
Abstract
Background:
There has been an emerging trend of adopting a death doula, a non-medical advocate and guide for people at the end of life and their families. While there has been growing empirical research regarding the work of death doulas, no studies have been undertaken with the families who have engaged them.
Objectives:
To understand the experiences of families who used a death doula in terms of what they did for the patient and family; to understand the benefits and drawbacks of using a death doula; and to use family insight to determine cultural shifts towards death and dying, and what the death doula phenomenon tells us around our attitudes towards death and dying.
Methods:
We recruited and interviewed 10 bereaved family members to learn about their experiences using a death doula. This qualitative research took an interpretive phenomenological approach, and thematic analysis was used to analyse the data.
Results:
The most valuable attribute the families gained from death doulas was an increase in death literacy resulting in personal empowerment. Empowerment enabled positive end-of-life experiences for the family and personalised deaths for the patient. A novel finding was that the connections and knowledge shared between the death doula and family had a resonant effect, resulting in families being more comfortable with death and keen to share their knowledge with others. Therefore, family engagement of a death doula led to an increase in community awareness around death and dying.
Conclusion:
Family members’ experience with a death doula was overwhelmingly positive, empowering them practically and emotionally to deliver the best end-of-life care. Empathy and sharing of knowledge by death doulas were valued by families and resulted in an increase in death literacy which provided families with opportunities to ‘pay it forward’. Furthermore, the relationships formed between doulas and families have the potential for a lasting, resonant effect.
Plain language summary
To date, there are no research studies with a focus on family experiences using death doulas for end-of-life care. We interviewed 10 family members from Australia and the United States to understand what benefits death doulas provided, what complicating factors might be involved when engaging them and what value and impact they had on end-of-life care for families.
The most valuable attribute the families’ gained from death doulas was an increase in death literacy. There was a direct connection between this and a sense of empowerment for patients and families. Empowerment enabled positive end of life experiences for the family and personalised deaths for the patient.
Introduction
It is becoming increasingly common for people to choose to die at home where possible 1 ; however, this requires both formal care provision and informal care; the latter often provided by family and friends and other social networks.2,3 Family members undertake many tasks and experience physical, emotional and financial burdens in the process,4,5 often trying to manage alone with services that are inconsistent and with health providers with limited time to provide the help and support required. 6 Increasingly, there are also those with no family support at all. 2
There has been an emerging trend of engaging a death doula (DD), a non-medical advocate and guide for people who are at the end of life (EoL) and their families.7,8 A DD provides guidance and support in the time leading up to death and in the period after providing many and varied services including helping with advance care planning, providing respite, helping with practical tasks and physical care, and providing companionship.9,10 The DD role has its roots in the fundamental belief that the medicalisation of death has removed much in the way of death awareness and death literacy, including the ability to talk openly about death. 11 In more practical terms, the movement reflects what some have identified as a shift in health services back into the community. 12 Parallels to the DD role can be found within Australian Indigenous communities, where support in dying (e.g. spiritual care) is provided at a grassroots and culturally appropriate level within the community, a role formalised in more recent years as that of Aboriginal and Torres Strait Islander health workers. 8
The DD role has been under scrutiny in the literature as one, that while regulated in Australia, remains unregistered with no standardised education requirements.10,13,14 This is also true in the United States with no state or federal oversight or agency overseeing the DD certification process. 15
While the topic of DDs has been popular in the media, 16 it is only in the past 5 years that there has been a growing number of descriptive articles, followed by some empirical research. This has included literature reviews,8,10 surveys and interviews with DDs,7,14,17–20 a survey with DD training organisations 21 and two studies on DD models of care.22,23 While this relatively new phenomenon is gaining more focused attention and research, it has consistently focused on the DDs perspective, without to date, any research privileging the voices of families who have engaged a DD. Given the ultimate arbiter of the usefulness of any service role is the end user, in this case family members, it is therefore vital that an examination of their experiences be undertaken as the most appropriate way to investigate perceived value and family satisfaction with the care provided by DDs.10,24 The aims of this qualitative research were therefore threefold:
(1) to understand the experiences of families who used a DD in terms of what they did for the patient and the family.
(2) to understand both the benefits and drawbacks of using a DD from the families’ perspective.
(3) to use family insight to inform understandings of cultural shifts towards death and dying more broadly and what the DD phenomenon tells us culturally around our attitudes towards death and dying more broadly.
Methods
This qualitative research took an interpretive phenomenological approach 25 to understand the lived experience of families who engaged in the services of a DD via an in-depth inquiry.
Study recruitment
Names that have been included are pseudonyms. When recruitment stalled, a modification request was submitted to the ethics committee, and approval was received, to recruit more broadly via the international DD training organisations that we had previously reached out to.
We began by approaching those who had assisted with recruitment for our previous studies across Australia. We also approached carer organisations, funeral directors, death café networks and community centres. After a limited response over 6 months, we increased our scope internationally approaching independent EoL groups, national DD organisations and larger international DD organisations. All organisations were provided with a description of our research for circulation. We were also contacted by a colleague in the United States with a special interest, who was a DD herself and who offered to help with recruitment.
Inclusion criteria for our participants were members of the public aged between 18 and 80 years who had used a DD to assist them with the EoL care of the patient and who were now bereaved. Initially, we sought those whose experience was between 3 and 6 months prior to interview. However, due to the difficulty in recruitment, we allowed participants who had used a DD up to 3 years prior. Only one participant did not fall in this range, her experience being 6 years prior. A study by DiBiasio et al. 26 found stable responses from participants between 3 and 9 months following the death of hospice patients, with Bentley and O’Connor 27 describing bereaved family members feeling most comfortable being interviewed within the first 5 months of bereavement and that the timing of such interviews should be at their discretion. It was also felt to be important to not only have some distance between the death but also (we thought) distance from the DD, with any current caregiving experience and reliance on the DD for support and guidance, potentially colouring the experience.
The research assistant (an experienced female PhD qualified qualitative researcher) contacted prospective participants in the United States and Australia, providing study information sheets detailing the purpose of the research and conducting interviews with 10 family members who had engaged the services of a DD for a loved one. Five family members were from Australia and five from the United States and all but one was female. All participants contacted the researcher if interested in participating and none subsequently dropped out. Those being cared for were predominantly spouses (6), parents (3) and one great-aunt (see Table 1).
Family members.

DD, death doula; HPC, Health Care Professionals.
We conducted nine semi-structured interviews online via Teams or Zoom, and one via telephone, with the interviewer not known to the participants beforehand. All participants were interviewed alone, with each interview of approximately 1-h duration. Field notes were not taken, as each interview was audio and visually recorded and transcribed verbatim via a third party with a non-disclosure agreement in place. All participants were provided with a consent form and information sheet prior to the interview. The information that we were interested in came in the form of question prompts, based on the researchers’ previous work. The questions were not piloted. Questions were posed about the person who had died, the bereaved family members’ relationship with them, any family support available and how they came to engage a DD. From there, we were interested in how the DD supported both the dying person and the family member (i.e. what they helped with). Other areas of interest included payment, other family members’ feelings towards the DD and any positive or negative aspects related to engaging a DD. Interviews lasted approximately 1 h and were digitally recorded and transcribed verbatim by an independent company. No interviews were repeated or followed up.
Participants were offered the opportunity to view the transcriptions for verification, and some participants expressed interest in learning about our findings. Participants were provided with a $30 gift card to thank them for their time. Unfortunately, though, this attracted over 200 scam emails that required verification screening, such as for duplicate responses and similar IP addresses. This is not an isolated incident as a result of online recruitment,28,29 but it does add to the complexity and the timelines.
Data analysis
We used a combination of both deductive and inductive coding to organise and analyse the qualitative data. As this research supplemented all our previous studies on DDs, we had very specific aims as noted above. Although deductive analysis usually begins with theoretical propositions or is guided by one theory, this was not in the design. Furthermore, it could be described as ‘theoretical thematic analysis’ only in terms of providing a more detailed analysis of some aspects of the data. 30 However, the researchers remained reflexive and mindful of this, recognising transparency is important when conducting inductive analysis with presuppositions. 30 In specifically addressing reflexivity, as four of the authors have a track record in DD research, the second author conducted the interviews and led the data analysis with no previous history in DD research and therefore no preconceptions. All participants checked the transcripts with no changes made, and verbatim exemplar quotes were provided.
We began with a coding table (or code book) before commencing analysis based on the research questions and aims. 31 This table was assessed by all the researchers for coherence. Once agreed upon, 10 descriptive codes were tabulated to capture the aims of the three research aims and were created as nodes using Nvivo v20 software (Lumivero, V13 (2020, R1). As data were entered into the software, preliminary organising of the data was categorised under each descriptive node. Codes grouped in this way formed the key features of each participant’s experience. Meaningful aspects of text matching these descriptive codes, such as ‘benefits’ or ‘change and impact’, were then identified and grouped under these codes. 31
Transcripts were coded again, this time inductively to identify the main themes common across cases. We adopted Braun and Clarke’s 30 approach to thematic analysis which they identify as phase IV of analysis. This is where the initial themes are refined, some collapse into each other and some may be eliminated and phase II, where we determine the validity of individual themes in relation to the data set. 30 Once this process was complete, three of the researchers met to discuss the themes and their significance with regard to the research objectives. All authors corresponded to discuss the main insights from the data and the main themes were discussed again to determine the ‘essence’ of what each theme was about in relation to the data. 30 Once there was agreement, three main themes (with subthemes) were identified.
Results
The results indicated that engaging a DD enabled an increase in death literacy which led to feeling prepared and empowered. As a broad concept, death literacy pertains to obtaining knowledge and skills that allow people to understand and act upon EoL care options. 32 The concept of death literacy suggests that caring for someone at the EoL is not only a learning experience but strengthens the capacity for caregiving and encourages sharing that learning with others. 33 This was evident in a majority of cases in this study.
The amount of direct contact the DD had with the patient largely related to the context of the patient’s condition and what assistance the family needed. In terms of fiscal arrangements, in four cases, there was no direct patient contact at all, with the families enlisting DDs for emotional and practical support for the family member. Six of the 10 paid a fee for their service, 3 were voluntary and 1 family member could not remember having paid or paid a minimal amount. It has been argued that since DDs are paid for their services, it is assistance that only those with a higher socio-economic status can afford. 17 However, in our study, none of the study participants considered the cost of their DD unaffordable, and one study participant said the cost was negotiable. Two participants from the United States were supplied DDs as part of their hospice package. One participating family member from Australia was on a pension and still managed to afford hiring a DD. DDs were, for the most part, on-call and responded to the needs of the family as they arose, and no conflicts were reported in their interactions with other healthcare professionals who were involved in the care of the patient.
Engaging a DD appears to serve both the practical and emotional support necessary for personalised and informed EoL care. The emphasis on the value of DDs from the families in this study was the empathy and knowledge they provide, the bonds they formed and their ability to enable a meaningful EoL care experience. These values were identified through three main themes: (1) preparedness, (2) empowerment and (3) connections. Each theme then had subthemes.
Theme 1: Preparedness (subthemes: physical, practical and emotional)
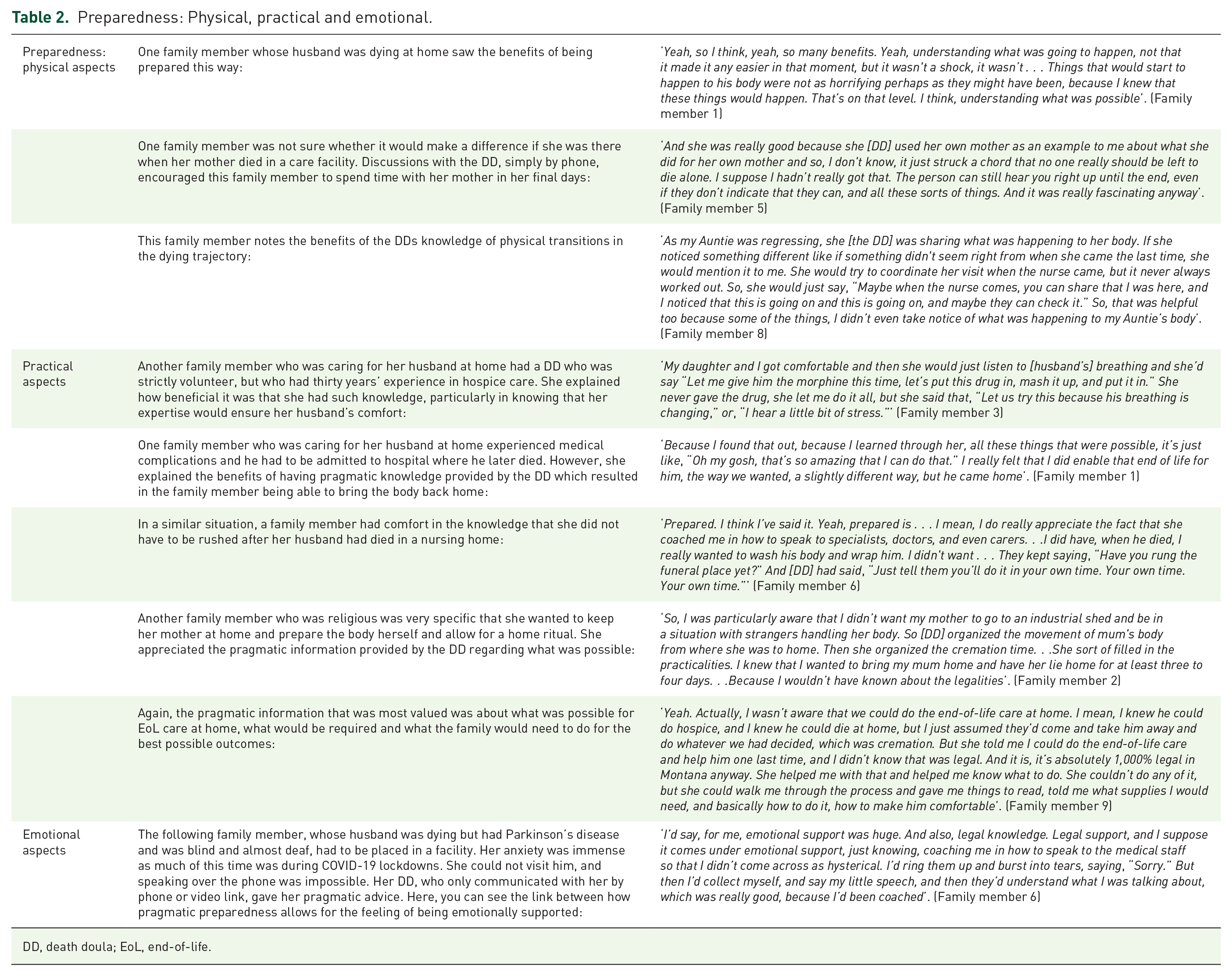
Preparedness around death and dying encompasses many elements. These can include medical, practical, psycho-social and spiritual preparedness.34,35 Family member’s emphasis on feeling prepared came from the knowledge about death and dying processes, and about what pragmatic information they needed to care for the patient. One family member said, ‘She supported me rather than him, so that I could keep my spirits up and keep supporting him. That’s basically what I was wanting’.
For those participating in our study, preparedness included knowing what to expect physically as the patient deteriorates and being prepared through knowledge of what pragmatic tasks would be required to enable a good death. For four of the participating families, their DD had a health background, which our previous research also indicated was common. 21 Three had a nursing background and one had unspecified medical training through their career in the military. Those with health backgrounds usually explained this to the families in the first meeting or consultation. These consultations explained DD services but were also a way for the DD to understand the families. In the cases where participating families had DDs with a health background, the difference seemed to be that they were more specific with the family members about what to expect from the dying trajectory and patient deterioration. None of the DDs administered medications.
Pragmatic aspects of preparedness were also highly valued. Families wanted to know the practicalities of what was possible, particularly for home deaths. However, sometimes they did not even know what questions to ask, but the DD would let them know what was possible in relation to what kind of death the family wanted within jurisdictional regulations and laws. Even for those who died in facilities, the pragmatic aspects of what happens after death were also highly valued (see Table 2).
Preparedness: Physical, practical and emotional.
DD, death doula; EoL, end-of-life.
Theme 2: Empowerment (subthemes knowledge and personhood)
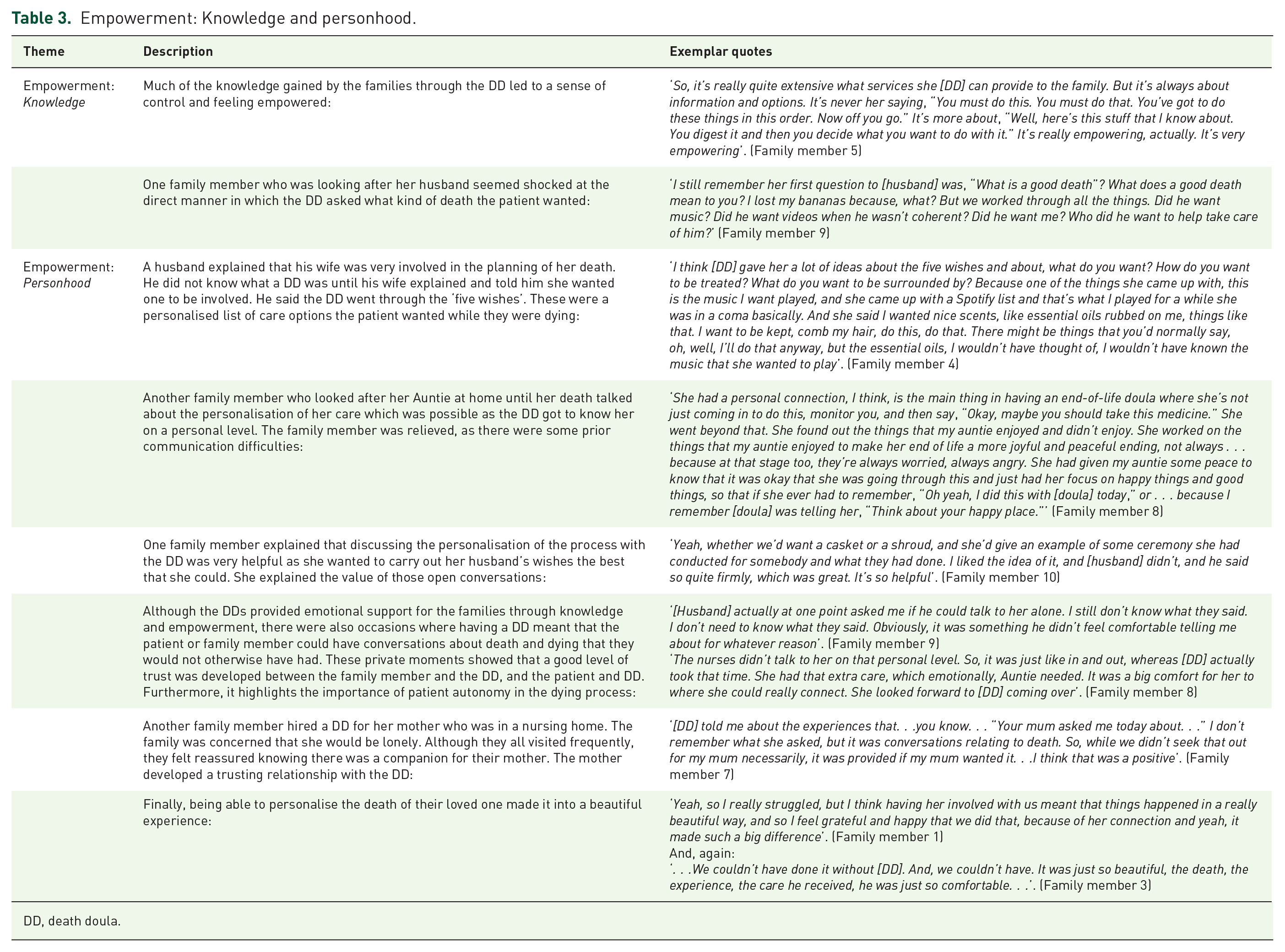
In confronting death, there is a sense of loss of control. 36 For families in this study, knowledge was power. The knowledge provided by the DDs provided a sense of empowerment and control over the events for patients, but more significantly for the family members. Good deaths were achieved from the perspective of the families and a sense of empowerment was found through the preservation of the personhood of the patient. Indeed, empowerment for these families did not just come from knowledge and being informed, but in the family member being able to ensure the EoL of their loved one was carried out in a personalised way (Table 3).
Empowerment: Knowledge and personhood.
DD, death doula.
Theme 3: Connection (Subthemes learning and sharing, paying it forward)
One of the most significant and novel findings from our research which could only have been garnered by speaking with families was the learnings that were shared between DDs and family members, and the depth of the connections that were made. In sharing openly about everything one needs to know about death and dying, the families felt that the experience left a resonant effect on their lives and a propensity to share that knowledge with others. In some cases, this led to helping other people at the EoL. Henceforth, although it is clear that DDs do not fit neatly into the compassionate communities’ paradigm,24,37 as bereaved members of the community, the eagerness of the interviewed family members to share and help others spreads compassion in the community around death and dying which we feel fits into the concept of ‘pay it forward’.
Many of the families in this study kept in touch with their DD after the death of their loved one. One family member said, ‘It’s hard for me to draw a line because I formed a relationship with her, and we still go out for coffee once a month’. One husband, whose wife engaged a DD for her EoL care, still keeps in touch with the DD and still feels emotionally supported. They go out for lunch, and she shares support group information with him, and they speak on the phone. We asked if that means they are now friends, he said; ‘Exactly, yes’ (see Table 4).
Connection: Learning and sharing, paying it forward.

DD, death doula; EoL, end-of-life.
Discussion
DDs suggest that their role is for the benefit of both client and family, but there is an agreement that it is client centred (patient centred) first, to advocate for the wishes of the person who is dying.1,10 Death is not solely about the person who is dying. There are complexities and nuances around who is involved or affected, and therefore there are implications in designing any systems or models of care around individual needs.
In our previous research on the DD role, we have elicited the views of DDs themselves with positive aspects of the role and its benefits highlighted. In this study, we have described the experiences of families who have engaged a DD to assist in EoL care. In agreement with other research on the topic, the utility of DD’s echoes other studies regarding their services and work structure.1,10,14 However, in this research, we were able to identify what values and benefits the families themselves experienced by engaging a DD. We discovered that variation in their services was not only influenced by family needs but determined by the stage of the trajectory that the patient was in when they were hired. In some cases, the DD had no patient contact at all; instead, the DD served to empower the family member to deliver the best EoL care.
What was surprising was that the relationships formed in the process of engaging a DD had a lasting, resonant effect. Two family members knew the DD personally before engaging them in the role (one as a massage therapist and one as a neighbour) however despite this, some of the others went on to develop strong bonds and even friendships with the DD. The connection made between families and DDs and the knowledge gained by the families led to them being eager not just to recommend DDs to others, but to share their newfound knowledge around death and dying with others and in some cases, being compelled to help others going through the same experience. In this respect, DDs are contributing to the perpetuation of compassion in the community through an increase in death literacy and the concept of ‘paying it forward’. This, in turn, is potentially contributing to a reshaping of the death system and enabling family members to become more compassionate community members. There was a decided connection between death literacy, empowerment and emotions, resulting in an increase in positive emotions while reflecting on their experience.
Preparedness (physical, practical and emotional) was found to be important for participants. However, preparedness for the patient and the family members differs. For example, a consequence of patient preparedness for pending death can manifest in having an EoL plan that allows for patient autonomy until death. 35 For family members, general unpreparedness when undertaking the challenging role of caring for someone at the EoL compounds the levels of stress and anxiety that they experience.38,39 Pragmatic aspects of being prepared were also highly valued. A recent study showed a categorical link between pragmatism and comfort; completing tasks that follow the wishes of the loved one has a two-pronged value. 40 In terms of knowing what to expect from the dying process, the DDs helped the families feel prepared for what physical transitions their loved ones would go through, especially if the DD had a health background.
The reason for the apparent rise in engaging DDs then cannot be viewed as simply filling gaps in the health system. The fact that families in our study still hired DDs when they had service provision means that their utility and value are much more complex. Perhaps some families engage in a DD not because they are necessarily incapable of providing care but because they require the extra support mechanisms (advice, guidance) that DDs provide for them in addition to community care services or hospices that are only able to provide fragmented care. Some of the DDs were also on-call or available around the clock. Roles such as navigators, Indigenous support workers, pastoral care services and compassionate communities may provide similar support, as opposed to physical care tasks, recognising as our study does, that the needs of family members are often related to a lack of awareness and self-confidence. As previously stated, health and social support for EoL care, even when available, is likely to be inadequate and not necessarily offered to families, leaving it at the behest of families to request it. 38
The knowledge provided by the DDs provided a sense of empowerment and control over the events for patients, but more significantly for the family members. The process of dying and meaning-making in death are sociocultural; death embodies a permanent loss of personhood. 41 In many respects, personhood is the preservation of autonomy. When it comes to EoL care, an empowered person is an autonomous person. 42 Personal preservation permeated these stories, particularly for the home deaths. Personal preservation is couched in liberal ideas of individuality and rights as an ethics of care. 43 According to individualism and identity, to die well is to die in accordance with ‘my’ personal way of living, joyfully, beautifully, autonomously. 44 Indeed, beauty was mentioned now and again to describe the EoL that these families managed to arrange for their loved ones. The families in our study felt that the experience of engaging and working with a DD resonated so much with them, that they, in turn, went on to share that knowledge with others.
In our previous research, DDs claimed the most important aspects of their role were to reduce fear and anxiety around death, empower families, educate and inform and provide emotional and spiritual support. 14 These aspects of their role were all echoed by the families in this study. The differences in emphasis in what families valued about DDs depended on the context of the situation, and their individual needs and wishes. Although previous research shows that what DDs provide depends on family needs and the DDs background, 19 a more accurate observation would be, as another study has found, that this depends on the timing of when the DD is hired. 17 For example, if a DD is engaged during the early stages of the dying trajectory, their role becomes more personalised to the patient’s wishes around their death, whereas when they are hired much later, or in cases where the family just needs advice and support, then it is more about support for the carer.
What is particularly interesting to note regarding our recruitment process and in obtaining willing participants for our study was that all the experiences that we documented were overwhelmingly positive, with no participants describing a negative experience using a DD. However, it is worth noting that one channel of enquiry of potential participants informed us that they did know of a family member who had used a DD, but that their experience was very traumatic, so it was unethical to reach out to them. Henceforth, no participants in our study could explicitly describe any drawbacks of using a DD. However, potential drawbacks or complicating factors of this movement can still be inferred from the data. Henceforth, the issue remains around potential conflicts with staff, how to regulate the industry and end-user protection. The question of potential conflicts between DDs and other healthcare staff could not be answered here as no overt conflicts were reported by the participating families. In two cases, however, families reported that they sensed an aloofness between the hospice nurse and the DD which for one person was simply referred to as a ‘vibe’. As such, although potential conflict may be possible, for these families, there was no evidence of this.
The issue of payment of DDs may also be a source of contention. Indeed, some people may not be able to afford additional services in the care of their loved ones. However, all families in this study stated that it was affordable and well worth it although four family members engaged a DD who did not charge a fee. Many believed that the benefit outweighed the financial cost and many also stated that they would not have been able to provide, either practically or emotionally, the level of care they did had they not engaged the DD. Finally, there still remains the issue of lack of regulation and protection for families who may have a negative experience. Further research needs to consider what recourse families have in these circumstances and how this could be managed through regulation.
Based on our findings, the most positive benefit of using a DD appeared to be the sharing of knowledge with a decided link between death literacy, empowerment and positive emotions. Evidence suggests that a sense of preparedness does not just provide a sense of support for families, it leads to better post-bereavement outcomes. 45 Through this, families not only felt they had the means to cope with the death of a loved one but were able to provide the best death possible, a personalised death.
The growing engagement with DDs for EoL care indicates an increase in families not only having control over the dying process, but in making deaths more personalised, taking suffering and death and making it more meaningful. 46 Having control over the manner of one’s death reflects that liberal individualism around death. The death of their loved ones was in many respects transformed into something they could reflect on positively; and in some cases, even describing it as beautiful. To note is that the perception of a ‘good’ or here ‘beautiful’ death is in the eye of the participant, acknowledging that there is no single definition that exactly describes that experience. 47
Some have argued that DDs are operating as ‘vanguards and ideological change agents’ who challenge the biomedical framing of death as a medical event. 19 Our view is that this approach to death and dying shifted long before DDs became popular. There is no supply of service without the need, and the increase in the number of people looking after their family members at EoL not only gives rise to a need for practical support, but emotional support. Indeed, death is relational, and families are diverse. The families in our study emphasised the emotional relief they experienced through engaging a DD. We agree with Broom and Kirby who argue that family involvement in death is an avenue that reflects the changing cultural ideas around the responsibility of care for the dying. 48 DDs are starting to be recognised perhaps because there is a gap not just in terms of capacity but in the type of needs that should be met by healthcare systems and the needs of living as you are dying. Public health, aged care, acute care, primary care and families and relationships must work together to seamlessly support those who are dying and their families. 49 This also speaks to the difference between care as a technical provision and care and caring in the familial context.
Interestingly, two participants (6, 7) alluded to their DDs working with the dying person who was in an aged care facility (nursing home), which we have found in a previous study, 23 and which could be an important step towards supporting those who are dying in facilities or perhaps in supported accommodation. 50 To also consider is that there are more people with no local family, friends or social networks (some of whom are in aged care facilities) and a DD can provide services that ensure nobody dies alone. 2
Perhaps one key commonality within DD service provision along with their heterogeneity is their agreement that their role is strictly non-medical.8,10,15 However, this is complicated by the fact that DDs can have a background in health, which must continue to be recognised as a potential point of contention not just with role blurring, but with family expectations. It should be noted that one DD provided advice on the timing of providing morphine and as someone with 30 years of hospice experiences this would have come naturally to them. While this DD did not administer the medication themselves, they were providing advice to the family member about medical issues, a fine line undoubtedly for many DDs with a medical or nursing background. 14
While our participants had overwhelmingly positive reports on the experience of engaging a DD, it needs to be acknowledged that most family members do not know what they do not know, and are grateful for any advice, support and guidance provided, but lack awareness of what else is available or what another DD can offer. It also should be noted that if a DD does not have a health background, then they are unlikely to have the same level of knowledge and experience in dying and what this entails, and consumers will be unaware if they are receiving accurate advice. This all speaks to a lack of standardised education programmes and mechanisms for registration that allow those with no experience (perhaps save for caring for their own family member) and/or a weekend DD course in setting up a business.
A broader conversation is required that includes death literacy, compassionate communities and bereavement care, with tensions between personal responsibilities, community functioning and formal systems. Where do these responsibilities lie within changing societal dynamics?
Strengths, limitations and future directions
The present study has generated valuable new knowledge about the lived experiences of families who engage in the services of DDs in Australia and the United States and is the first study of its kind to interview family members about the DD experience. Nonetheless, the findings should be considered within the context of its limitations. Our study, while providing unique and important data that have meaning, does have a lack of certainty about the potential for generalisability.
Recruitment was prolonged and problematic and conducted in phases as we extended our reach to capture potential participants. This may have led to a self-selection bias in only people with positive DD experiences agreeing to be interviewed, some having been recruited by the DD that they engaged. It is possible that family members who had a negative experience would have been less likely to feel comfortable talking about that experience, and they were also probably less likely to have seen the calls for study participants via the avenues we had available for participant recruitment.
For one participant, considerable time had lapsed since their DD experience, which may have resulted in recall bias with many details fading over time. Our initial thoughts for the bereaved family member to have distance from the dying experience and the DD were confounded by the fact that many participants were still in contact with the DD and considered them a positive influence and even friend, again a possible confounding factor. The experiences of using DD services may also be different in other countries with different health service provision models.
To gather richer information about the experiences of families engaging in DD services that can better account for recall and self-selection biases, future research needs to longitudinally follow families over time, recruiting them at the start of their DD consumer journey and learning how their experience unfolds. As the prevalence of DD services increases, this will be an important direction for future research to address.
Conclusion
For families in this study, DDs enabled the family member to be prepared for death which led to a sense of empowerment. This, in turn, made them feel emotionally supported and enabled the family member to provide personalised deaths and funerals for their loved ones. The increase in death literacy they gained from engaging in a DD left a resonant effect, whereby the families became more open to discussing death and sharing their knowledge with others. This has the potential to lead to an increase in community awareness and openness to engage with the fundamentals of death and dying.