
Abstract
Background:
Resilience is an increasingly used term in medicine and subject to various definitions, often not easy to grasp. There are established core concepts for patients receiving palliative care, for example, meaning in life, that have already been researched a lot. Resilience, relative to these concepts, is a new object of research in palliative care, where it has so far been used predominantly with regard to the well-being of teams.
Aim:
To explore how experts in palliative care define the concept of resilience and its suitability for patients, significant others, and professionals.
Design:
Qualitative study using summarizing content analysis according to Mayring.
Setting/participants:
Twenty-one health and social care professionals with expertise caring for persons with life-threatening/limiting illnesses and their relatives were interviewed in three individual interviews and four focus groups. All conversations were recorded, transcribed, coded via MAXQDA, and validated by another researcher.
Results:
Resilience has been described as something procedural, dynamic, individual, and flexible. In connection with well-known concepts such as posttraumatic growth or terms from the field of mindfulness, social environment or personal factors have also been linked to resilience. Resources such as spirituality can contribute to resilience, and resilience itself can function as a resource, for example, by contributing to quality of life. An active use of the term in practical work with patients or relatives is rare, but it is used in education or team measures. Limited lifespan can pose a challenge to an active use of the concept of resilience.
Conclusion:
Resilience as a very individual approach provides added value to other core concepts of palliative care. Within the palliative context, the normative dimension of resilience must be well reflected. A broader definition of resilience is recommended, leaving room for everyone to find their own form of resilience. The concept of resilience in palliative care includes opportunities as well as risks and should, therefore, be implemented carefully, requiring specific training.
Plain language summary
Background
Resilience is an increasingly used term in medicine. In the context of psychological well-being, resilience, along with social support and spirituality, was identified as a significant variable at the end of life. 1 In addition, as a term that always resonates in existential crises, it has become even more prominent in times of the COVID-19 pandemic.2,3 Both in the context of pandemic research and in general scientific usage, it is noticeable that resilience in the medical context is predominantly used with regard to the well-being of teams,4–6 but less with regard to patients and relatives. The recommendations ‘on how to build and maintain resilience of frontline healthcare professionals exposed to COVID-19 outbreak working conditions’ 7 are just one example of the boost given to the concept of resilience by the pandemic. The ongoing challenge to find a universal definition of resilience 8 and the fact that it is not easy to grasp make it possible to speak of a real ‘mystery of the resilience concept’. 9 For example, resilience is defined as ‘a construct connoting the maintenance of positive adaptation by individuals despite experiences of significant adversity’, 10 as a process of utilizing resources 11 or as a dynamic concept. 12
Palliative care is defined as ‘the active holistic care of individuals across all ages with serious health-related suffering due to severe illness and especially of those near the end of life’. 13 Palliative care may be required from the diagnosis of a threatening illness to the end of life, which in turn means taking different phases of life into account and poses a particular challenge for defining resilience. In material science, resilience is understood as the ability to bounce back, resuming the original shape after deformation. Transferred to psychology and medicine, this would mean coming out of the crisis unchanged. However, this seems – at least – impossible in palliative care, as the ongoing progression of the underlying disease does not allow for restitution of health or physical integrity, and coping with life-threatening illness requires psychological adaptation. This idea of development and human adaptive performance also underlies the psychological understanding of resilience. 14 Such processes of change can also be found in the concept of posttraumatic growth. Similar to the concept of resilience, descriptions of posttraumatic growth vary 15 and can be summarized as a ‘tendency to perceive benefits from trauma’. 16 A recent concept analysis identified similarities between resilience and posttraumatic growth. In addition to coping and thriving, both concepts were defined as ‘processes that result in internal changes for an individual with an antecedent of trauma or adversity/stress’. 17 Thus, an understanding of resilience that takes into account various parameters and focuses on the idea of elasticity and deformation instead of a rigid bouncing back is more fitting for medicine. Such a description can also be found in material science, where resilience is described as ‘a complex stress-strain-time property’. 18 It has been observed that resilience in a curative context can take on ‘a problematic, even toxic, dynamic and [can be] counter-productive to maintaining or enhancing the participant’s quality of life’ 19 because the only focus is on healing.
Resilience is described both as a term and as a concept, 20 but it seems obvious that describing resilience only as a fixed term falls short in the discourse. A recent systematic review found that a psychological concept of resilience often dominates in palliative care. 21 For the field of palliative care, there are already a number of core concepts, including quality of life, sense of coherence (SOC), dignity, meaning in life, autonomy, and an abundance of spiritual dimensions. In order to be able to continue to sharpen the concept of resilience, it seems necessary to clarify which concepts are associated with resilience, explore their relationship, and to identify overlaps and differences. The literature has already pointed to a growing scientific as well as societal interest and a related desideratum of interdisciplinary resilience research. 22
Our aim is to analyze whether the concept of resilience is useful for palliative care or not. For this purpose, we posed the following research questions: (A) How do experts interviewed define the term resilience? (B) How do experts interviewed use the term in their everyday, practical work? (C) Does the use of the concept of resilience create added value to palliative care? (D) Are there any risks in using the concept of resilience in the context of palliative care? (E) What components of resilience can be found that contribute to the necessary operationalization of the term? (F) What is the significance of the concept of resources for the resilience concept?
Methods
Design and sample
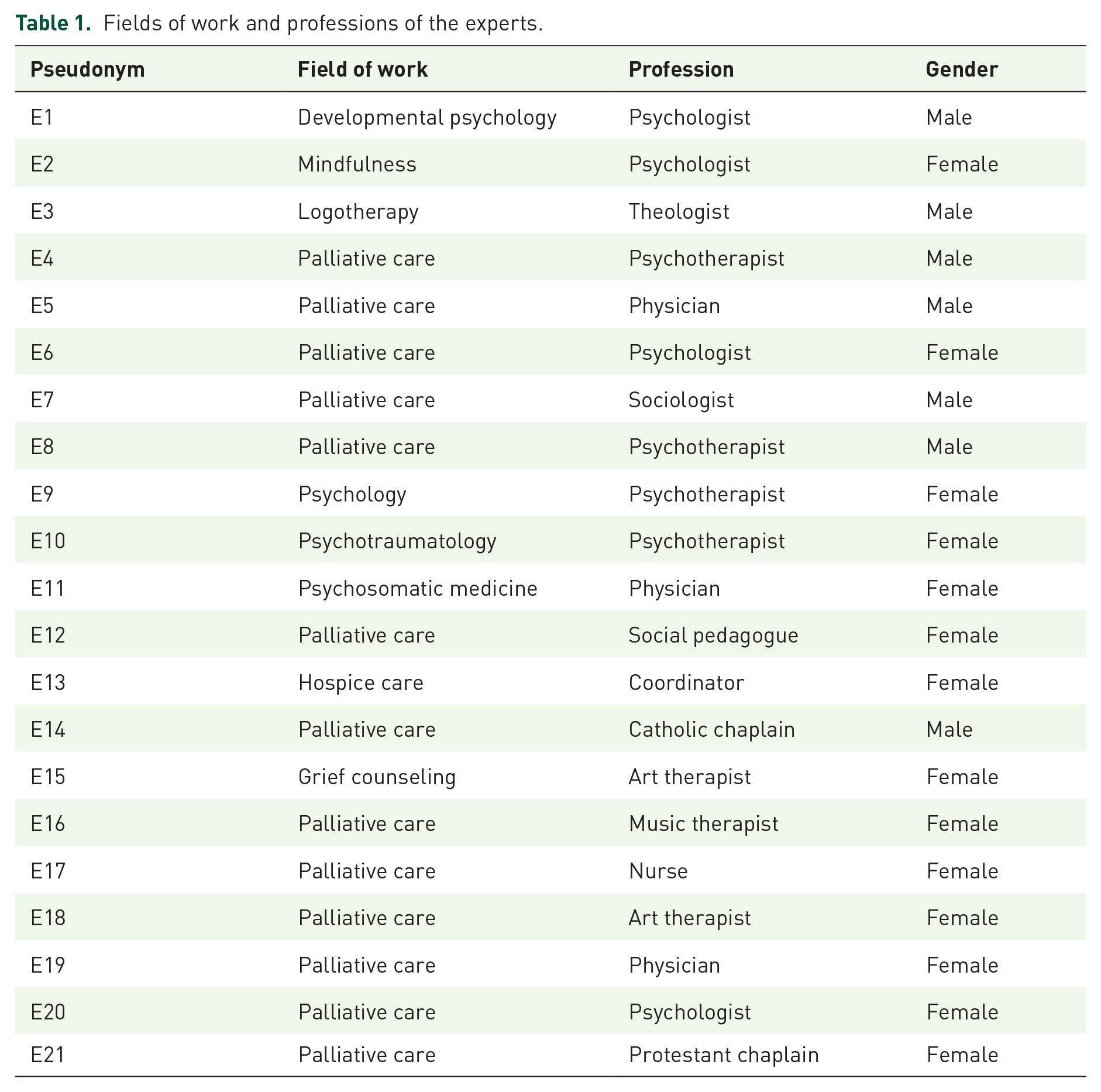
For this study, our work package ‘Resilience and Coherence in Palliative Medicine’ is part of a larger interdisciplinary research group funded by German Research Foundation (Deutsche Forschungsgemeinschaft; DFG), including theology, philosophy, spiritual care, psychosomatic medicine, and palliative medicine (https://www.etf.uni-bonn.de/de/fakultaet/drittmittelprojekte/dfg-for-2686-resilienz-in-religion-und-spiritualitaet). To evaluate the perspectives of experts from within the field of palliative care as well as from related disciplines, a total of 21 experts (14 female, 7 male) participated in the study. Four persons refused to participate due to lack of time or scheduling conflicts. The sample was selected purposively. Data saturation was reached when topics were repeated and no significant new themes emerged from the interviews. Different professions with expertise in psychology, psychotherapy, sociology, medicine, theology, grief counseling, or other fields were represented. In order to be able to take closely related disciplines into account, eight experts were included who do not work primarily or only partially in palliative care but provided important contributions from the fields of (developmental) psychology, mindfulness, logotherapy, psychotraumatology, psychosomatic medicine, hospice care, and grief counseling. The results of this paper will be used for contrast in subsequent surveys.
Initial interviews
First, three semistructured, qualitative interviews with one expert (E) each in developmental psychology, mindfulness, and logotherapy, as three disciplines highly relevant to resilience research, were conducted in May and June 2020 by one researcher (KM). Due to the COVID-19 pandemic, interviews took place via telephone or video call. An interview guideline was developed by the research team based on a previous research project using discourse analysis from our workgroup. 23 The interview guideline was pilot tested three times with staff from the fields of psychology and humanities. The final version included around 20 open-ended questions in four thematic blocks:
General understanding of resilience (personal definition; synonyms; learnability; measurability)
Associations of resilience with other terms and concepts of interest (spirituality; religion; hope; optimism; SOC; quality of life; meaning in life; autonomy)
Particular expertise (connection of the terms and concepts of interest and specific interventions in their fields of work)
Assessment of the relevance of these terms and concepts in everyday work practice (patients, relatives, staff).
Focus groups
Four focus groups were organized with 3, 4, 5, and 6 professionals, respectively, for a total of 18 experts between October 2021 and May 2022. Focus groups took place via video conference by two researchers (KM together with FP or GA). The findings from the expert interviews were used for the development of the interview guideline for the focus groups. All groups were given the same questions, which were shown during the discussion via PowerPoint presentation. Each group started with a short round of introductions of the participants, followed by an introduction of the project. The first question in the round was about the personal definition of the term ‘resilience’ and potential synonyms for it. After that, a picture (https://karrierebibel.de/resilienz/) was inserted showing a human, equipped with a cape and a sword, in a fighting position and a very tense facial expression. Several words (life crises, setbacks, separations, conflicts, losses, and suffering) pelt his shield in the form of arrows and bounce back from it. Participants were asked to share their associations with this image of resilience. However, because this image of resilience embodies a very specific view of resilience, it was explained in advance in each group that it was consciously selected to be provocative. Subsequently, they were asked if and when the concept of resilience in the field of hospice and palliative care can be beneficial and when it can be harmful, and this question was repeated for each of the three target groups (patients, relatives, and staff). Finally, participants were asked to evaluate whether the concept of resilience is suitable within palliative care and whether they feel that they would use it more often following the focus group in their daily work. Field notes were documented after each interview and focus group, reflecting on the courses of conversation.
Data analysis
All interviews and focus groups were audiotaped, transcribed verbatim, and analyzed via summarizing qualitative content analysis according to Mayring and using the software MAXQDA2020 as well as MAXQDA2022 (VERBI Software). One researcher (KM) carefully reviewed the interview material and coded it inductively. Mayring’s technique of Summarizing is characterized by analytical steps of paraphrasing and reduction. 24 This approach is very useful for researching extensive concepts and terms as it allows ‘to reduce a large volume of material to a manageable level, but in so doing retaining the essential content’. 25 Validation was performed by a researcher from another discipline (MKR or JKM) involved in the research group but not in the direct data collection. This researcher looked at the coded interviews and marked places with disagreement or where codes were missing. The researchers discussed the codes until agreement on the final code tree was reached. The codes were then grouped in categories by the first researcher (KM).
Trustworthiness
Quality criteria are highly debated in qualitative research. One suggestion comes from Lincoln and Guba, who propose credibility, transferability, dependability, and confirmability. 26 Credibility includes the piloting of the interview guideline(s), the design of the interviews as well as the professional and methodological expertise of the research team. The purposive sampling resulted in the availability of a high level of knowledge and the representation of different professional groups within palliative care and closely related disciplines. This ensures transferability to similar populations and research contexts. With regard to the dependability of the study, its methods were described and documented in detail. This study followed the Consolidated criteria for reporting qualitative research (COREQ) with a 32-item checklist for interviews and focus groups 27 (Supplemental Materials). To ensure confirmability, various methods were used against the background of triangulation – both in terms of the methods themselves and the researchers involved in collecting and analyzing the data. Regular exchanges and the preparation of memos during the validation process helped to generate reflexivity among the researchers. In addition, two participants read their transcripts and gave feedback on the results.
Results
The data analysis resulted in eight main categories: understanding of resilience, resilience as a process, resources for resilience, resilience as a resource, time dimension, practical use, opportunities, and risks. Table 1 shows the professions interviewed and enables attribution of the following quotes, which were generated from both the individual interviews (E1–E3) and the focus groups (E4–E21). The individual interviews were 48, 58, and 128 min in duration [mean = 78 min, standard deviation (SD) = 43.6 min]. The mean duration of the focus groups (96, 84, 92, 96 min) was 92 min; SD = 5.7 min.
Fields of work and professions of the experts.
Understanding of resilience
Various definitions and descriptions of the term resilience can be identified (research question A). Descriptions of resilience ranged from ‘a strength or a will to face even what is unpleasant’ (E9) to ‘having a certain inner wealth that I can fall back on, especially in crisis situations’ (E4), ‘a cooling system that simply carries me through stressful, really hot times’ (E8), ‘a framework in which things happen and are important’ (E4), ‘to be able to recover again in a short time after stresses and strains’ (E14), or that a person still ‘feels a bit grounded’ (E4). Resilience was also described as ‘a bouquet of quite, quite many techniques, offers’ (E9), going hand in hand with the aspect of individuality. The most used word was capability of resistance; however, it was emphasized that ‘resilience is much more complex than just this’ (E3). The way one deals with life’s crises or challenges also played a role. This includes ‘inner qualities and experiences already made’ (E2) as well as what is perceived as helpful in dealing with stressful situations. So another explanation was that ‘resilience consists of various partial abilities that make a person resilient’ (E1). This in turn goes hand in hand with the issue of protective and risk factors. Additionally, there was a view that ‘you can be anywhere on a continuum from not at all resilient to very resilient’ (E1), which means that resilience is not either or. Other terms that came up when asked for paraphrases of resilience were: (inner) strength, self-efficacy, self-awareness, self-assurance, self-esteem, emotional regulation, endurance, openness, courage, engagement, acceptance, fighting, the opposite of vulnerability, pliability, elasticity, flexibility, stability, not to break, dealing with crises, renitency, coping, serenity, growth, crisis as an opportunity, a high degree of adaptability, anxiety reduction, social skills, resources, and cultural values. Resilience could be associated with an aspect of avoidance, trying to get away from something unpleasant or difficult as quickly as possible. This broad spectrum of terms shows why the unclear and broad definition of resilience was perceived as ‘so vague that it can be everything and nothing somehow’ (E9).
However, there were also clear ideas about how resilience should not be understood. For example, that one remains able to resist everything and that nothing can knock you down ‘because something has knocked this patient over, otherwise they would not be in hospital’ (E11). This was particularly reflected in the evaluation of the image shown in the focus groups. The relevant opinion was that the image of a ‘superhero who is able to build up a protective shield against everything’ (E7) was inappropriate to represent resilience and very normative. There was also criticism of the rebounding arrows. For a more appropriate representation of resilience, experts pleaded that the arrows should have hit the person (‘that is actually not my image of resilience, that the arrows do not arrive at all’, E20). Also the sword symbolized the aspect of fighting back inadequately (‘You might not need a sword, a little bit of sword is good but maybe not like that’, E19). Missing in this picture, as reported by the experts, was the idea that crises can also mean an opportunity and the possibility of growth. Experts also criticized the missing representation of feeling. The picture title, describing resilience as the ‘immune system of the soul’, was assessed as ‘quite good, because our immune system can’t ward off everything, it is also permeable in some places’ (E17). However, experts lacked the depiction of social factors (‘the immune system of the soul would also be that I still have an environment that I am not alone there, but I would like to put a few people around it’, E13). In summary, the image was perceived as too aggressive and threatening (‘that’s the surest way to smash resilience, if I carry on doggedly’, E14).
Resilience as a process
A procedural nature was highlighted by describing resilience as ‘a development and a process, not a snapshot’ (E13). As an important component, processuality thus contributes to the necessary operationalization of the term resilience and is, therefore, an answer to research question E. This description of resilience as a process was used in two ways: First, resilience was described as something dynamic in dealing with crises (‘one does not remain constantly motivated to change but also always swings back and forth a bit’, E9). This was accompanied by flexibility, as resilience was not seen as something rigid in the sense of its word origin of ‘springing back’ to its original state as well as the idea of ‘an elastic handling of stresses and I will not be dented permanently’ (E14) or elasticity in a sense of ‘that one can return again, even after a jarring setback’ (E7).
Second, responses concerned the learnability of resilience, which went hand in hand with adaptation and learning processes (‘If I adjust myself to it, I can also develop my resilience as a process of my personal development, also strengthen it as I go along’, E5). Self-reflection was mentioned as relevant for developing resilience (‘If I am very reflective, I can also learn something, then I see what is good for me and what is not’, E18). Resilience was rated as acquirable and as ‘something you get in your life and don’t generally have in yourself. It’s definitely not an inner quality. You can certainly strengthen it consciously later, or not, but first it’s something like a gift (. . .) also a gift from the environment’ (E12). One expert described resilience as a ‘potential’, reflected on how a person could make the most of it, and also found the answer in something moving and processual (‘I am constantly moving in this process of exploiting my resilience’, E3). In addition, recourse to the lived experience of how previous crises have been overcome (‘then of course I activate these problem-solving strategies and these competences and can then consider in the next step how I can apply them today’, E1) and ‘to value your own history’ (E11) were seen as important.
Resources for resilience
To answer research question F: Although there was one view of the resilience and resource concepts as competing (‘For me, resilience is once again a competitor for the topic of resources, because I am tired of the inflationary use of “resource” (. . .) another concept than just saying resource to everything’, E10), the topic of resources was very prominent in the interviews. The question about the personal definition of resilience was answered with ‘in critical or difficult situations to know what we need right now to get through it in the best possible way’ (E15) or ‘to say in difficult crises: Where can I get such a protective spell for myself with a thought of something wonderful?’ (E5) and it was mentioned that ‘it can definitely be different things that make a person resilient’ (E1). Thus, some resources that contribute to developing resilience could be identified.
First, the social environment was addressed as an important resource for promoting resilience. According to this, a resilient person was not characterized by ‘coping alone, but that there is also a network of assistance’ (E9), which included both private environment and professionals. Resilience was also mentioned as a structural component in the context of social embeddedness, what ‘shows itself above all in social interaction (. . .) how I react to a context myself, take a stance on it’ (E5). The statement that ‘resilience only arises out of life crises and by being supported in a network’ (E13) is also consistent with this and addresses the idea of growth as well as growing resilience from life experience simultaneously. Because it was recognizable that when personal factors were addressed in terms of inner qualities or experiences, the number and intensity of crises already experienced also played a role, according to the idea that resilience ‘also relates to life experience: How did I get through crises before?’ (E17).
‘The option of acceptance, simply accepting things that are there, learning to deal with strokes of fate’ (E8) was considered beneficial ‘while resisting and fighting against the crisis situation would weaken resilience’ (E2). Acceptance was closely connected with the concept of allowing, ‘an openness, courage and an acceptance that certain things are allowed to be there’ (E9). Such an acceptance ‘cannot be demanded but can be encouraged. That someone accepts that an end is imminent’ (E3). This included allowing negative feelings, crying, screaming, or anger because ‘people with resilience can also be quite vulnerable’ (E4). ‘Letting something that comes from the outside affect me and seeing how I learn to deal with it mindfully’ (E8) was connected with the concept of letting go as ‘no longer rearing up and fighting and wanting to settle everything, but simply accepting things or taking a step back or saying: “Wow, I’m giving up this fight right now. I don’t have to be strong and function right now”’ (E10). But acceptance was also clearly separated from the concept of enduring, which has a negative connotation, when endurance is accompanied by a combative attitude and ‘can also have a fatalistic nuance in the sense of “o.k. I have to endure this now”’ (E2). In a crisis, it is more about ‘perhaps first of all enduring the fact that I can’t yet experience what’s happening here as meaningful’ (E6). This went along with an ‘inner attitude we practice with mindfulness, namely kindness, friendly interest, openness’ (E2) or the – also fitting to openness – definition of spirituality from a theological perspective: ‘For me, spirituality would start here (. . .) where I am able to open up and then maintain this perspective and eventually also this openness for the whole picture’ (E3). Other concepts related to acceptance were observing (‘Now there comes the difficult feeling, the difficult experience, the difficult thought together with body sensations and so on. And I can observe that (. . .) which in turn promotes composure, reduces anxiety’, E2), curiosity named as ‘having the courage to look, in quotes, “where it hurts”’ (E9), but also in contrast not-knowing (‘we deal with the fact that in the end we don’t know (. . .) and with this we develop a strong resilience factor. Because we as humans are simply also limited and can not understand a lot of things’, E2).
The statement ‘When you are cared for in hospital, the focus is always on what is not working, what is sick, what is broken, what can be improved somehow, and what is often forgotten is what is also working’ (E16) embodies the basic idea of the salutogenesis concept. From the salutogenic thought, in turn, emerges the concept of SOC, whose three elements could all be found in the interviews: comprehensibility as ‘accepting, embracing, and understanding the contexts in which we live’ (E2). Manageability in the sense of ‘still remain capable of acting to a certain extent in order to be able to care for oneself and others’ (E14). ‘That it provides a goal or a framework and thus perhaps also a meaning. That I know again what I am actually doing this for?’ (E9) addresses meaningfulness as third component of SOC.
From a logotherapeutic point of view and with reference to Frankl, the meaning of freedom to choose was added: ‘that I constantly have a bit of power to choose and can possibly make the most of every situation (. . .) then I am also more resilient as a result and always learn something new’ (E3). ‘Not allowing oneself to be intimidated’ (E1) was representative of autonomy as a further, important resource for resilience. Reassessment as an aspect of change (‘factors that have already once led to coping with certain things, and so perhaps also to make a reassessment’, E10) referred to hope and optimism as relevant components of resilience. Hope was predominantly associated as ‘the motor for change or for action’ (E2) and as ‘the perseverance that I can still shape, still change something’ (E3), while optimism was defined as ‘that I have an idea of something good, that it can turn out for the better’ (E2) as well as ‘less active, but rather a passive waiting that a miracle happens’ (E3). Trust was also relevant, but it is important to distinguish which trust was spoken of – for example, trust in God or trust in oneself, that ‘trust then also always has an object’ (E2).
Faith in sense of ‘belief in providence. But providence not in this fatalistic sense’ (E3) was addressed as ‘a source of strength that helps me in a particularly difficult situation or phase to then keep up my social self which I wouldn’t be able to without’ (E5). Also, spirituality as ‘the feeling to be carried by something greater’ (E2) was assessed as a potentially strengthening resource. More specific ‘some people call it a spiritual activity when they walk in the forest and think about the trees and nature and that also leads to transcendent thought processes’, although spirituality is not a competency as much as self-efficacy’ (E1).
All of this applied both to patients themselves and to their environment such as family members, who ‘then actually somehow are resilient, if they can also fall back on personal or social resources, which help them to cope with the illness of the patient or to deal with the grief, so that they won’t suddenly commit suicide or something like that’ (E5). Support in revealing resources within a resilience process should be the task of the palliative care team and professionals should look carefully on which aspect the person being cared for is focused, because ‘resilience can also be understood as a moral requirement or as a claim on an individual’ (E7).
Resilience as a resource
Also referring to research question (F): Resilience itself could be seen as an important resource. When asked for synonyms for resilience, quality of life was a frequently mentioned term (‘resilience is also about not letting it impact one’s quality of life’, E6) and the experts had quality of life in the back of their minds as a concept in their work (‘quality of life is one of the important outcome variables of any psychotherapy’, E2). These descriptions showed the understanding of quality of life as an outcome and resilience as a resource to reach that outcome (‘resilience, I think, is a big key for quality of life and for me it’s also a little bit about this deepening feeling, inner richness, despite the external, sometimes adverse circumstances of life’, E6). This fits in with the understanding of resilience as a process in which partial aspects should be focused on (‘Better can also mean that the pain stays the same, but my quality of life gets better again. Or my mobility. Or my social contacts or whatever’, E11) and all of this ‘must also be adapted to some extent to the process, to the moment, to the goal’ (E11).
Time dimension
In response to research question E, another important component that should be considered showed up: at various points, the temporal aspect of resilience was named. Resilience meant not only to be quite stable in the short term, but also in the long term, to be able to maintain one’s own attitude’ (E5). There was no belief in a point in time when resilience no longer plays a role, but ‘that resilience will, at some point, open a different horizon. So that in palliative care, it relates to smaller entities and to smaller contexts (. . .) that it is also limited in time to the immediate future’ (E11). This is particularly relevant with regard to the challenge of a limited lifespan, what also meant ‘in the light of a very limited life expectancy you have to formulate the goal differently in order to be able to find resilience at all. At least for the patients, if the goal is travelling down a good path, whatever way that may be’ (E11). It would also be important to keep in mind that ‘every technique or every approach naturally entails an end in time (. . .) or even just for the moment and maybe five days later it works again, and we can continue with the approach’ (E9).
Practical use of resilience
This category relates to the research question of how the experts interviewed use the term in their everyday practical work (research question B). Resilience was mentioned by the experts as a topic in the education and training of healthcare professionals. In one institution, the concept of resilience was purposely integrated into the training of medical students and other healthcare professions. Experts wanted to integrate the term into the training of physicians and nurses (‘today it became clear to me again how different the term can be understood and I have to think about it again, whether this is a very good approach for the further training for the team’, E7). One person reported using it specifically in training courses in order ‘to illuminate it critically and not to associate it with a panacea or a silver bullet or anything else as an expectation’ (E4).
When asked to what extent the term is used practically in working, for example, with patients, clients, or significant others, the experts agreed that active use of the term is rare. Resilience as a concept was already present in the back of their minds, but the term has not yet been actively used, accompanied by concerns about not reaching people if terms are used hastily or incorrectly (‘I will rather use really simple paraphrases and try to find the respective appropriate term based on the individuality of the person I am dealing with’, E8). However, it was also pointed out that this is nothing new for the field of palliative care (‘we try to have a very family and patient-oriented language in which we really avoid medical terms quite deliberately and then rather paraphrase that with other words’, E5).
Opportunities of using resilience
Experts were appreciative of the concept of resilience and the opportunities it offers for patients and significant others (research question C). This was exemplified by the psychotraumatological perspective on resilience as ‘the power of resistance that a person has to cope with difficult things and severe crises and actually performs superhuman feats’ (E10). Resilience has also been linked to the potential ‘to show why people are different in crises and situations’ (E6). One expert assigned resilience ‘more to prevention than to therapy’ (E11). Overall, the experts agreed that resilience could be an opportunity in clinical care if it is seen as an offer, not an obligation, and this is clear communicated to all participants. Resilience should be understood as ‘a very individual approach, shaped to the individual (. . .) on very different levels’ (E5). It ‘can be an opportunity if the patient is involved, if they are taken seriously, on eye level and if the spoken word or wishes are also taken seriously (. . .) perhaps also involved with the closest family members’ (E15). So it became clear that resilience can only be used if the team is trained in its use. The concept of resilience was seen as useful for palliative care ‘if the counselor/other person can deal with it well’ (E12) and ‘if its normative dimension is also reflected’ (E7). A definition of resilience that is not too narrow would ‘perhaps leave more room for everyone to find their form of resilience’ (E11).
Resilience also comprises some strengths for staff: ‘How can I remain emotionally aware and responsive and experience the work as meaningful, experience the care as meaningful and thus also remain in the field for a long time without becoming numb, without no longer allowing myself to be affected, or the protective armour being so strong that nothing reaches me?’ (E6). Also in leading positions, people have to think about how to ‘control the distress in the team in a situation where people who are cared for are frequently dying and the team must be able to cope with this distress’ (E5). In this context, resilience was described as ‘a quality of someone who can cope well with their work tasks and does not fall ill under them’ (E11).
Risks of using resilience
Experts were concerned about risks in using the concept of resilience in the context of palliative care (research question D) if professionals use the term wrongly: ‘We have to be careful what our idea is, a paternalistic approach or duty of care’ (E5). This includes also using it misleadingly with the expectant and demanding call that ‘the patient has to be able to cope with the pain and that this is now the crisis that he has to overcome’ (E6). This is not only a risk in relation to symptom control, but also to cultural differences bereavement rituals. A dangerous understanding of resilience would also be that ‘the patient must be led to accept death’ (E18) or in general ‘if the team knows better what the patient needs’ (E15). Resilience should not be used with ‘the intention to improve or optimize something’ (E9).
Additionally, concerns were expressed that the word resilience might evoke unrealistic hopes in patients: ‘I find it difficult at the moment to talk to patients about resilience as such because it’s already a buzzword in many places that perhaps awakens a false expectation’ (E4). Resilience was seen as a problem for patients when it leads to pressure, when they think ‘that they as individuals just have to behave differently, then the situation they are in gets better. Although quite a lot of things don’t get better’ (E7). Thus, resilience ‘must be well undergirded to be not simply an empty phrase that is misunderstood and misinterpreted’ (E4). This also includes the risk of ‘imposing this therapeutic concept on the counterpart, even though they may not need it at all. That their resilience takes some other form than what I think it should be’ (E10). Value was placed on the preservation of individuality and the associated wording, because ‘quickly thrown in or quickly used terms jeopardize the chance to look at what is actually behind the question or behind the statement of poverty and needs’ (E4). It was also suggested that common synonyms and related terms be used in conversations with patients, significant others or staff to ‘translate the term, to make it less convoluted’ (E8). Caution is especially advised when using it in sensitive life situations, which are omnipresent in palliative care (‘If I were to start talking about meaningfulness or resilience with an acutely bereaved person, I think I would simply not be able to perceive the individual need at that moment’, E6). A risk was also seen when the concept of resilience is not sufficient explained, because it is ‘so much in the media and it is googled and then maybe it gets into such a false track again when patients check it’ (E9). There was a plea to consider the target groups of patients, significant others, and staff separately, because ‘what can be good for the family members, for example, may not be good at all for the patient’ (E7). Thus, in working with family members and significant others resilience should be considered from two sides: ‘On the one hand, how do you deal with the crisis for yourself? And then how do you deal with the crisis for the person who is ill and that you are about to lose?’ (E4).
For staff, the resilience concept was seen critically when personal limits are disregarded, ‘when it is assumed: “Gosh, they are resilient! We can increase the burden!” Then it is ultimately harmful’ (E19). Concerns were also expressed about the misuse of resilience to make people compatible with a system (‘If I’m not resilient enough, then I have to leave the field (. . .) So to simply deal with the system’s mistakes on a personal level would be fatal’, E6). Experts understood resilience of staff as a total sum: ‘If someone is fully burdened at home, or is currently going through a life crisis themselves, then from my point of view they cannot also deal with patients in a resilient way and do their full job, i.e. call up their full performance capacity’ (E15). There was the opinion that the word resilience ‘is in itself (. . .) a very valuable one, but through the popularisation and dissemination it has also acquired a connotation to the effect that you only have to train people enough, then you can burden them with the most strenuous tasks and work, then they can withstand it; withstand the bad working conditions. And that’s not what resilience should be’ (E4).
Discussion
In a medical context, resilience is often described as ‘the process of harnessing resources to sustain wellbeing in the face of adversity’. 11 Although this is a simple and conclusive definition of resilience, there are numerous other definitions. This observation was also reflected in the expert interviews reported in this study. The synonyms and paraphrases for the term resilience provided by the experts illustrated a broad spectrum of related terms and underlined the multidimensionality and complexity of the construct (research question A). It seems to be difficult to find unique and simple synonyms for resilience. The experts preferred complete sentences as paraphrases and synonyms were limited mostly to ‘capability of resistance’. Furthermore, resilience can be described as a character trait, an outcome, or a process.9,28,29 And even if resilience is understood as a process, there are still different ideas about this approach. The description as a trait is problematic if resilience is associated exclusively with positive characteristics. The philosophy of palliative care allows a positive evaluation of traits that have a negative connotation in society (such as anger or despair) but may be seen as strengths in a more differentiated resilience concept. It seems quite normal that palliative care patients in their disease trajectory experience ‘a roller coaster ride of ups and downs’ 30 and this was reflected in the discussions in the focus groups. Resilience was not simply understood as an ability to simply let the strokes of fate bounce off, but rather was attributed to sensibility and vulnerable elements. Vulnerability and resilience are not mutually exclusive. 31 An early study on protective factors in connection with the development of resilience already came to the conclusion that ‘protectiveness is not the obverse of vulnerability’. 32 In the interviews, resilience was described as a resource to improve palliative care outcome variables, such as quality of life. The literature reinforces this by arguing in various places that resilience ‘should be viewed as an interactive process, rather than an outcome’. 33 This highlights the added value that the concept of resilience offers for palliative care (research question C): Such an understanding of a procedural nature simultaneously excludes rigid concepts and implies that support of patients and significant others in a nonlinear disease trajectory should be based on equally nonlinear concepts. In a study examining survivors’ perceptions of hope, the majority of respondents defined hope as resilience, which in turn was defined as ‘strength or a (coping) strategy to endure adversity’. 34 Terminology originating from the field of mindfulness, such as openness, courage, or not-knowing, may provide important additions and applicable elements for resilience in (existential) crises with life-limiting diseases. These concepts all have in common that they allow for a degree of flexibility as an expression of discretionary power. This aligns with other descriptions in the interviews, such as ‘an inner wealth’, ‘a cooling system’, or ‘a framework’, all of which have a processual and modifiable character. It is precisely this flexibility that is needed be able to accept the adversities as part of one’s own biography, which goes hand in hand with the integration of negativity and powerlessness. 35 These descriptions also underline the complexity of resilience and add to the challenge of how to operationalize or measure resilience and its underlying terms and concepts. Individuality seems to play an important role in the understanding of resilience. Both for the definition of resilience (research question A) as well as for the practical use of the concept of resilience (research question B), respect and preservation of individuality were emphasized by the experts. It may not be possible to distinctly assess and measure resilience without losing the broad range of understanding of resilience for the individual patient. This principle of uncertainty is not unique for the palliative care setting, and has indeed been described as a problem for other scientific fields outside of medicine. 36 An interdisciplinary approach – which is core to palliative care anyhow 37 – may be beneficial to identify the best trade-off balance between operationalization and individuality.
One strength of resilience concepts was described as not being oriented toward deficits, but focus on ’the often hidden’ potentials and resources. 38 This resource perspective cannot succeed without considering the salutogenesis concept, where again highly procedural components are found. Thus resilience is understood as something that can be strengthened in the process of health maintenance in order to foster salutogenesis.39,40 This aspect was mentioned in the focus groups, where it was criticized that in clinical care, primarily the illness and the associated loss of function or other deficits are considered. The attribution of process-modeling and facilitating properties to resilience 41 supports the argument that resilience should be considered as an important resource for patients. However, experts described resilience not only as a resource in itself, but also discussed resources that can be helpful for the development of resilience, such as spirituality (research question F).
In addition to the focus on psychological issues, spiritual and religious themes are a substantial part of resilience-specific research.42–44 Spiritual care has been listed as one of the four major domains of palliative care, in addition to the physical, psychological, and social domains. However, in contrast to the other domains providing care for spiritual needs may be challenging for healthcare professionals. 45 More research is needed on the relationship of resilience and spiritual care and whether the resilience concept can be used to sharpen the understanding of spirituality in the context of palliative care. Recently, a study of hope perceptions of bereaved caregivers of oncohematological patients identified, along with expectation and desire, resilience as one of the three main functions of hope. 34 This points to an inverse relationship between spirituality and resilience, where spiritual components may be a resource for resilience, and resilience may be understood as a resource for spirituality.
In an interview study with lung cancer patients and informal caregivers, patients and caregivers highlighted the nurses’ role in salutogenic aspects. 46 In addition, the unmet needs, burden, and morbidity of family members of palliative care patients require attention from healthcare professionals, who often lack knowledge and tools for this task. 47 The concept of resilience could be used as such a tool. However, until now, resilience has been used predominantly in the context of reducing stress and increasing the well-being of (palliative care) teams41,48 and as an indicator of high quality healthcare. 49 The call for further resilience-specific research 50 should be pursued but needs to be expanded from resilience in professional caregivers to understanding and fostering resilience in patients and significant others. This includes the need to develop interventions aimed at achieving resilient coping styles among informal caregivers. 51 Promoting resilience in patients and informal caregivers requires much more than an awareness of one’s own resilience: namely, a deeper understanding of the term and knowledge of potential pitfalls and risks, but also the beneficial potential of resilience. This also fits in with the need already expressed ‘to require new models of training for multisector and multidisciplinary teams to advance the science and application of multisystem approaches to resilience’. 52 Resilience is already described as an umbrella term in other disciplines, 53 and this also applies to the context of palliative care. Resilience is not a panacea in palliative care but requires sensitive use, which addresses a major risk of using the concept of resilience (research question D). Sensitive use of resilience in palliative care also includes a time dimension, which – in addition to the processual character – in turn represents an important component for the necessary operationalization (research question E). Issues related to the concept of resilience – including spiritual issues – can arise at any point in the disease trajectory. 54 However, early on in the trajectory, patients might be more focused on resilience as resistance to change as they are struggling to overcome or at least slow down their illness. In patients near the end of life, resilience might prove to be elusive, as physical and cognitive impairments prevail. A resilience corridor between these two positions has to be identified, clarifying the time frame for the development of resilience interventions that are feasible and beneficial in palliative care.
Limitations of the study
The study included only the perspective of the healthcare experts. We are aware that it is important to include patients and significant others in our research, which we will do in subsequent surveys.
Conclusion
Resilience is not a self-explanatory term. Using the concept of resilience in palliative care practice is irrevocably fraught with risk because of a possibly incorrect use of the term – especially if it is used expectantly or demanding. Its use should be sensitive and targeted. It should always be seen as an offer and in no way be imposed on a person – whether on patient, significant others, or staff. Palliative care does not only refer to the end of life, but it also still involves working with patients who have a very limited lifespan. The concept of resilience could also be used here when it relates to smaller contexts, for example. Various resources for resilience have been identified, but resilience can also be a resource in itself. The nature of resilience, which is described as processual, flexible and dynamic, is convenient to a nonrigid understanding in palliative care.
Our findings highlight the diversity and usability of the concept of resilience in the context of palliative care and confirm that its increasing attention in the scientific community is justified and that it should be adopted as an important concept in palliative care. Resilience as a very individual approach provides added value to other core concepts of palliative care. In the sense of resilience adding value to core concepts well-known in palliative care and functioning as an umbrella term for them, a broader definition of resilience is recommended. It should leave room for having respect for each individual’s personal concept of resilience. In consequence, it is important to educate not only patients but also their professional and informal caregivers about resilience and provide training opportunities. Based on the results of our interviews, we suggest raising awareness of the term among those just entering the profession (e.g. medical students and other health professionals). The role of staff in fostering resilience should be clearly defined, as they could be trained based on that role and then act as important multipliers for the implementation of a resilience concept that will be feasible in palliative care. For this, it is essential to proceed as already known from established core concepts: to move from more theoretical approaches toward clinical practice, analyzing and revising the resilience concept, and its components in real-life palliative care settings, and, finally, to develop interventions fostering resilience in patients and caregivers.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241254839 – Supplemental material for ‘Not a panacea’ – Expert perspectives on the concept of resilience and its potential for palliative care
Supplemental material, sj-docx-1-pcr-10.1177_26323524241254839 for ‘Not a panacea’ – Expert perspectives on the concept of resilience and its potential for palliative care by Katja Maus, Frank Peusquens, Milena Kriegsmann-Rabe, Julia-Katharina Matthias, Gülay Ateş, Birgit Jaspers, Franziska Geiser and Lukas Radbruch in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank the participants of the interviews and focus groups, without whom this research contribution would not have been possible. We would also like to thank our student assistants Charlotte Brockmann and Johanna Mischnick from University Hospital Bonn for their support with the transcription work.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.