
Abstract
Background:
It is crucial that clinicians develop skillful communication to support patients to improve their illness understanding. A strong understanding of illness is associated with improved quality of life and care that is consistent with patient priorities. Unfortunately, many clinicians lack these skills, and residents, in particular, feel unprepared. The ABCs (All Providers, Better Communication Skills) is a virtual curriculum that teaches core communication skills to facilitate conversations with people who are living with serious illnesses.
Objectives:
We explored whether the ABCs curriculum increases self-efficacy and addresses self-reported weaknesses in communication training for internal medicine (IM) and family medicine (FM) residents.
Design:
We conducted a prospective sequential mixed methods cohort study.
Methods:
Residents completed pre-/post-curriculum self-assessment surveys and a post-curriculum semi-structured interview. Primary outcomes were changes in self-efficacy, whether the curriculum addressed self-identified training needs and feedback on its structure and delivery. Secondary outcomes included feedback on how the modules could be tailored to IM and FM-specific content.
Results:
Twelve residents completed the study. Most were in IM, female, and aged 26–30 years. Self-efficacy improved significantly as per the SE-12 summative score (mean difference 11.5 points (SD 10.35), p = 0.003). The study-created items showed a significant improvement in breaking bad news (0.83 (SD 0.84), p = 0.005), overall knowledge (0.67 (SD 0.65), p = 0.005), and confidence (0.67 (SD 0.50), p = 0.001). Key strengths of the curriculum were its structured approach, focus on allowing for silence, transferrable skills, and practical application. The virtual format was both a strength and a weakness, as residents appreciated its accessibility but valued real-time practice.
Conclusion:
The ABCs improved self-efficacy among IM and FM residents. We will use results from this study to inform future iterations of the platform that are tailored to resident-specific learning needs and improving patient-centered outcomes.
Keywords
Introduction
Good illness understanding among patients with serious illnesses is associated with receiving care that improves the quality of life1 –3 and aligns with their priorities. 4 Patients with advanced cancer who have a better understanding of their illness are less likely to pursue interventions that are not medically beneficial at the end of life 3 and more likely to decide to focus their care on comfort.1,2 Unfortunately, many patients have a limited understanding of their illness trajectory.1,3,5 –9 In one study where advanced cancer patients estimated life expectancy, 87% overestimated with nearly half (46%) overestimating by more than 2 years. 1
Effective clinician-patient communication is essential to learn what a patient understands and what is important to them. This can help them prepare for illness progression and make informed decisions. Conversations about serious illness encompass a wide variety of subjects (e.g., breaking bad news, code status discussions, advance care planning, and decision-making), and communication throughout a patient’s illness trajectory promotes quality of life. It is important that clinicians can competently facilitate these conversations. Unfortunately, many clinicians have not received appropriate communication skills training,10 –12 and residents, in particular, feel unprepared.13,14
Communication skills can be formally taught and learned,15 –21 and medical residency programs expect that residents are competent in these areas. 22 Unfortunately, family medicine (FM) 23 and internal medicine (IM)24,25 residents report a lack of formal serious illness communication training during their training.24,25 This is in part because communication training is resource- and time-consuming (e.g., in-person workshops) and difficult to standardize across programs. 17 Existing training courses are limited by high cost and the requirement for trained facilitators and can be limited in scope (i.e., focus on specific conversation types, like code status). There is a need for an accessible and standardizable communication training program that prepares residents for the variety of serious illness discussions they will face in clinical practice. Further, the COVID-19 pandemic has forced trainees and clinicians to transition care and learning to virtual formats.26 –31 An online training curriculum could teach residents a broad range of difficult communication skills in a virtual context.
A group of clinicians and researchers at the University of Toronto and McMaster University have developed the ABCs (All Providers, Better Communication Skills), a virtual curriculum that teaches the core communication skills needed to facilitate a wide range of conversations about serious illness. The curriculum includes modules hosted on an Electronic Learning Management System (ELMS) comprised of educational text, video examples, case studies, and short quizzes for self-directed learning. Currently, the ELMS focuses on oncology. In the future, we aim to expand the curriculum to include other disease areas.
Objectives
We aimed to explore whether the ABCs curriculum increases self-efficacy and addresses self-reported weaknesses in communication training for IM and FM residents at McMaster University completing an oncology rotation.
Methods
Study structure
This is a prospective pilot, mixed methods study with quantitative and qualitative measures assessing an educational intervention involving a novel virtual communication skills curriculum using pre-/post-curriculum self-assessment surveys and post-curriculum semi-structured interviews.
Participants
We recruited 12 residents for this pilot study. This sample size was felt to be feasible and has been shown previously to be sufficient for a qualitative analysis. 32 We recognized that this number would underpower our quantitative analysis; however, it was felt to be both appropriate for a pilot study and feasible to recruit in a timely manner. Residents included IM and FM residents completing an oncology rotation at McMaster University. Inclusion criteria were enrollment in the IM or FM programs at McMaster (post-graduate year (PGY) 1–3); enrollment in an oncology rotation; and ability to complete the study in English (Supplemental Table 1).
We used a consecutive sampling method to recruit from a group of FM and IM residents rotating through oncology. These training programs were chosen because serious illness communication skills are a core competency in these disciplines. Further, the ABCs modules are currently oncology-focused, and trainees from both disciplines will care for cancer patients in their future careers—either through their general practice or through medical oncology subspecialty training for IM residents or general practitioner of oncology training for FM residents. We, therefore, felt that the ABCs curriculum would be appropriate to be tested among this group of learners.
All residents completing the rotation had access to the curriculum. Notably, this curriculum was offered in addition to the residents’ training and did not replace a preexisting curriculum. Residents who were interested in participating signed written informed consent (Hamilton Integrated Research Ethics Board (HIREB) 15075). Dedicated time was set aside in the residents’ schedules to allow them to complete the modules. A $50 gift card incentive was given to each resident for their time.
Intervention
The ABCs curriculum was developed to teach communication skills to support healthcare providers leading “difficult conversations” with patients and families with serious illnesses, including specific examples for oncology. The curriculum draws from the strengths of several existing serious illness communication frameworks and teaches a broad range of skills, such as how to explore illness understanding, provide information, and explore values and goals. The curriculum is organized around common structural elements of conversations about serious illness. It is based on the principles that conversations about serious illness are relational, complex, and iterative, and offers a set of skills that can be used in different combinations and at various points of a conversation, instead of a script-like checklist intervention.
The ABCs was created by an interdisciplinary team of clinicians with over 20 years of experience providing care to patients with serious illnesses, including during critical illness and end of life, as well as researchers and educators. The content was developed from a modified Delphi consensus process and was informed by the creators’ experience, literature review, best practices in clinician-patient communication, and expert consultation for content validation. It was refined through a stakeholder panel, including clinicians and educators across Canadian institutions from oncology and palliative care specialties and psychosocial oncology, patients, and family advisors. The final content was defined through stakeholder consensus. 33
The curriculum and content are based on previous online modules uniquely developed by the authors in 2014. These modules were updated for the ABCs curriculum.
The ABCs course begins with a novel framework called “Prepare or Decide,” which helps clinicians understand the overall purpose and outcomes of conversations. 39 The course teaches several principles of communication, such as self-awareness, complexity, and the importance of open exploration. The content then shifts to three sets of micro-skills to support effective, compassionate, and empathic communication. These microskills are building blocks that can be used for any encounter. Knowledge and skills gained from the ABCs apply to all conversations in health care, in all care settings, from the most routine to the most complex. The ABCs are appropriate for all healthcare workers across all health disciplines (such as physiotherapists, nurses, personal support workers, and occupational therapists).
We provide references within the ABCs to the many other communication courses so that learners can take other complementary courses to continue building their skills.
The educational materials were hosted on Moodle ELMS. An overview of the curriculum can be found in Table 1. The curriculum includes six 30-min virtual modules comprised of video cases, educational text, and short quizzes. The modules cover the topics of (i) introduction to conversations about serious illness, (ii) preparing for and introducing a conversation, (iii) assessing understanding, (iv) providing information, (v) responding to emotion, and (vi) summarizing and recommending a plan. Within each module, there were microskills—simple and actionable techniques to show residents how they can apply communication best practices. Residents completed a pre- and post-curriculum online survey (via Moodle) and a post-curriculum virtual semi-structured interview.
Table of contents of the ABCs curriculum.

ABC, All providers, Better Communication Skill.
Outcome measures
Primary outcomes were changes in self-efficacy, whether the curriculum addressed self-identified training needs and feedback on its structure and delivery. We adapted the Self-Efficacy Questionnaire (SE-12) 34 to measure the clinical communication skills of healthcare professionals. The SE-12 has been validated and widely used in different care settings with multidisciplinary healthcare providers. This questionnaire has demonstrated high internal consistency (Cronbach’s α = 0.95) and response stability in test-retest reliability (intraclass correlation agreement of 0.71).
Secondary outcomes included feedback via qualitative interviews, conducted over Zoom, on how the modules could be tailored to IM and FM-specific content. In the interviews, participants were encouraged to elaborate on survey responses, the strengths and weaknesses of the curriculum, and opportunities to adapt it to other specialties.
Data collection and analysis
Data was collected from February 2023 to January 2024. Residents completed online surveys on Moodle prior to and upon completing the intervention. In-depth interviews with all residents were conducted on the Zoom video conferencing platform, and the audio recordings were transcribed verbatim using the Otter.ai text transcription application (Supplemental Figure 1).
Pre-curriculum surveys collected resident demographic data and quantitative assessments of the level of knowledge and confidence in conducting conversations about serious illness with cancer patients. They also collected perceived gaps in existing training and personal learning objectives through open-text questions. Post-curriculum surveys collected updated self-assessments, open-text feedback on the structure of the platform, whether the curriculum met identified weaknesses, and recommendations to tailor the training to IM and FM-level learning.
The results of the survey directly informed the semi-structured virtual interview, to ensure that insights found in the surveys were thoroughly explored. The themes that emerged from the open-text questions were explored in more detail. The interviews also explored the residents’ immediate reactions to the curriculum, its strengths and weaknesses, and which aspects were the most effective at improving self-efficacy (Supplemental Figure 1).
Standard descriptive statistics (frequencies, mean, median, standard deviation, etc.) were calculated for the outcomes and participant characteristics. IBM SPSS version 29 was used for quantitative analysis. We also applied qualitative methods to analyze the survey data, including a qualitative descriptive design in which qualitative data are used to expand upon quantitative findings. We used a constant comparative approach for thematic analysis of the survey’s open-ended questions and the interview transcripts to develop a conceptual understanding of the residents’ perceptions of conversations about serious illness and the ELMS.35,36
While acknowledging that in a reflexivist approach, it is expected that different researchers may bring out somewhat different results, it is important to balance the role of the researcher’s own perspective with results that are grounded in the data. To address this, we reflect on how our perspective influences the data and address this in the final reporting of outcomes. For example, the research team consists of clinicians and researchers with a longstanding interest in serious illness conversations in oncology, which may bias us toward certain views of communication best practices. The primary author, M.S.U., is currently a medical resident, which may influence her views on medical education and teaching communication skills.
Additional steps were taken to ensure the trustworthiness of the study, paying particular attention to credibility and dependability. Researchers develop credibility by engaging with participants over extended periods, observing persistently and reflexively. To support this, the interviews ran for as long as the participant required to express their thoughts. Dependability pertains to the enduring nature of the research findings over time. We have clearly documented our approach for data collection and analysis and our decision-making through the research process to allow others to reproduce the study.
For consistency with the SE-12 validation study, we analyzed the mean summary scores of the SE-12 self-efficacy responses. These were on a 10-point scale from 1 (very uncertain) to 10 (very certain). We analyzed additional survey questions (confidence breaking bad news, discussing goals of care (GOC), transitioning away from treatment and code status; and levels of skill, knowledge, and confidence) as individual items. Responses were compared using a paired T test. Inferential analyses were two-sided, and statistical significance was set at the α = 0.05 level.
Transcripts from the virtual interviews were coded using Lumivero NVivo software version 14. Codes were grouped into categories and categories into themes. The first three transcripts were coded by three authors independently (MS, DB, SJK) who are experienced qualitative researchers. Codes were compared and consolidated among the three analysts, who then developed a master list of codes to guide the analysis of the remaining transcripts. One author coded the remaining nine transcripts (M.S.U.), with the resulting codes and themes discussed and ratified among the analysts. The results of the open-ended survey questions were pooled with the post-curriculum interview to inform the qualitative analysis of the impact of the curriculum on self-efficacy and training needs.
Given that this is a mixed methods study with a substantial qualitative data component, we followed both the Good Reporting of A Mixed Methods Study (GRAMMS) checklist 37 (Supplemental Figure 2) and the Standards for Reporting Qualitative Research (SRQR) statement 38 guidelines (Supplemental Figure 3).
Results
Participants
Twenty-two learners were approached about the study. The demographics of the 12 residents who completed the study, including modules, pre-/post-curriculum surveys, and the post-curriculum interview, are shown in Table 2. One resident who was enrolled was lost to follow-up due to scheduling conflicts and, therefore, not included in our analysis. Most of the residents were enrolled in the IM program, in their first year of post-graduate training, female, and aged 26–30 years (median 28.5, range 24–37).
Resident demographics, n = 12.

PGY, post-graduate year.
Survey results
The curriculum’s impact on resident self-efficacy
Overall, the residents’ self-efficacy, as reported on the SE-12 survey items, significantly improved after completing the curriculum, compared to their baseline scores (p = 0.003; see Table 3 for paired comparisons). Notably, SE-12 summative scores improved by a mean difference of 11.5 points out of a total of 120 points (SD 10.35, p = 0.003). The greatest reported improvements by SE-12 item were in the abilities to successfully encourage patients to expand on their problems, structure the conversation, and close the conversation by assuring that patients’ questions have been answered (mean improvement 1.30–1.50 on a 5-point scale). For a complete breakdown of each SE-12 questionnaire item, see Supplemental Table 2.
Mean self-efficacy scores from the pre- and post-curriculum surveys and paired mean, n = 12.
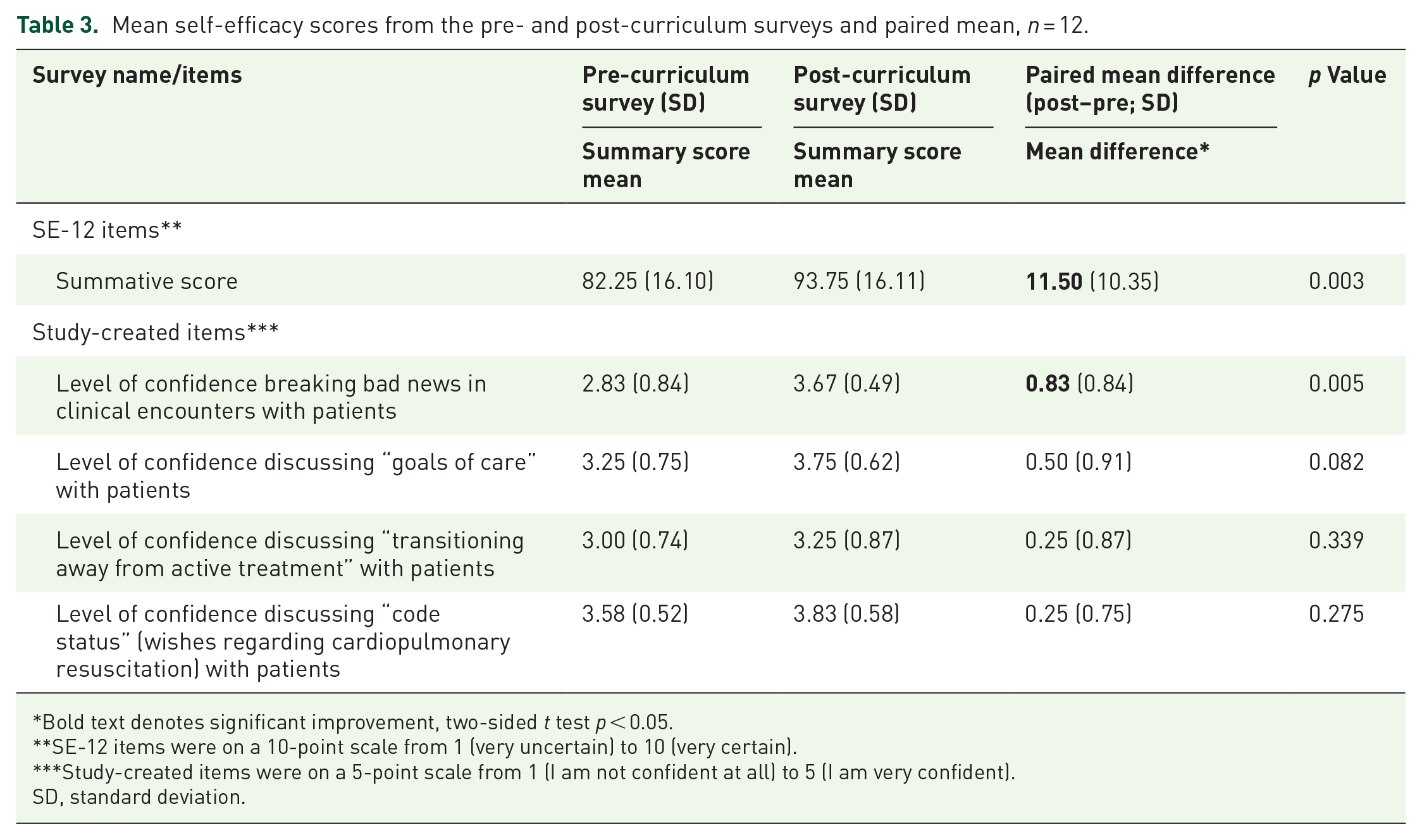
Bold text denotes significant improvement, two-sided t test p < 0.05.
SE-12 items were on a 10-point scale from 1 (very uncertain) to 10 (very certain).
Study-created items were on a 5-point scale from 1 (I am not confident at all) to 5 (I am very confident).
SD, standard deviation.
Similar improvements were seen for the study-created items. Residents reported an increase in their self-efficacy for all items after completing the curriculum, including a significant improvement in their level of confidence in breaking bad news (paired mean difference 0.83 (SD 0.84), p = 0.005); an improvement in discussing GOC (0.50 (SD 0.91)), transitioning away from active treatment (0.25 (SD 0.75)), and discussing code status (0.25 (SD 0.75); Table 3). Their skills, knowledge, and confidence in discussing serious illness improved (Figure 1). There was a significant improvement in their knowledge (mean difference 0.67, SD 0.65, p = 0.005) and confidence (mean difference 0.67, SD 0.50, p = 0.001).

Self-assessment of skills, knowledge, and confidence as reported by residents on the pre- and post-intervention surveys. Assessments were made on a 5-point scale from 1 (none at all) to 5 (a great deal). Improvements in knowledge (paired mean difference 0.67 (SD 0.65), p = 0.005) and confidence (0.67 (SD 0.49), p = 0.001) were significant.
Differences in self-efficacy scores were seen across each training level. Fifty-eight percent 58% (n = 7) of participants were in PGY1, 25% (3) were in PGY2, and 17% (2) were in PGY3. Pre-curriculum self-efficacy scores were higher for more senior residents—94.5 summative scores for PGY3s, 86 for PGY2s, and 83 for PGY1s. Post-curriculum scores, however, were similar across seniority levels (PGY3 post-curriculum summative score was 96.5, PGY2 was 95, and PGY1 was 96).
Learning objectives and satisfaction
The most common pre-curriculum objectives identified in the open-text survey questions were wanting to have a structured approach to conversations about serious illness, transitioning through different parts of the conversation, and balancing information-sharing with emotional support. Key weaknesses in existing training were that communication was felt to be taught as a soft skill, not an evidence-based practice; it focused on a limited scope of conversation types (e.g., solely code status discussions), and there was a lack of supervision.
Most residents indicated that the curriculum met their personal learning needs and prior training gaps. They felt the structured, building block approach would help them facilitate a wide range of conversations and help them navigate the phases of a conversation. The curriculum’s emphasis on allowing for silence and responding to emotion helped them to balance information-sharing with empathy, and the curriculum was felt to be evidence-based and rigorous in its development and execution.
Thematic analysis of the post-curriculum interviews
The post-curriculum interviews took an average of 15 min (range 8–22 min). All 12 participants completed the qualitative interviews. Four key themes emerged: sensibility of curriculum structure and content; realization of prior limitations in residents’ communication skills; benefits and drawbacks of the virtual format; and complement to current knowledge.
Clear and sensible curriculum structure
Almost all residents commented on the structure of the curriculum, which they found to be sensible, clear, and organized. They found the module themes to be intuitive and appreciated the organization of the micro-skills within them, which allowed them to explore the theme with more granularity. This framework helped them to transition to different points throughout the conversation, which was helpful for residents who felt disorganized or patients who got off-track.
I think it would go back to that structure piece; I think it did a really good job of giving me a framework to work with when I have a serious illness conversation. For me personally, that was lacking going in. I knew all the different pieces, but I didn’t always have the best idea of how to piece all the different components together.—PGY2 Family Medicine Resident
The curriculum was viewed as applicable, with practical micro-skills that could be applied in clinical work. Residents appreciated the diverse clinical examples and specific examples of language. They appreciated the focus on identifying unique patient goals and needs. Several residents describe the curriculum as meeting the patients where they are.
All felt that the curriculum, which was primarily oncology-focused, was transferrable to other specialties. They found the concepts of preparing for the conversation, identifying whether a treatment or care decision was needed, determining the patient’s level of understanding, and responding to emotion were particularly transferrable.
I really liked the division between planning conversations and goal related conversations, because that helps you have the agenda set prior to going into the conversation. I think that’s really great and transferable, and then all of the micro-skills are transferable not only in serious illness conversations, but just generally in clinical skills.—PGY1 Internal Medicine Resident
Some barriers to applying the content to other specialties were identified. Illnesses like heart failure or chronic kidney disease were felt to have a longer trajectory than oncology, often spanning decades. Residents felt patients early in their disease may struggle to understand the life-limiting nature of their illness and be unwilling to engage in a conversation about serious illness. Residents felt that the public perception of cancer prepared patients to have these conversations, which was not the case for other diseases. Oncology was viewed as having existing opportunities for these conversations, for example, at diagnosis, after completing a line of treatment, or after surveillance scans. Residents felt there were few natural opportunities for these conversations for other diseases.
Many of the residents appreciated the curriculum’s emphasis on allowing for silence and responding to patient emotions. They found this to be a common pitfall in their own practice and an aspect of the curriculum that was unique compared to prior training. Several highlighted this as a skill they would incorporate into their work in the future.
I think that the parts of it that were the most helpful were. . . the common pitfalls, because those always triggered me to realize that I had fallen into those same pitfalls. Like for example. . . you should recognize when someone is having an emotional reaction and not try to correct them or offer more information.—PGY3 Internal Medicine Resident
Realization of prior limitations in residents’ communication skills
In a few instances, self-efficacy decreased after completing the curriculum. When asked about this in the post-curriculum interview, residents attributed this to the realization that they had misunderstood these skills prior to the training and afterward realized the gaps in their knowledge. They described this as a “pleasant surprise” and felt their new knowledge would help them approach this differently in the future.
I had a couple moments throughout, where I saw things that I could directly tie back to my personal experiences and realize things that I could have been doing differently. Direct specific things that I know I want to take forward into conversations . . . my confidence probably dipped, because having watched all the case studies, I realized that I thought that I was good at it before, but I probably wasn’t leaving enough room in that conversation.—PGY3 Internal Medicine Resident
Benefits and drawbacks of the virtual platform
The virtual format was seen as a strength and a weakness. Virtual access allowed the residents to go at their own pace and fit the ELMS into their busy schedules. The multimedia aspect of the modules was described as engaging.
I also really liked the use of audio-visual media. I thought the videos were really engaging. My favorite part was when we could test our knowledge a bit and the drag and drops I really enjoyed, because I thought that was a chance to see whether or not we’re absorbing the information that’s being presented in the modules.—PGY2 Family Medicine Resident
However, several residents wished there had been a real-time interactive component (either over Zoom or in person), for example, with a standardized patient, where they could practice their new skills.
I think one thing I had written in the post survey was possibly incorporating an in-person session, just to practice this. I don’t know it would be a lot more work to hire standardized patients to practice but even just if there were a couple other residents and we all meet up on the second last day or something and practice these scenarios.—PGY2 Family Medicine Resident
Complement to current knowledge
Some of the residents felt several of the modules were too long, with verbose text and repetitive content, particularly modules 1–3. These modules were also felt by some to be too simplistic, with material that overlapped with prior training. Residents were concerned that this could be a barrier to completion, given busy resident schedules.
. . .it is quite long; it is quite time consuming. I think that this is such an important part of medicine, that it should be given way more time than it is given but from a perspective of getting busy residents to complete online modules, and it’s not being built into the medical school training. . .—PGY1 Family Medicine Resident
Discussion
We found that the ABCs, a novel virtual communication training program, improved self-efficacy among IM and FM residents completing an oncology rotation. Key strengths of the curriculum were its structured approach, focus on allowing for silence and responding to emotion, transferrable skills, and practical application. The virtual format was both a strength and a weakness, as residents appreciated its accessibility but valued real-time practice.
Serious illness communication is an expected competency in medical training in Canada. 39 Residents are required to facilitate a broad range of conversations, spanning the trajectory of disease from diagnosis to the end of life, including breaking bad news, discussions about prognosis, code status, treatment options, and end-of-life care. These conversations must be tailored to individual patient situations, priorities, and information needs. However, residency programs and existing frameworks40,41 are often narrow in scope, focused specifically on one conversation type, and do not encompass the breadth of conversations residents will have in practice. In a review of online medical communication programs, most interventions taught structures for specific scenarios (e.g., breaking bad news) and did not offer transferrable approaches for broader applications. 42 This limits residents’ ability to adjust and adapt their knowledge to individual patients. The residents in our study highly valued the ABCs’ building block structure, which they viewed as transferrable to a wide range of conversation types (e.g., diagnosis vs end-of-life care) and disease areas (e.g., respirology, cardiology).
Communication training has traditionally been through in-person workshops or real-time experience, 43 which is resource intensive and often not standardized. However, online education programs can improve clinicians’ confidence and knowledge and, in some cases, drive behavior change, 42 and clinicians are far more likely to complete educational modules in an online platform than face-to-face. 44 Indeed, members of our research team have shown that virtual training for code status discussions can be equally effective when compared to a live workshop. 45 In a study of a hybrid palliative care education program combining both classroom and web-based content, 46 residents’ knowledge, attitudes, self-perceived comfort levels, and skills improved after completing the program. More recently, members of our team trialed Community Access to PAlliative Care via Interprofessional Teams Intervention (CAPACITI), 47 a virtual program designed to provide advice, strategies, and plans of action to assist primary care teams in operationalizing early palliative care. The virtual format was viewed as an effective element of the program, and although it was offered in combination with facilitated sessions, a purely self-directed format was considered potentially more convenient. As the COVID-19 pandemic forces a transition to virtual training and care, online education will become a growing area of study.
However, the limitations of online platforms are learner isolation and limited support or feedback. 48 Similarly, the residents in our study felt the online, virtual format of the ABCs curriculum was both a strength and a weakness. While the platform allowed residents to work at their own pace, they could not practice their skills or get feedback. To address this, members of our research team are exploring the impact of virtual standardized patient encounters in combination with the ABCs curriculum (trial NCT05810987). If we find the use of standardized patients for training and assessment of communication skills to be feasible, a larger trial will follow.
Understanding and allowing for patient emotions can improve the physician-patient therapeutic relationship.49 –52 Silence is a key emotional tool 53 that can allow patients to process their emotions, reflect, and explore information. 54 Training programs focused on patient emotions can positively impact clinician communication skills, demonstration of empathy, and clinician and patient satisfaction. 55 Communication programs that highlight active listening and allowing for silence are well received by learners. 56 However, there is little formal training in emotional awareness or the use of silence in therapeutic practice, and such pauses in the conversation may feel awkward to the uninitiated.57,58 Indeed, it is often cited that physicians prematurely interrupt their patients, 59 limiting their understanding of patient priorities and ability to communicate useful information. The residents in our study reported that “allowing for silence” and “responding to emotion” were the most profound takeaways from our intervention. They identified these as weaknesses in their prior skills and gaps in existing training programs. This was seen as being practice-changing for many.
Some survey items lacked statistical significance. These included improvements in the participants’ level of confidence discussing “goals of care” with patients, “transitioning away from active treatment” and “code status” (wishes regarding cardiopulmonary resuscitation). Given our small sample size, it is difficult to determine whether this is a true finding. However, if these results were reproduced in a larger study, it would be important to target these areas with an additional focus—for example, by increasing the number of case studies that address these conversations or explicitly addressing difficult aspects of these conversations.
Limitations of this study include its small sample size. Residents were heterogenous in their prior clinical experiences (recruitment spanned PGY 1–3), which may influence baseline knowledge of conversations about serious illness and perception of curriculum difficulty. We found differences in self-efficacy scores across each training level, in which pre-curriculum scores were higher for more senior residents. Post-curriculum scores, however, were similar across seniority levels. This may indicate that senior residents started the curriculum with a higher level of baseline self-confidence due to greater experience with communication skills training programs and clinical work, but the curriculum offered greater benefit to junior (self-efficacy delta of 13 for PGY1) than senior residents (delta of 2). Unfortunately, the small sample size and skew toward PGY1 residents make it difficult to draw conclusions, and statistical significance could not be calculated.
Residents were enrolled in a medical oncology rotation at the time of the study. Communication training is often associated with cancer care, and our residents may have a greater interest in communication skills than the typical IM or FM trainee. We provided the residents with protected time to complete the curriculum, which may not reflect the time constraints of typical trainee schedules.
Self-reported assessments of efficacy may not accurately reflect clinical skills, and our study did not include objective measures of behavior change. Self-assessed performance is generally an inaccurate surrogate marker for competence60,61 and physician confidence and actual ability in end-of-life discussions have shown a large disconnect.62,63 As indicated by our residents, acquiring knowledge of communication skills made them realize their prior shortfalls in engaging in these conversations. However, knowledge may not accurately reflect ability as clinicians may understand what is important in these discussions but lack the skills to carry them out. 64 Further, these measurements are not patient-centered and may not reflect what is actually meaningful to patients.
Future research should investigate if the curriculum improves clinician behaviors directly with a focus on patient-centered outcomes. Unfortunately, there is a paucity of data on this, limiting our understanding of which indicators (e.g., satisfaction with care, understanding of prognosis, or quality of life) are most meaningful to patients. Virtual training programs, in particular, lack this data. 42 Communication training is not benign, and while some interventions improve patient and family satisfaction, 65 others have been associated with worsening patient depressive symptoms, 66 underlying the importance of focusing training on outcomes that benefit patients. In a recent systematic review, members of our research group found a wide diversity in outcomes to measure the effectiveness of palliative care educational programs and limited trials assessing actual behavior change or impact on patient- or family reported outcomes. 67
Conclusion
We found that the ABCs virtual curriculum improved self-efficacy among IM and FM residents on an oncology rotation at McMaster University. Strengths of the curriculum were its structured approach, focus on allowing for silence and responding to emotion, and practical application. The virtual format was a strength and a weakness, as residents appreciated its accessibility but valued real-time practice. We will use results from this study to inform future iterations of the platform that are tailored to resident-specific learning needs and improving patient-centered outcomes. We aim to expand the ABCs ELMS to encompass specialties outside of oncology, including cardiology (e.g., heart failure), respirology (e.g., chronic obstructive pulmonary disease), nephrology (e.g., end-stage kidney disease), and acute care specialties (e.g., critically ill patients and procedural consent). Our overarching aim is to ensure that all residents have the communication skills necessary to effectively facilitate conversations about serious illness with their patients.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251326949 – Supplemental material for A mixed methods pilot study of a serious illness communication training curriculum among medical residents
Supplemental material, sj-docx-1-pcr-10.1177_26323524251326949 for A mixed methods pilot study of a serious illness communication training curriculum among medical residents by Megan Smith-Uffen, Shilpa Jyothi Kumar, Oren Levine, Daryl Bainbridge, Jeff Myers, Leah Steinberg, Nadia Incardona, Maggie Civak and Hsien Seow in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.