the subject matter. Despite growing evidence supporting the need for palliative care in neurodegenerative diseases such as PD, NPC remains largely unfamiliar to many healthcare professionals, including neurologists worldwide. This lack of awareness and acknowledgment significantly hinders the effective management of PD. 9 To add to this, the gap between the services and needs is huge in the Indian context due to the burden of care. 10 Current findings revealed the intention of palliative care in neurological illnesses where the focus is on improving the patient’s QOL, caring for the caregiver, and advance care planning, involving multidisciplinary teams for overall supportive care. However, the view regarding the time points when palliative care must start varies, probably due to the previously held concept that end-of-life care equals palliative care debate. This corroborates with findings from previous literature where participants differed in their views about when and how NPC is needed.11 –14 This clearly emphasizes the need for education for primary physicians/neurologists in palliative care aspects integral to the primary treatment of the illness. Previous literature suggests that healthcare workers must push themselves to have these discussions and should be open to cues from the person with PD for the right time to have these discussions. 15 Extending this knowledge, the role of allied health professionals such as clinical psychologists, social workers, occupational therapists, speech therapists, neuropsychologists, and caregivers are important stakeholders in the management of PD in our study. Existing research has supported this and recognized their role as paramount—right from diagnosis to end-of-life care through the provision of supportive interventions, and there is evidence of the efficacy of such interventions in PD.16,17
What constitutes NPC, according to study participants, is a broad horizon covering psychological (grief and bereavement counseling), social, spiritual, and physical (pain reduction) components. Literature highlights the positive impact of occupational, physio, and speech and language therapies on improving the QOL and maintaining independence for individuals with PD. 18 Although in our study, participants recognized multidisciplinary teams have a holistic remit, the barriers need to be recognized and cleared. The study revealed that currently, the practice is largely based on a referral system, which is dependent on many factors such as primary care professionals recognizing the need, availability of professionals such as psychologists, social workers, and occupational therapists, and accessibility and affordability for the patients and families. Each time the patient is being recommended or referred to for such services the onus of seeking out these services is on the patient rather than a system that is built as a form of palliative care centers or services. Healthcare professionals are unsure of the appropriateness of referral due to a lack of education about palliative care and patients and carers were not equipped with information to seek palliative care. 19 These challenges are not limited to lack of awareness or willingness to refer on the part of the primary treating team but extend to the delivering adequate allied health care, including insufficient expertise among therapists, low patient volumes, and lack of collaboration and communication among different disciplines identified previously. 20 Furthermore, the provision of rehabilitation care by allied health professionals in the palliative stage of PD is hindered by personal and organizational barriers, negative perceptions, and a lack of training. 21 In our study, the need for training, education opportunities, and capacity building for primary and allied healthcare professionals was a prominent theme. There is a dearth of mental healthcare professionals in India, and palliative care training opportunities are also limited. The need to improve the knowledge about complex PD, developing disease management programs, continuity of information, and optimization of coordinated and person-centered care has been documented in earlier studies too.15,22
It has been established that caregivers are important cogs in the wheel for delivering NPC but their burden of care needs a systematic approach.11 –14 In this study, all participants highlighted the role of preparedness on the part of caregivers and the importance of addressing their psychological and spiritual needs since caregiving causes exhaustion and burnout.
Costs of treating PD in India are lower than those in developed nations but are still out of reach for most Indian patients. 23 To meet this challenge, a key finding from the study was the suggestion of the use of tele-support by allied healthcare professionals to enhance accessibility and usability as it is cost-effective and reduces the burden of bringing the patient on frequent follow-ups.
Western literature suggests that a more effective interface between different specialists, more research to determine trigger points when palliative care input is needed, as well as better coordination of health systems is needed in specialist palliative care. 24 A systematic practice review from Europe opined that education about palliative care and movement disorders is essential. Palliative care should be multidisciplinary, individualized, and coordinated. Proactive involvement and support of caregivers throughout the illness is recommended. 14 Authors recommend several pathways for enhancing NPC in India based on the current findings and learning from Western models. Central to the advancement of NPC in India is the commencement of proactive discourse concerning end-of-life care and preferences, initiated early in the trajectory of the ailment. On a broader scale, endeavors should be made to effect policy-level alterations with a special focus on neurological illnesses that must be done to the already existing guidelines for palliative care. 25 This should be accompanied by the establishment of specialized NPC centers equipped with an adequate inventory of symptom-alleviating medications and appropriate infrastructure, thereby providing the requisite impetus for the maturation of NPC services across India. It is imperative to underscore the adoption of a multidimensional approach that centers on holistic patient care and necessitates the collaborative engagement of a diverse cadre of healthcare professionals, encompassing neurologists, primary care physicians, physical medicine and rehabilitation specialists, social workers, psychologists, nursing staff, support personnel, paramedics, pharmacists, physiotherapists, and volunteers—all of whom play pivotal roles in the provision of comprehensive care to patients and their families. Although the complexities posed in the development of NPC are like those in the West, in the Indian context, the landscape is still evolving, and it is in a nascent stage. Personal preferences of the patients and caregivers, coordinated efforts of all healthcare professionals, and continuity of care are needed to advance the NPC in the Indian context.
Despite the study’s considerable significance for the advancement of NPC within the Indian context, it is imperative to duly recognize certain inherent limitations. The endeavor to strike a balance between achieving thematic data saturation and ensuring the practical feasibility of the study engendered the selection of a sample size of 15, a factor that could potentially curtail the extent to which the findings can be extrapolated to the broader population. In addition, it is vital to acknowledge that the qualitative nature of the investigation renders the findings susceptible to the influence of the researchers’ subjective interpretations and perspectives.
Conclusion
Neurodegenerative disorders remain a group of diseases with limited chances of recovery. The illness and its disability progressively increase with periodic crises. This study highlights the psychosocial needs of caregivers and patients as perceived by healthcare professionals and the need for providing NPC services in PD with an integrated approach embedded in the current practice. NPC outcomes need to be considered as part of normative care and not only when dysfunction is suspected. By providing holistic care, the burden of care is reduced, and QOL is improved. Individual attitudinal shifts in care to policy-driven guidelines are indicated for NPC in PD. To provide the structured stepped-care approach in managing PD, there is a need to understand the psychosocial and palliative care aspects of PD in patients and caregivers in the Indian context. Adequate training and resource allocation are needed for NPC to be adopted in clinical care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251326952 – Supplemental material for Neuropalliative care for Parkinson’s disease in India: a qualitative exploration of healthcare professionals’ perspectives
Supplemental material, sj-docx-1-pcr-10.1177_26323524251326952 for Neuropalliative care for Parkinson’s disease in India: a qualitative exploration of healthcare professionals’ perspectives by Prerna Sharma, Upasana Baruah, Suman Kushwaha, Akanksha Yadav and Rajinder K. Dhamija in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.