
Abstract
Background:
Bereavement support is considered a core standard of care for paediatric palliative care (PPC) teams. Support for grieving siblings can present unique challenges. Developmentally appropriate care can help children navigate their grief experience.
Objectives:
To describe the provider perspectives (mission and development) of bereavement care for siblings, and to describe the bereavement follow-up interventions offered for siblings by hospital-based PPC teams nationwide.
Design and methods:
Qualitative study conducted by semidirected telephone interviews. At least one member from each PPC team was interviewed. Interviews transcribed verbatim were analysed using grounded theory.
Results:
Twenty-one teams participated (response rate 91%). Most teams (80%) provided individual psychotherapy to families, and a few (28%) offered group interventions. PPC teams endeavour to expand their bereavement services and create a stronger collaboration network with community services. However, limited human resources, lack of facilities and financing, and geographical distances were frequent obstacles to bereavement care program development.
Conclusion:
PPC teams support bereaved siblings as an integral part of palliative care. Although PPC teams cannot meet all the needs of bereaved families, they can serve as important reference points to consolidate knowledge of available local resources and offer well-informed guidance to families and community users. Greater public awareness of childhood bereavement and engaging with community structures could help overcome some of the common obstacles to service development. Further studies are warranted in evaluating bereavement services in France and in other healthcare systems.
Introduction
Paediatric palliative care (PPC) is defined as the active total care of children with life-limiting conditions and involves providing support to the whole family after the patient’s death. 1 In France, the annual death rate in paediatric, adolescent and young adult (<24 years) populations represents about 1% of the nation’s total deaths. 2 Similarly, an American study estimated that nearly 1.5% of all children nationwide would be bereaved of a sibling by the age of 18. 3 Despite being a common experience, bereavement can potentially have a negative impact on both short- and long-term psychosomatic and socioeconomic outcomes without suitable support systems. 4 Continuing care beyond the death of a child through family bereavement support is an international core standard of care for PPC teams.5,6
There is growing evidence, predominantly from intensive care and oncology, that transitional hospital-based bereavement care is beneficial for both families and health care staff. 7 For staff, continuity of relationships is an integral part of their own bereavement process, 8 and they view their role as meaningful and gratifying.7,9 For parents, the loss of the hospital community after the death of their child can be abrupt and challenging. Maintaining contact with staff aids in building a new community of supportive peer relationships, which can improve psychosocial outcomes. 7 For siblings, hospital coordinated peer groups are particularly helpful for normalizing their grief experience, reducing isolation and reinvesting their social life.7,9,10 Although continuity of care has historically proven to be beneficial, most hospital-based interventions are geared towards parents. Very few are directly aimed at siblings.7,8 Further information, from the vantage point of PPC professionals, is needed to identify their role in caring for bereaved siblings, methods used and challenges faced.
PPC teams in France were created in 2013 following the governmental plan for the development of palliative care. 11 Twenty-three multi-professional ‘Regional PPC Resource Teams’ (Equipes Régionales Ressources de Soins Palliatifs Pédiatriques) were established to provide PPC care across their allocated geographical territories. Each team is tied to a tertiary care hospital, and functions as an outreach consultation team working alongside colleagues both in the hospital and community setting. No specific in-patient PPC services (such as paediatric hospices) existed at the time of the study. 12 The French organization of PPC is unique in Europe in that the teams are federated on a national level so as to ensure equal access to PPC across the country. 13 These 23 PPC teams were given five missions: (1) cultivate a palliative care approach among paediatric teams, (2) promote awareness of distinct features of PPC teams, (3) provide ongoing support to the family (including bereavement care), (4) train and support healthcare professionals and volunteers and (5) contribute to advancing research. 14 Although bereavement support is a clearly defined mission and a pillar of quality PPC, only one French intervention for bereaved siblings has been described and evaluated to date. 10
Bereavement care is identified as care given to all family members of the deceased child. Sibling bereavement care stems from this concept yet requires a more specialized approach, such as age and developmentally focused services. For this reason, we felt it important to develop a better understanding as to how PPC teams perceive and work towards their goals in bereavement care for siblings. The objective of this study is twofold: to describe the provider perspectives (mission and development) of bereavement care for siblings, and to describe the bereavement follow-up interventions offered for siblings by hospital-based PPC teams nationwide. To our knowledge, this is the first study to survey French bereavement support for siblings on a national scale and to focus on bereavement support given specifically via PPC teams.
Materials and methods
Participants
We conducted a qualitative study of PPC teams across France. All 23 teams were invited by email in January 2021 to participate in the study. Two reminder emails were sent at 2-week intervals. All French PPC teams were eligible for inclusion. Those refusing to participate or not responding to emails were excluded. At least one member from each team was interviewed, preferably the one most involved in their team’s bereavement care interventions. However, we did not request participation from a specific profession nor did we limit the number of members that could participate. As long as the interviewee was currently employed by the team, there were no specific exclusion criteria. All participants provided informed consent to participate in the study. Obtaining theoretical data saturation required a maximal number of included teams in order to provide a complete landscape of French PPC team-based bereavement care for siblings. 15
Procedures
We conducted the semi-structured telephone interviews from February to April 2021. The teams received by email a list of questions 1-month prior to the interview. This allowed time for internal team discussion prior to their appointed spokesperson’s interview. The open-ended questions concerned four topics: definition and evaluation of the mission, current interventions in place, means of collaboration and bereavement care development. All interviews were anonymized (PPC team 1–21), audio-recorded and transcribed verbatim. All interviews were conducted in a private space within the hospital in French by the first author (female hospital physician (MD) with previous experience in qualitative research in palliative care). All participants spoke fluent French and had no hierarchical or established relation with the researcher prior to the study.
Analysis
Quantitative data weres analysed using raw scores and percentages to provide descriptive statistics. Qualitative data was analysed using Glaser and Strauss’s ‘Grounded Theory’. 16 The transcribed interview texts were coded in a three-step process: open coding, axial coding and selective coding. First, the text was open coded ‘line-by-line’ to identify anchors allowing the key points of data to be gathered (such as ‘avoiding abandonment’, ‘emptiness’, ‘keeping contact’, ‘maintaining a connection’, etc.). Next, axial coding involved regrouping the codes into concepts (or collections of codes of similar content) such as ‘reducing isolation’ and ‘continue walking with families’. Lastly, selective coding sought to aggregate broad groups of similar concepts into distinct categories or themes, such as ‘continuing care’, to describe the subject of research (provider perceptions on the mission and development of bereavement care for siblings). The analysis was undertaken by the authors and discussed until consensus was reached. The results are reported in accordance with the consolidated criteria for reporting qualitative research (COREQ; Supplemental File 1). 17
Results
Twenty-one teams were included in our study (91% response rate). One team refused participation (too recently established) and one team was unreachable and were excluded from the study. A total of 30 PPC team members participated in the interviews: 15 psychologists, 9 nurses, 5 doctors (4 paediatricians and 1 child psychiatrist) and 1 secretary. Fourteen interviews were conducted with one team member, five interviews with two members and two interviews with three members simultaneously. Interviews lasted a median time of 27 min (18–76 min). The major themes that emerged from the interviews were grouped into the three categories shown below.
Defining the mission of bereavement care for siblings
From the interviews emerged four subthemes characterizing the mission of bereavement care as provided by PPC teams.
Important and essential work
Three-fourths of the teams (76%, n = 16) viewed their mission of bereavement care as ‘important’ and ‘essential’ work for PPC teams. The main reason given was that other paediatric healthcare professionals rely on their provision of services to ensure befitting follow-up of bereaved families, especially since services are free and PPC staff are experienced in childhood grief. Several PPC teams consider bereavement care to be equal to their other missions, but it must be constantly re-evaluated and re-defined depending on the families’ individual needs and each team’s capacity to respond.
Continuing care
Bereavement care was viewed as a means to continue walking with families, especially siblings and parents, for an extended period. Both PPC teams and families appreciated the continuity. The families were relieved that they need not retell their story and valued speaking with healthcare professionals who knew their loved one. PPC team members reported the importance of keeping in touch with families and ensuring that they received the help they needed to navigate their grief journey. Furthermore, some expressed that maintaining contact can help reduce the feeling of abandonment that many families encounter once medical care stops after death: “It’s an integral part of our work in palliative care. Bereavement care is nothing other than the continuity of care for the deceased child and their family.” “Families can feel a sense of abandonment and total emptiness, there was so much going on around the illness. . . It’s the idea of not leaving behind families that we cared for all throughout the illness, of maintaining a connection.”
Second-line support
Almost half of the interviewees reminded us, however, that their teams alone were unable to provide all the bereavement care needed for siblings in their region. Taking on a resourceful ‘second-in-line’ role can be necessary. This involved onward referral for professional help, collaborating with existing community services, and providing support and training to other ‘frontline’ professionals less experienced in childhood grief: “We are attentive to maintain our ‘resource mission’. By that we mean that we try to be resourceful for parents and siblings, that we’re not necessarily providing ‘front-line’ periodic follow-ups, but that we foster the resources available around a family.”
Anticipating grief
Some teams emphasize that bereavement care should be anticipated. When palliative care commenced, they explained to families that they would continue to journey with them even after the child’s death. Some felt that being able to work with the families before the death occurred could help reduce unfavourable outcomes and could improve the quality of bereavement care: “Working (with the family) while the child is still alive reduces complicated grief. . . It improves care following death.”
Current bereavement care services
Intervention type
Although all teams seek to maintain contact with families, half of the teams (57%, n = 12) had a more systematic method of punctual bereavement follow-up with specific mediums and time-points. Sending a card (52%, n = 11) or a telephone call (57%, n = 12) addressed to the whole family (siblings and parents) were the most frequent means used. These took place at regular intervals between <1 week and 3 years post-death. Some teams always offered a consultation (14%, n = 3) or home visit (19%, n = 4), which siblings were invited to attend. These typically took place between 1 and 5 months after the death. Figure 1 shows the different means of contact and time-points implemented by the PPC teams.

Bereavement follow-up.
The most common form of bereavement intervention by French PPC teams was individual psychotherapy (80%, n = 17) provided by the PPC teams’ psychologists. Sessions took place either at the hospital (n = 9) and/or at the family’s home (n = 15). Reasons for meeting outside of the hospital included providing a neutral location and less restrictive facilities. Most teams did not put a time limit on the duration of therapy (n = 10). One-third of teams (n = 7) placed an upper time limit either at 2–5 punctual meetings (n = 3), 1 year (n = 2) or 2–3 years (n = 2). The reason given for placing a time limit on therapy duration was lack of human resources for the longer term.
Six teams offered group interventions. These interventions took on various forms (group sessions, playgroup, camps) and were led mostly by psychologists accompanied by other professionals. All groups, with the exception of the playgroup, were geared specifically towards children bereaved of a sibling. The layout balanced grief-centred activities with more leisurely and creative activities. In regards to intervention accessibility, families almost exclusively gained referral from the PPC team that knew them previously. Only three teams that offered a group intervention advertised their services and accepted outside participants. Regarding funding, all PPC team members led groups during their work hours and thus were entirely remunerated for their services. Additional expenses were covered by external funds. All groups, including weekend camps, were free of charge for families. A detailed outline of the individual group interventions can be found in Table 1.
Group interventions.
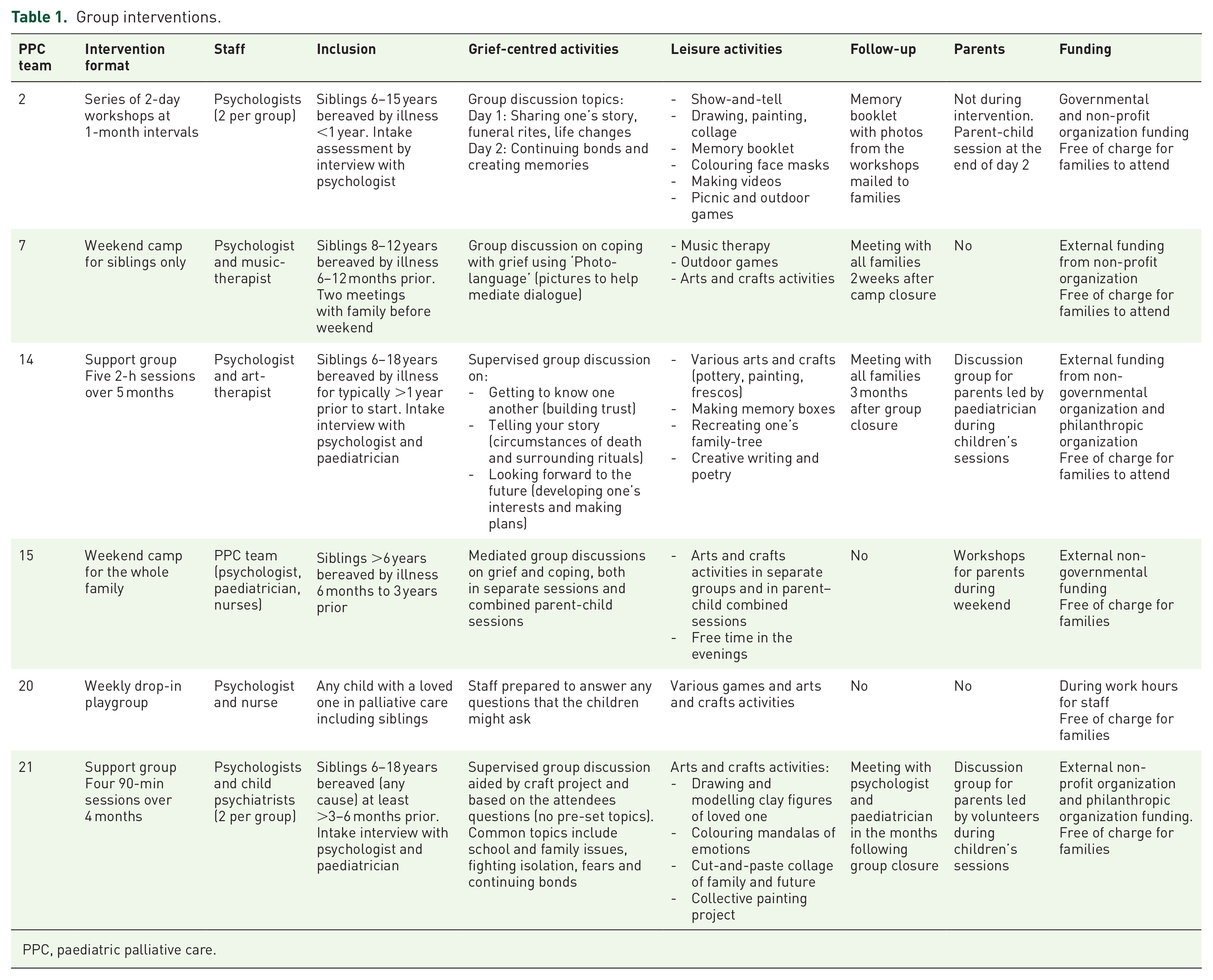
PPC, paediatric palliative care.
Collaboration with community services
All teams collaborated with various community services including non-profit organizations (n = 17, 80%), schools (n = 11, 52%), special schools and institutes for the handicapped (n = 15, 71%) and home hospice care (n = 6, 28%). Collaboration with community services was predominantly an indirect aid to the bereaved siblings by directly aiding the staff that cared for them. PPC teams referred onward to non-profit organizations that provided group interventions, and to seek local care for families further away. One team even founded their own non-profit organization to provide bereavement groups. In schools, teams assisted the teaching staff in talking about death and dying with students, sometimes meeting students directly when necessary. Two teams had been invited to give lectures at school counsellor training days, and one team met with their school board superintendent, school nurses and doctor to better explain their mission and services. Lastly, PPC teams often led debriefing sessions for community workers following death.
Intervention staff
In all teams, the psychologists had a leading role in coordinating and providing team bereavement care services. In most teams (n = 16, 76%), PPC doctors and nurses played a contributing role by following up with families (sending cards, telephone calls). Their medical expertise was particularly useful for post-death home visits and consultations when families needed further medical explanations regarding the child’s care and circumstances of death. Three-fourths of staff members (76%, n = 16) had not received prior training specifically in the area of childhood grief, but rather ‘learned on the job’ (PPC team 3). Five teams had undergone specific training in the grief process in children and facilitating group discussions. Most, however, had some form of training in palliative care in which bereavement is briefly covered.
Two-thirds of teams (66%, n = 14) organized regular debriefings for their team. For most (n = 10) it consisted of one meeting every 2–4 months led by an external psychologist or psychiatrist, but concerned all areas of pediatric palliative care. Four teams (all providing group interventions) had supervision for staff specifically to discuss bereavement care after each intervention session. When asked about emotional exhaustion, less than one-fourth (n = 5, 23%) considered it a limiting factor for past bereavement services provided. Methods to avoid ‘burnout’ include working in pairs and team supervision. Regarding burnout, one team stated ‘just the opposite’, that ‘not being able to provide adequate bereavement care gives the impression of giving sub-optimum care to families’ (PPC team 20) and could be a source of occupational burnout. Providing bereavement care can help PPC teams ‘close the loop’ (PPC team 1).
Development of bereavement care services
When asked if the teams felt that they were meeting the needs of the families in their care, only one-third responded positively (n = 7, 33%). The majority of teams (n = 14, 66%) felt that improvements were needed. Table 2 gives a description of the future vision and barriers to development as described by the teams.
Future vision and common obstacles to bereavement care development for siblings.

PPC, paediatric palliative care.
Future vision
The teams gave three areas where they would like to develop bereavement care for siblings: establish or expand group interventions (n = 11), create a stronger collaboration network with community services (n = 6) and redefine and communicate services (n = 6).
There was a demand from parents and professionals to develop support groups for siblings. Children appreciate the group dynamic and ‘they often say that they are happy to meet other children like themselves’ (PPC team 21). Teams also hoped to extend their services to younger children ‘under six years of age with a low staff to participant ratio’ (PPC team 21).
Developing a strong collaboration with community services was vital, especially for psychologists who were ‘the only psychologist on the team’ (PPC team 10). The PPC teams sought to better equip the community to help them respond to the demand, whether it be teaching ‘other professionals to detect grief’ (PPC team 7) or ‘working with schools [to] help both students and teachers’ respond to grief (PPC team 14).
It was important for teams to keep their mission in-check in order to ‘offer professional and personalised care’ (PPC team 10) and because it ‘requires a team effort to keep it going’ (PPC team 9). Several teams sought to ‘inform other hospital wards and schools’ of their services (PPC team 14), as well as keep an ‘up-to-date repertoire of local groups’ (PPC team 2).
Common obstacles
On the other hand, teams reported three major obstacles to developing bereavement care: insufficient human resources (n = 17), lack of material resources (n = 21) and geographical distance (n = 10).
Lack of time prevented teams from starting ‘any project that was too ambitious’ and making it ‘long-term’ (PPC team 2). Psychologists especially felt that more human resources were necessary ‘to dedicate more time to follow-ups’ (PPC team 14) and to be ‘able to go deeper with families’ (PPC team 13).
Furthermore, lack of material resources further restricted interventions. Funding was ‘hard to obtain’ (PPC team 2) leaving bereavement care projects ‘underdeveloped’ (PPC team 20). Teams often lacked sufficient facility space to welcome families, and some families preferred to meet in a neutral location outside the hospital ward. To overcome these obstacles, several teams offered ‘home visits’ that were ‘more comfortable for families’, sometimes travelling ‘throughout the entire region’ to meet demand (PPC team 6).
However, not all teams were able to offer home visits due to long distances. Some requests for follow-up were turned down ‘because it was too many kilometres to drive’ (PPC team 17). Remote and socially underprivileged regions were particularly challenging, as resources outside the city were scarce and families lacked ‘the means to make the journey for groups happening in the city’ (PPC team 8).
Discussion
Main findings
PPC teams described bereavement support for siblings as being an important continuation of care. Most teams provided individual psychotherapy to families, and a handful of teams offered group interventions. PPC teams hope to expand and communicate their bereavement services, as well as create a stronger collaboration network with community services. However, limited human resources, lack of facilities and financing, and geographical distances were frequent obstacles to bereavement care development.
Implications for current and future practice
Addressing siblings’ concerns and needs throughout their brother/sister’s illness and beyond death is an important aspect of care, as their suffering is often underestimated. Current international standards for PPC recommend that psychosocial support should be ‘available to all family members after the death of a child and, when possible, for as long as needed’. 6 French PPC teams viewed bereavement care coordination as an important aspect of continuing care, and each team had an individual approach to their interventions. Bereavement interventions for siblings can take on various forms (such as group sessions, weekend camps, family therapy and individual therapy), but the most commonly described form in literature are group interventions. 9 Services that balance a mixture of grief-related and leisure activities can be beneficial in facilitating dialogue and creating a sense of community among grieving families. 9 Participating children positively evaluated the group dynamic which helped them to express and normalize grief, reduce isolation and reintegrate socially, increase awareness of self and others, and to simply have fun.9,18 –23 Out of the 21 teams interviewed, less than one-third provided group interventions (n = 6, 28%), but half of PPC teams (n = 11, 52%) viewed establishing peer support groups as an important way forward. Out of all types of interventions reported by the teams, developing group interventions was at the forefront.
Although many French PPC teams perceived the benefit of such groups, their development was often held back by insufficient human resources and funding. Literature often describes that sibling bereavement groups are conducted by unpaid volunteer staff from a variety of backgrounds. 9 Whereas in North America other professionals may be identified as the key facilitator, such as social workers, 8 in France psychologists lead hospital-based bereavement care and are remunerated for their services. It was a governmental choice to employ at least one psychologist in every PPC team to help uphold this mission 24 as supporting bereaved children has its unique challenges. A child’s understanding of death evolves over time with cognitive development and maturity. Five components are progressively acquired: irreversibility (permanency of death), personal mortality (death applied to oneself), universality (all living things must eventually die), non-functionality (cessation of all life-defining capabilities) and causality (realistic understanding of death’s causes). 25 The age at which children have a mature understanding of death is variable in the literature, spanning from 4 to 12 years, although most acquire key bio-scientific components by age 7. 26 Psychologists are a key component for facilitating dialogue in individual or group settings while taking into account the dynamics of a child’s cognitive maturity and growth. This is particularly important for future development of bereavement interventions for young children under the age of 6. Although many children may not require professional assistance nor show signs of complicated grief, developmentally appropriate bereavement care is befitting and helpful for families to navigate the grief experience.27,28
Despite French PPC teams being nationally federated and funded through the public health care system, those that offered group interventions had to seek out external non-governmental funds to support these services. Furthermore, French PPC teams did not report other forms of group interventions, such as annual remembrance ceremonies or memorial services, which are considered to be an integral part of other hospital-based bereavement programs.7,8,29 These ceremonies had a positive impact on grief and families viewed them as one of the most helpful interactions with the program. 29 If financial and human resources are lacking for regular group interventions, developing annual commemorative services could be an alternate and complementary step forward. This underlines the need to continue raising awareness of childhood bereavement as a broader public health concern and to continue advocating for more accessible services.
If the teams were unable to meet the siblings’ needs through their services alone, they reached out to the community for well-suited alternatives. All teams collaborated with bereavement services in the community setting through non-profit organizations (80%, n = 17), the school system (52%, n = 11), special schools and institutes for the handicapped (71%, n = 15), and/or home hospice care providers (28%, n = 6). French PPC teams are organized as outreach consultant teams, each responsible for overseeing care for both in- and outpatients of a designated geographical region sometimes spanning over 100-km. Interviewees were conscious that their teams alone had insufficient time and resources to directly meet all the needs of their bereaved families. Taking on a more indirect, supportive ‘second-line’ role was essential, involving referring onwards, collaborating with existing resources and training others to accompany childhood grief. Providing grief education for the workforce and community can help strengthen the capacity of the whole system to respond adequately and sensitively to the needs of grieving children. 30 Many teams had reached out to teachers, nurses, doctors and superintendents of mainstream and special-needs education schools to assist them in recognizing and supporting grieving students. Enhanced school-based social support from teachers and friends can facilitate the adjustment of bereaved siblings. 31 Furthermore, French PPC teams provide bereavement care almost exclusively to families already under their care prior to death. Many professionals and families may look to PPC teams for advice in onward referral. Having a good knowledge of existing local group interventions offered through non-profit or other community organizations is necessary for appropriate guidance. Bereavement care, albeit important, is a mission among many others for PPC teams. Collaborating with community services to create a network of resources for bereaved families is critical to filling the gaps and meeting the needs of grieving children.
Participating in hospital-based bereavement follow-up has a positive psychosocial impact on both the staff and the families involved. 7 Staff often found meaning, satisfaction and closure in assisting bereaved parents to transition from the hospital to the community.7,8,32 Our study highlights that this is also true for PPC staff in assisting bereaved siblings in their grief. Interestingly, three-fourths of PPC teams (76%, n = 16) did not view bereavement care as a source of emotional exhaustion if proper measures were taken. Rather it was described as befitting and fulfilling for PPC professionals to continue walking with families and to help bring closure. Healthcare professionals can also experience a degree of grief following the death of a paediatric patient. 33 Support from colleagues within the healthcare team and focusing on positive outcomes surrounding the circumstances of a patient’s death were important alleviating factors of grief. On the other hand, lack of organizational support and restrictions on expressions of grief were compounding factors.7,33 Lastly, three-fourths of PPC team members had not received prior training specifically in the area of childhood grief. Lack of knowledge and advanced skills in handling death-related issues can be linked to increased difficulty in providing care, 34 underlining the importance of targeted formation. Additional resources such as age-appropriate literature may further empower health care professionals to guide sensitive conversations. 35 Providing team debriefing and specific training seem to be important foundations for PPC teams in general, and especially in bereavement care.
Study limitations
Our study had some limitations. For most teams, only one member participated in an interview which could lead to a reporting bias. We attempted to minimize this bias by sending out the interview questions in advance so that teams could discuss their responses and requesting that the spokesperson be the one most knowledgeable of their team’s bereavement care. Broad inclusion criteria allowed our study to have a high response rate, thus giving an accurate landscape of current interventions nationwide. Although our study aimed to focus on the mission and provision of bereavement care for siblings, some interviewees may have expanded their answers to include parents and the family as a whole. This could potentially reduce the specificity of our findings, which should thus be interpreted with caution. Second, our study presents a collection bias as interviews took place over telephone and were relatively short. Lastly, the heterogeneous allocation of resources and population distribution of each team’s territory were factors not taken into account in our analysis and could further impact bereavement service provision.
Conclusion
In conclusion, PPC teams value supporting bereaved siblings as an integral part of palliative care, and employ available resources to create a support network around each family. Although PPC teams understandably are unable to meet all the needs of bereaved siblings, they can serve as important reference points to consolidate knowledge of available local resources and offer well-informed guidance to families and community users. A greater public awareness of childhood bereavement and engaging with community organizations could help overcome some of the common obstacles to service development. Further studies evaluating the feasibility and efficacy of services in France, as well as other nationwide studies analyzing their service provision in relation to their pediatric palliative care model, are warranted. PPC teams regularly encounter grieving siblings, and these teams can be instrumental in helping families navigate their bereavement journey.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524241304782 – Supplemental material for A nationwide survey of bereavement care for siblings provided by paediatric palliative care teams
Supplemental material, sj-pdf-1-pcr-10.1177_26323524241304782 for A nationwide survey of bereavement care for siblings provided by paediatric palliative care teams by Ashley Ridley, Régis Aubry and Sandra Frache in Palliative Care and Social Practice
Footnotes
Appendix 1: Guiding interview questions
Acknowledgements
The authors would like to extend their sincere gratitude to the members of the paediatric palliative care teams that participated in this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.