
Abstract
Palliative care is a holistic practice using a multidisciplinary approach in addressing multidimensional needs. Although the social aspects surrounding the end-of-life phase suggest a place for social work in it, the profession is often inadequately involved in daily practice. This contrasts strongly with the potential meaningful contributions of social workers in this field. To date, no comprehensive list of prerequisites for meaningful social work involvement in palliative care exists. This review aims to gain more insight on the prerequisites for meaningful social work involvement in palliative care and how to realise them in practice. It could therefore provide pathways for future intervention development in enhancing the involvement of social workers and maximising their contributions in palliative care. A scoping review methodology was used. A systematic selection of peer-reviewed articles ranged from 2000 to April 2021 – out of the electronic databases Web of Science, Scopus and Pubmed – was conducted. The 170 articles that met the eligibility criteria were analysed for relevant content using open and axial coding processes. The findings are reported according to the PRISMA-ScR checklist. The nine prerequisites listed in this review concern the level of individual social work capacities and the level of contextual factors structuring social work practices. A majority of articles have, however, focused on the level of individual social work capacities in a rather specialist view on palliative care. Future research should further address the contextual level of social work involvement in the broader practice of death, dying and bereavement.
Introduction
Palliative care is an inherently multidisciplinary practice.1,2 Recent definitions describe palliative care as ‘care that helps with personal, social and medical problems associated with serious and potentially mortal illness, assists families and carers and supports them in bereavement, and uses approaches from a trained team, but also involves friends, family members and the wider community’. 3 The complex and multidimensional nature of needs and the multiple care recipients and providers warrant a coordinated and multidisciplinary care approach. Furthermore, the sociological tradition has emphasised that death, dying and bereavement are social processes with medical components rather than the other way around. 4 The social aspects surrounding the end-of-life phase indeed suggest a place for social work in palliative care practice.
From the inception of palliative care in the latter half of the 20th century, social workers have always been involved5–7 and today they can even be described as core members in this field of practice.7,8 Brandsen 9 discerned three major social work roles in palliative care: social workers address psychosocial concerns of clients and their relatives; they promote and contribute to advanced care planning (ACP) and offer grief counselling for bereaved relatives. In performing this role, social workers pay extra attention to vulnerable groups with specific palliative care needs. 10 The theoretical added value associated with these roles lies in the ‘person-in-environment’ perspective, which can be traced back to Mary Richmond’s 11 model of social diagnosis. As social work assessment links individual clients with their physical and social environment, it is ideally suited to respond to various end-of-life challenges and to complement to multidisciplinary palliative care practice.9,12 Furthermore, the empirical added value associated with these roles relates to better outcomes for care recipients and general cost-savings in end-of-life care spending for care institutions. 13
However, social workers often struggle when claiming their role 7 and their capacities often remain underutilised in professional palliative care delivery. 6 At the same time there is a call for optimising underused nonprofessional capacity in palliative care. This is one of the strategies to guarantee the adequate delivery of care in the context of a growing number of people with palliative care needs versus a limited number of professionals explicitly mandated to meet these needs.10,14,15 This strategy creates new opportunities for social work as the profession has the potential to extent professional palliative care delivery beyond formal health care settings to the larger community. 16 In this respect, social work can build bridges between professionals in formal health care settings, dying clients and the persons that matter to them such as informal caregivers and bereaved family members.17,18 Social work is therefore a unique player in palliative care practice as it can make meaningful contributions to both professional and nonprofessional care delivery.
To enhance the involvement of social workers and maximise their contributions in palliative care, the pathways to do so need to be explored and, hence, the prerequisites identified. This is important for the future development of interventions aiming to optimise the capacity of social work in both professional and nonprofessional palliative care delivery. To date, no comprehensive list of prerequisites exists.
The main aim of this study is to gain more insight on the prerequisites for meaningful social work involvement in palliative care. By ‘prerequisite’ we mean a situation that must exist or a condition that must be fulfilled before social workers can be meaningfully involved in palliative care. Logically, many of these prerequisites will relate to unfortunate realities in contemporary social work or palliative care practice that need to be addressed. By ‘meaningful involvement’, we refer to a situation in which the capacities of social workers – their knowledge and skills – are well developed and fully utilised in palliative care delivery. The breadth of this study topic lends to a scoping review approach as this type of review typically starts from a broad and comprehensive but structured and reproducible search strategy. As this scoping review is the first step in gathering relevant information on the prerequisites for meaningful social work involvement in palliative care, it is recommended to approach this topic broadly.
This scoping review specifically addresses the following two research questions:
What are the prerequisites for meaningful social work involvement in palliative care?
How can the prerequisites for meaningful social work involvement in palliative care be realised in practice?
Methods
The structure of this scoping review paper is guided by the Preferred Reporting Items for Systematic reviews and Meta-analyses extension for Scoping Reviews (PRISMA-ScR) by the Joanna Briggs Institute.
Eligibility criteria
The studies that were included in this scoping review had to meet the following eligibility criteria:
Contributions in peer-reviewed journals of which the full text is available and of which the full text is written in English;
Contributions in peer-reviewed journals of which the main focus lies on the involvement of social work in palliative care;
Contributions in peer-reviewed journals that, regardless of their research objectives or research design (empirical as well as nonempirical articles), report on any general prerequisites for meaningful social work involvement in palliative care.
Information sources and search methods
Three electronic databases (Web of Science, Scopus and Pubmed) were searched for contributions in peer-reviewed journals published between 2000 and April 2021. Although the inclusion of grey literature is a common feature of scoping reviews, it was not included in this study due to practical constraints as it would result in an unfeasible number of articles up for screening. Nevertheless, in a newer research field as palliative care, seminal ideas can often be found in nonempirical work. Nonempirical contributions such as editorials, letters to the editor or essays were therefore also included in case they report on any general prerequisites for meaningful social work involvement in palliative care.
The search string contained two exposures. Exposure A contained the search terms: Social work OR Social work practice. Exposure B contained the search terms: Palliative care OR End-of-life care OR Hospice care. In the selection of sources of evidence, we interpreted the term palliative care broadly in accordance with the definition set out above. We therefore looked at articles covering the involvement of social workers within formal palliative care services as well as the involvement within the broader context of death, dying and bereavement. The main reason why we limited exposure B to the aforementioned search terms was to make the search more manageable. ‘Prerequisites’ was not included as a search term as most articles mention prerequisites indirectly, which would have resulted into a number of included articles that would have been too narrow. Exposures A and B were combined into a search string using the Boolean operator AND. The search string was used in each database independently.
Selection of sources of evidence
Duplicates were removed before the selection process. Titles and abstracts were screened by a single researcher. Articles were included if they specifically mentioned the involvement of social work in palliative care. Subsequently, two researchers independently conducted a full-text screening and selected articles that met all three eligibility criteria described above. Articles selected by just one of the researchers were kept separate. The articles kept separately were then reviewed again, after which a final decision on in – or exclusion was made.
Data charting process
Each time an article was included the two researchers listed the most important information concerning that article: its authors, its year of publication, its country of origin and some key findings relating to the research questions. This activity led to a preliminary idea on how to synthesise the results.
Quality appraisal
As the main aim of a scoping review methodology is not to assess the quality of the included articles, a formal quality appraisal was not undertaken. Nevertheless, articles whose methodology and presentation of findings looked questionable or flawed were not included.
Synthesis of findings
The included articles were uploaded in NVIVO 12©. A single researcher then searched for content that was considered relevant for answering the research questions following a process of open coding. Subsequently, in an axial coding process, these codes were combined into overarching codes. The relevant information in the overarching codes, which correspond to the prerequisites for meaningful social work involvement in palliative care, was than qualitatively analysed.
Findings
Selection of sources of evidence
Starting from the 1684 articles that were up for screening, a total number of 170 articles were included at the end of the selection process. This process is visualised in the PRISMA flowchart – as adapted from Moher et al. 19 – in Figure 1. During the first step, a single researcher screened titles and abstracts, resulting in the exclusion of 1324 articles. During the second step, the remaining 360 articles that were up for full-text screening were examined by two independent researchers. In the end, another number of 190 articles were excluded with reasons. The total number of included articles in this scoping review is therefore 170.

PRISMA flowchart.
Characteristics of sources of evidence
Table 1 presents the characteristics of the sources of evidence. The vast majority of the included studies originate in English-speaking countries, with the United States as a clear frontrunner. Some studies have mixed origins. As far as the design of the included studies is concerned, most contributions are case reports on small-scale studies, intervention programme descriptions or pilot tests, followed by literature reviews and cross-sectional studies.
Characteristics of the sources of evidence.

Frequency of mentioned prerequisites
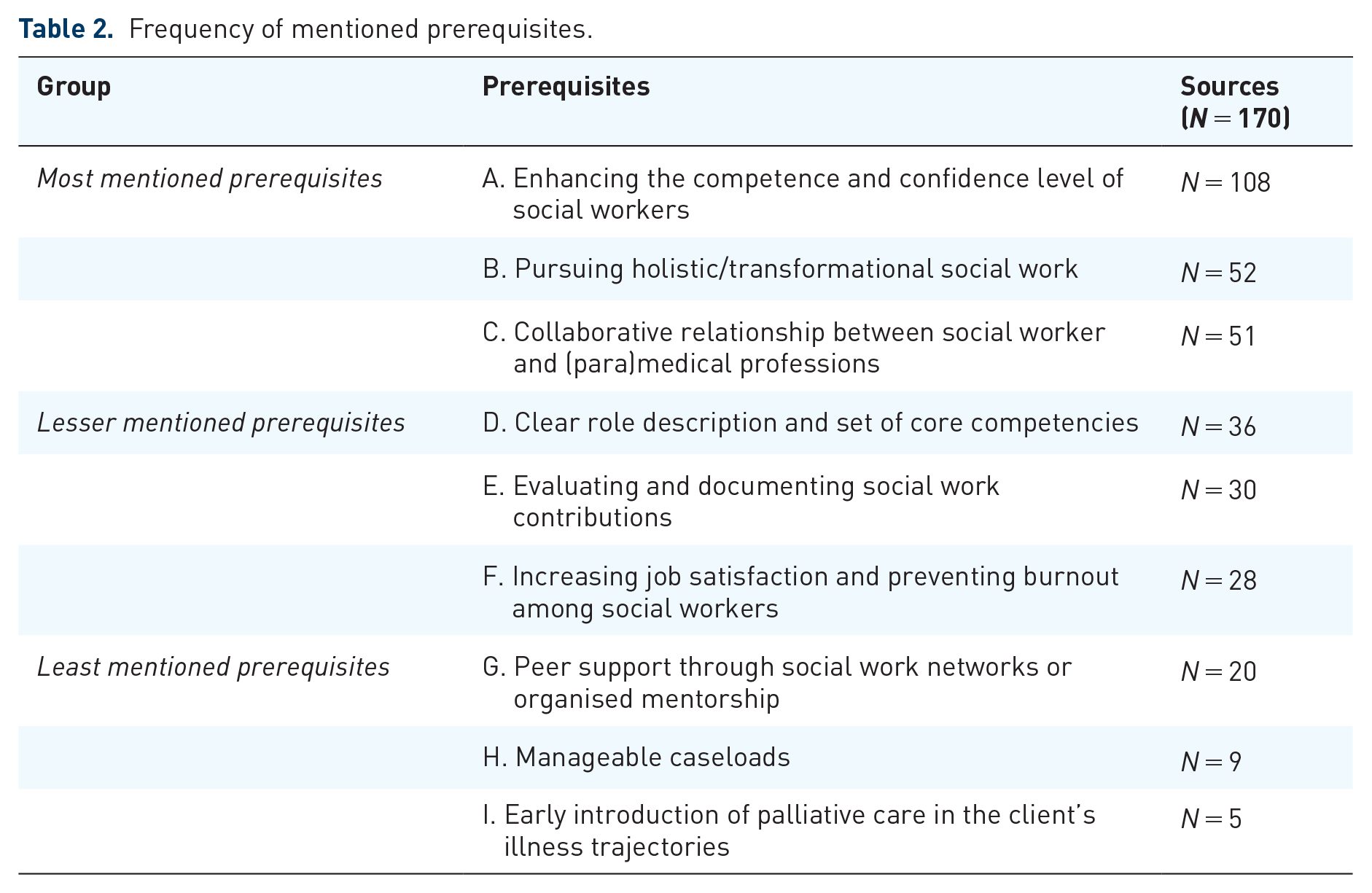
Following the processes of open and axial coding, nine substantial prerequisites for meaningful social work involvement in palliative care were found. In terms of frequency in which these were mentioned in the included studies, three groups can be discerned: most, lesser and least mentioned prerequisites. These groups are summarised in Table 2. A Supplemental File Appendix lists all of the sources of evidence and indicates which prerequisites are mentioned.
Frequency of mentioned prerequisites.
A qualitative synthesis of prerequisites
Enhancing the level of competence and confidence of social workers
There are multiple dimensions to ‘being competent and confident’, which is mentioned as the most important prerequisite for meaningful social work involvement in palliative care. Some authors have emphasised the broad need for culturally competent practice,20–22 whereas other authors have focused on specific skills such as contributing to ACP8,23 and emotional or grief counselling.24,25 Furthermore, authors have encouraged social workers to gain specific knowledge on physical aspects of death,26,27 dementia 28 and the relationship between physical and psychosocial symptoms. 29
How can this prerequisite be realised in practice? The literature presents two recommendations to enhance the competence and confidence of social workers in palliative care. A first path is to improve the palliative care content in (under)graduate social work curricula. However, opinions differ on the concrete amount of content in these curricula. On one hand, several authors have specifically suggested to include at least a minimum amount of general palliative care content in social work curricula.30–33 On the other hand, authors have specifically mentioned that social work curricula should ideally include a mandatory and specialised component on palliative care.34–36 A second path is to develop postgraduate or other continuing education opportunities for social workers.24,37,38 Preferred formats for continuing education are participation in local or regional conferences and workshops or participation in online courses. 39 Furthermore, forms of peer-to-peer learning between skilled social workers and social workers new to palliative care can improve competence and confidence40,41 or train skills that were not covered in undergraduate curricula.8,33
In practice, ‘competence and confidence’ is rather a product of undergraduate education, continuing education and so-called ‘on-the-job learning’.18,22,31,42 Given the increasing number of people with palliative care needs, the development of social work competencies should at best not solely rely on on-the-job-learning and continuing education. 43 However, Sumser et al. 10 found that only 46% of respondents felt prepared by their social work curricula, whereas a vast majority of respondents reported learning through interprofessional collaboration or peer-to-peer contacts, 81% and 74%, respectively. This observation is not surprising as many studies have shown the lack of palliative care content in the professional socialisation of social workers, resulting in inadequate levels of competence and confidence after graduation.18,25,38,44–46 Although there are clear gaps in undergraduate social work curricula, it may be a more fruitful endeavour to focus on continuing education as undergraduate curricula are already crowded with topics.47,48 The development of continuing educational interventions must nonetheless account for multiple barriers to participation such as costs and time away from work, lack of adequate social work content 32 and lack of external funding. 38
Pursuing holistic and transformational social work
Both holistic and transformational practices serve as a second prerequisite for meaningful social work involvement. Not only are these practices central to the unique role of social workers in palliative care but they also contribute to job satisfaction as they put typical social work values in practice. 49
By holistic work we refer to the ‘broader picture’ – fostered by the ‘person in environment approach’ – in assessing clients’ needs. Social workers should always realise that clients are embedded in a social context and that multiple environmental factors shape the unique position of each client.12,50 Holistic work therefore means that the care that social workers offer extends beyond the individual client to family and other actors in the client’s social environment.51,52 Nevertheless, in contemporary diversifying societies, the main challenge for holistic social work increasingly relates to ‘culturally sensitive practice’ in dealing with diversity,21,51,53,54 multilingualism 55 and diverse spiritual beliefs.21,56
While holistic social work relates to a broad assessment of clients’ needs, transformational social work puts the social worker as an intermediary figure between clients and society. Based on their work with individual clients and families, the task of social workers is then to allude to positive transformations in society. 57 Examples include influencing policy and practice58,59 by advocating for appropriate service design for marginalised and disadvantaged populations 60 or initiating a public debate on combatting inequalities in the access to palliative care.54,61,62 These kind of interventions were labelled by Reith and Payne 52 as ‘social work macro interventions’.
How can this prerequisite be realised in practice? Three factors facilitate the implementation of holistic and transformational social work practices. First, educational programmes must equip social workers to develop holistic and transformational assessment skills. 63 This includes general programmes as well as educational programmes aimed at specific minority groups – such as those commented on by Arthur 64 and Bekkema et al. 1 Second, Csikai and Martin 65 suggested that holistic practice is linked to an early introduction of palliative care in the end-of-life trajectory, providing social workers with more opportunities to engage with clients. Third, adequate staffing ratios of social workers in palliative care services avoid high caseloads, creating more opportunities for holistic practices. 66
Collaborative relationship between social workers and (para)medical professions
A collaborative relationship between social workers and (para)medical professions provides more opportunities for social workers to get involved in palliative care and – as a result – to influence practices.
Four examples illustrate this argument. First, a collaborative relationship is important in advocating for the adequate treatment of nonmedical issues.18,63,66,67 Examples consist of addressing psychosocial barriers to symptoms reporting; 29 long-term financial implications of cancer treatment 68 and the family context of illness and care. 69 Second, a collaborative relationship means that social workers can advocate for the early integration of palliative care in clients’ treatment trajectory.68,70 Third, social workers can be better intermediaries between a client and the multidisciplinary team in case of a good collaborative relationship.18,62,67,70,71 This is important to perform typical social work tasks in palliative care such as facilitating difficult client–physician conversations 43 or addressing the needs of clients who do not understand the medical jargon. 34 In this respect, the social worker serves – as Otis-Green et al. 27 put it – both ‘as a consultant to the team and as the voice of the patient’. Fourth, a collaborative relationship with other professionals leads to a higher job satisfaction for social workers. 72
However, social workers often experience multiple barriers in collaborating with (para)medical professions. This situation can possibly be explained by the dominance of the medical model in palliative care prioritising clinical needs48,73 and, as a result, perceiving social work as ‘ancillary to medicine’. 74 Kimura et al. 75 found that medical professionals often refuse to share essential medical information with social workers, which substantially reduces the chances of social workers to influence multidisciplinary practice. 63 Furthermore, evidence shows that social workers often feel unappreciated by other professionals in the team 76 while team meetings as such are perceived as not suited for a holistic assessment of clients’ needs. 77 The effect of an exclusive physical focus in medicine on the social work role is best illustrated in the studies by Lawson 78 and Stein et al. 8 They found that social workers tend to adopt a more leading and coordinating role in hospice settings than in a highly medicalised setting such as the hospital, in which nurses and physicians may be the most important coordinators.
How can this prerequisite be realised in practice? Based on the reviewed studies, there are two ways to stimulate a collaborative relationship between social workers and (para)medical professionals. On one hand, social workers can clearly express the value of the bio-psycho-social model in palliative care practice and the important position they could have as professionals within this model. This means that it is equally important to clearly articulate how their role differs from other professional roles as to avoid nurses and psychologists taking their places. 52
On the other hand, the literature emphasises the need for ‘competent and confident’ social workers who can take up their rightful position in palliative care. Elementary medical knowledge79,80 and knowledge on palliative or end-of-life care81,82 are therefore a necessity to foster cooperation between social workers and (para)medical professions. Furthermore, interdisciplinary training opportunities respecting the diversity between relevant disciplines in palliative care83,84 can increase cooperation among all professionals.28,36,48,85,86 In any case, this kind of training should be implemented into educational curricula from the early stages of professional socialisation. 36 A concrete example can be found in the contribution by Neuderth et al. 87 who reported on an interdisciplinary training for medical and social work students in Germany, which was received as highly satisfactory.
Clear role description and set of core competencies
A clear role description of social work in palliative care – operationalised by a well-defined set of core competencies – is another prerequisite. 88 The previous paragraph already mentioned the importance of social workers clearly articulating their role. Yet, the dominant focus on physical aspects in palliative care often jeopardises the role articulation of social workers.51,89 This may certainly be the case if there is no role description at all. The articulation of the social work role is important in multidisciplinary cooperation, but without knowing the specificities of that role, it is hard to articulate it.
There are three benefits associated with a clear role description of social work in palliative care. First, a clear role description with an outlined set of core competencies makes the benefit of social work visible to other professionals,90–92 reduces the chances of role conflicts2,21 and helps to maintain professional boundaries. 93 Role clarification therefore enhances multidisciplinary cooperation. 94 Second, it would bring about advancements in educational programmes and, as a result, more competent and confident social workers.30,91,95–97 If social workers cannot clearly articulate their role, they will feel less confident about their own capacities and, as a result, take up a less active involvement in palliative care. 98 Third, it becomes easier for the assessment and evaluation of the social work contribution in palliative care practice.9,91,99 As Munn and Adorno 98 put it, ‘without a clear definition of what social workers bring to the table, it is difficult to place a value on the social work contribution’.
How can this prerequisite be realised in practice? The reviewed studies call for a clear theoretical and operational description on the social work role in palliative care. However, this largely depends on the national context.94,100 Concrete outlines of social work competencies have already been developed in Canada 91 but also a general outline for European countries already came into being. 101 In the United States, a first comprehensive outline of core competencies was established by Gwyther et al. 16 and further elaborated by Head et al. 7 in a nationwide hospice and palliative care social work job analysis. For other countries, there either are no peer-reviewed records describing such outlines or they may not be published in English. However, it may be that for many countries – especially those without a long-standing tradition in social work research – a clear role description and set of core competencies is still lacking.
Evaluating and documenting social work contributions
Although the social work profession has been slow in evaluating and documenting its contributions,7,13 these activities form an important prerequisite for meaningful involvement in palliative care. Without a sense of proven expertise, the value and effectiveness of social work interventions can easily be questioned.88,102,103 Documentation and evaluation practices could thus empirically demonstrate the added value of social work in palliative care.7,9,54,61,104
Yet, multiple factors complicate the evaluation and documentation of social work practices. First, the absence of a clear role description on social work in palliative care makes evaluation and documentation difficult.91,95,105 Second, organisational conditions can prevent social workers from practice evaluation and documentation, for example, because they have only minimal access to patients as a result of cost-saving policies, 88 or because they are not involved in decision-making concerning evaluation instruments. 104 Third, social work interventions are not easily quantifiable while narrative documentation is often not considered sufficient. 106
How can this prerequisite be realised in practice? In the United States, a vast advancement in the field arose from the development and testing of the Social Work Assessment Notes (SWAT)104,107,108 and the introduction of a social work certification exam in palliative care. 7 In other countries, such initiatives may, however, still have to be taken to realise this prerequisite. Furthermore, the importance of evaluating and documenting social work interventions can be addressed in educational curricula6,109 or at social work conferences. 9 Apart from the initiatives taken by the social work profession itself, there are also organisational responsibilities to facilitate evaluation and documentation practices. It is the responsibility of agencies and organisations to include data on social work activities in, for example, medical records or administrative databases. This would highlight and document their specific role within the organisation.51,110
Increasing job satisfaction and preventing burnout among social workers
Increasing job satisfaction among social workers and preventing burnout is another prerequisite for meaningful involvement in palliative care. It is important to recognise that the emotional burden of social work practices in this field can have a substantial effect on job satisfaction.43,52,111–113 Previous research has evidenced a low job satisfaction among social workers in palliative care settings due to the high stress–high loss environment, resulting in a considerable prevalence of burnout. As personal experiences with death, dying and bereavement influence professional care delivery,46,114 social workers who have more of those experiences may be better equipped for palliative care practice. Furthermore, low job satisfaction has also been linked to a low understanding of the social work contribution among other professionals, 90 a general feeling of being disvalued in multidisciplinary practice72,76 and the inability to put holistic social work values into practice due to various policy or organisational constraints. 49
How can this prerequisite be realised in practice? The reviewed studies indicate the importance of coping skills to increase job satisfaction and prevent burnout. Social workers should learn coping skills in dealing with death, dying and bereavement as these issues are inherent to palliative care settings.115,116 Such coping skills should concern the ability to reflect on one’s own values, attitudes or anxieties regarding the end-of-life phase.44,117 Knowing one’s own worldview and beliefs is required to honour the beliefs of others and making objective recommendations. 83 Additional competency-based trainings can therefore serve as a solution for inadequate preparation in dealing with death, dying and bereavement during social work educational programmes.95,112 These trainings should enhance social workers’ emotional readiness and comfort levels in end-of-life settings. 46
Both educational institutions as well as organisations of employment are responsible for the job satisfaction of social workers and prevention of burnout. On one hand, educational programmes should include coping skills that social workers can use in their practices with clients facing end-of-life challenges.46,56,112,115,118 On the other hand, various organisations of employment – such as home care or hospice care services – should stimulate job satisfaction and provide self-care and coping strategies for their social workers.72,76,113,116 Moreover, as the likelihood on job satisfaction of social workers is higher in organisations where holistic social work values can be put into practice, it is important to align the organisational culture with those values. 49
Peer support through social work networks or organised mentorship
Social workers often require support from their peers in dealing with clients’ end-of-life matters, which we denote a prerequisite for meaningful social work involvement in palliative care. Previous research has found that social workers prefer support from other social workers over the support of other professionals such as nurses or physicians.77,107 In a high stress–high loss environment such as palliative care, social workers ‘may experience feelings of isolation when they have no local social work colleagues with experience in this field of practice’. 119 Hence, insufficient support is linked to job dissatisfaction and, as a result, a higher prevalence of burnout.46,113,120
How can this prerequisite be realised in practice? The reviewed studies indicate that peer support among social workers can be realised through existing social work networks or organised mentorship. In this respect, experienced social workers can increase the competence and confidence of less experienced social workers or social workers in training.8,10,40,41,121 A good example to illustrate this argument is the case of ACP. As only few social workers receive any content on ACP in (under)graduate curricula, it is a typical example of on-the-job learning. Therefore, experienced and skilled social workers play a vital role in preparing their less experienced peers in ACP. 8
Manageable caseloads
High caseloads are considered as an important challenge,39,122 meaning that assuring manageable caseloads is a prerequisite for meaningful social work involvement in palliative care. In their study, Munn and Adorno 98 suggested that the involvement of social workers may be enhanced through a lower staff to resident ratio. As they put it, ‘social workers are unable to become as involved as needed due to the large number of residents for whom they are responsible’.
There are two particular disadvantages of high social work caseloads in palliative care. On one hand, high caseloads resulting from low staffing ratios form a barrier for holistic social work practices. 62 When caseloads are high, there is simply not much time for in-depth contributions,13,123,124 resulting in inadequate social services. 125 On the other hand, high caseloads increase the risk on burnout. 113
How can this prerequisite be realised in practice? The reviewed studies recommend organisations to either decrease the social work caseload or increase social work staff ratios as they are two sides of the same coin. Following these strategies helps to assure the occurrence of holistic social work practices and avoids social workers from getting disillusioned. Nonetheless, Munn and Adorno 98 noticed that the quest for attracting additional social work staff is difficult to justify without evidence on the contribution of social work in palliative care. Therefore, the evaluation and documentation of their contributions forms a prerequisite to increase social work staffing.
Early introduction of palliative care in clients’ illness trajectories
A final prerequisite for the meaningful involvement of social work in palliative care relates to the early introduction of palliative care in clients’ illness trajectories. In practice, palliative care is usually initiated but late in the illness trajectory, which automatically reduces the involvement of social workers.39,123
How can this prerequisite be realised in practice? Social workers should have sufficient opportunities to facilitate the early introduction of palliative care during multidisciplinary discussions. 62 Although physicians usually have the final say in the start-up of palliative care, social workers can help to make the situation of a client negotiable. They should therefore be assigned to clients shortly after diagnosis as to inform them and their relatives on the options during the illness trajectory.126,127 This allows clients to further discuss these options with their physicians. The inclusion of social workers shortly after diagnosis is important as ‘the lack of inclusion of the social worker in initial diagnostic conversations’ forms a barrier to the implementation of holistic social work practices in the later palliative trajectory. 62 Therefore, Clausen et al. 63 argued that social workers should be integral members of the multidisciplinary care team to build durable relationships with clients and their families.
Discussion
This study identifies nine substantial prerequisites for the meaningful involvement of social workers in palliative care and summarises the recommendations or evidence-based practices that have been mentioned in the literature to realise them. The prerequisites are situated on two substantial levels. The first level concerns the individual capacities of social workers. For instance, social workers should ideally be competent and confident in palliative care practice, which means that they should pursue holistic and transformational social work practices, collaborate smoothly with (para)medical professions and know how to evaluate and document their own practices. The second level concerns the contextual factors that structure the practices of social workers in palliative care such as the composition of social work educational curricula, the care model and the characteristics of the organisations that social workers operate in.
Three critical comments can be made here. First, the considerable overlap between the prerequisites illustrates that the substantial levels on which they are situated are mutually responsive. An example can illustrate this argument. On one hand, the extent to which social workers are competent and confident in palliative care substantially depends on the amount of course content on palliative care during their education. On the other hand, the palliative care model in which social workers operate and the organisational structure of the agencies in which social workers are employed influence how their capacities are used in practice. A number of prerequisites can thus be realised by social workers – and social work educational institutions – whereas other prerequisites rely on contextual factors such as the care model and organisational or policy regulations. Nevertheless, a majority of articles focusses on the level of individual capacities of social workers. The question is then whether the contextual level is less important or simply under researched. In some cases, it might be possible that social workers have essential palliative care capacities but are unable to put them into practice due to organisational or policy constraints.
Second, although we interpreted the involvement of social workers in palliative care broadly – namely their involvement in the broader practice field of death, dying and bereavement – and not in just formal palliative service delivery, the majority of included articles is focused on the latter. A substantial body of literature has thus explored social work involvement in terms of being a member of a palliative care team, alongside (para)medical professions. However, not all social workers facing issues concerning death, dying and bereavement are part of a palliative care team. As palliative care needs will only rise in the future, it is recommended to know how social workers can be maximally involved in the broader context of death, dying and bereavement.
Third, the fact that a vast majority of articles included in this scoping review originate in a limited number of English-speaking countries – and especially the United States – could reveal a lack of research on this topic in other countries. It is rather unlikely that only a small number of researches in non-English-speaking countries are publishing their work in English.
The major contribution of this review is that it is the first step in presenting a comprehensive list of prerequisites for meaningful social work involvement in palliative care and the recommendations or evidence-based practices to realise them. Furthermore, the insights gathered in this review have consequences for future intervention development in enhancing social work involvement in palliative care and maximising their contributions. Ideally, interventions should carefully select a multiple number of prerequisites. It is, for example, not sufficient to ensure that social workers are competent and confident by composing the best educational curricula, as the care model they operate in and the organisational structure in which they are employed also influence the nature of their involvement in palliative care. It is nonetheless important to note that any meaningful form of involvement starts with a clear role articulation of palliative care social work, operationalised by a set of core competencies. Without a clear idea of what social workers do or should do in palliative care, there is no point in intervening.
This review has three limitations. The first limitation relates to the typical absence of a formal quality appraisal in scoping reviews, which means that the included evidence is not graded in terms of research quality. Furthermore, although grey literature was not included in this scoping review, we included nonempirical contributions such as editorials and essays.
The second limitation concerns the fact that a vast amount of contributions included in this review originate in countries where, despite significant national differences, individual psychosocial casework is the dominant approach to the social work profession. Høgsbro and Shaw’s 128 warning to the disproportional influence of American scholarship in social work research is especially relevant here as American social work is characterised by a strong emphasis on casework and a higher degree of professionalisation in comparison with other countries.129,130 Furthermore, the influence of the Social Work Hospice and Palliative Care Network (SWHPN) and the introduction of a certification exam for palliative care social workers (APSHW-C) have caused a significant focus on individual competencies in American social work research. This may partially explain the emphasis in our results on individual social work capacities and less on contextual factors.
The third limitation closely follows the second and relates to the impossibility to generalise the insights found in this scoping review as prerequisites for meaningful social work involvement may be highly context-specific. Nevertheless, this could also be considered as a strength of this study. The listed prerequisites – combined with a summary of recommendations and evidence-based practices on how to realise them – provide potential pathways for future intervention development in enhancing the involvement of social workers and maximising their contributions in palliative care. With this scoping review, future researchers could determine which prerequisites are important in their area, whether or not they are realised and how they can be realised.
Implications for further research and social work practice
There are three implications for further research. First, more research is needed on the contextual level of social work involvement in palliative care. Second, further research should tackle the question on how the profession can influence the broader practice field of death, dying and bereavement to compensate for the overemphasis on formal palliative service delivery in contemporary research. Third, we call on researchers from non-English-speaking countries or regions to critically examine the involvement of social workers in palliative care and to make their evidence available in English.
A final implication of this scoping review relates to a call for action for social workers to keep increasing their influence in the broader field of death, dying and bereavement – particularly as it relates to key social work activities in community work, advocacy and social justice.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524211058895 – Supplemental material for How can social workers be meaningfully involved in palliative care? A scoping review on the prerequisites and how they can be realised in practice
Supplemental material, sj-docx-1-pcr-10.1177_26323524211058895 for How can social workers be meaningfully involved in palliative care? A scoping review on the prerequisites and how they can be realised in practice by Brent Taels, Kirsten Hermans, Chantal Van Audenhove, Nadine Boesten, Joachim Cohen, Koen Hermans and Anja Declercq in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524211058895 – Supplemental material for How can social workers be meaningfully involved in palliative care? A scoping review on the prerequisites and how they can be realised in practice
Supplemental material, sj-docx-2-pcr-10.1177_26323524211058895 for How can social workers be meaningfully involved in palliative care? A scoping review on the prerequisites and how they can be realised in practice by Brent Taels, Kirsten Hermans, Chantal Van Audenhove, Nadine Boesten, Joachim Cohen, Koen Hermans and Anja Declercq in Palliative Care and Social Practice
Footnotes
Acknowledgements
This study is part of the project ‘CAPACITY: Flanders Project to Develop Capacity in Palliative Care Across Society’, a collaboration between Vrije Universiteit Brussel, Ghent University and the University of Leuven, Belgium.
Author contributions
BT conducted the main writing process and acted as first reader in the selection of articles. NB acted as second reader in the selection of articles. BT, KiH and AD prepared the first draft of the manuscript. CVA, NB, JC and KH participated in creating the concept of the study and, in discussions on earlier versions of the manuscript and, in critically revising the different versions of the manuscript. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by the Research Foundation – Flanders, file number S002219N.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.