
Abstract
Background:
Groote Schuur Hospital is a large Academic Hospital in South Africa that is in the process of integrating palliative care (PC) via a vertical nurse-led doctor-supported (VNLDS) service that was initially established to deliver clinical care. PC integration should occur across multiple dimensions and may result in variable degrees of integration between levels of the healthcare system. This research evaluates the VNLDS through a theory-driven evaluation to describe how the service affected integration.
Methods:
A mixed-method sequential design consisting of a narrative literature review on the theory of integration and PC, retrospective quantitative data from a PC service delivery database, qualitative data from semi-structured interviews and document analyses. It was structured in three phases which assisted in confirming and expanding the data. Statistical analyses, deductive thematic coding and documentary analyses were conducted according to the conceptual framework of PC integration.
Results:
The PC integration process was facilitated in the following ways: (i) the service provided good clinical PC; (ii) it was able to integrate on a professional level into specific diseases, such as cancer but not in all diseases; (iii) developing organizational structures within the service and (iv) the observed benefit of good clinical care increased the value stakeholders assigned to PC, thereby driving the adoption of PC. However, there are still clinicians who do not refer to PC services. This gap in referral may be grounded in assumptions and misconceptions about PC, especially at the organizational level.
Discussion:
Observed PC service delivery is core to integrating PC across the healthcare system because it challenges normative barriers. However, the VNLDS could not achieve integration in leadership and governance, education and hospital-wide guidelines and policies. Whole system integration, foregrounding organizational commitment to PC excellence, is core to integrating PC.
Conclusion:
The VNLDS service has effectively linked PC in specific disease profiles and normalized the PC approach where healthcare workers observed the service. These integrational gaps may be grounded in assumptions and misconceptions about PC, especially at the organizational level.
Plain language summary
This article evaluates a nurse led doctor supported service in providing palliative care and how it affected the integration of palliative care in an Academic Hospital in South Africa. This study will help us understand the goals of integration, the extent of integration achieved by this service and how and why it was achieved or not.
Introduction
Access to palliative care (PC) services is recognized as fundamental in the continuum of care; unfortunately, there is limited access to these services, especially in low-middle-income countries (LMIC).1–3 Multiple integration strategies are being used to integrate PC services and it is essential to evaluate how strategies work, especially in LMIC where the needs are so great. 4 Groote Schuur Hospital (GSH) is a large Academic Teaching Hospital (ATH) in South Africa that is in the process of integrating PC. 5 For the past 10 years, a PC service has been provided by a vertical nurse-led doctor-supported (VNLDS) service in the hospital. The provision of PC services in an ATH is aligned with the South African National Policy Framework and Strategy for Palliative Care Policy (NPFSPC) based on the World Health Assembly 67.19 PC resolution, which provides guidelines on PC service delivery in hospitals.1,6 Furthermore, this Framework describes PC in an ATH as ‘a specialist palliative care service at regional and tertiary hospitals. Centres of excellence will be established at academic hospitals to support education and research in palliative care’. 6 Therefore, the role of a PC service in an ATH extends beyond the provision of clinical care. The NPFSPC was adopted in 2017, and the PC service in GSH had, thus, been started without policy guidance and may provide a service different from that envisaged in the policy. Therefore, it is essential to evaluate this service to identify gaps in its integration process and establish how and why it was or was not achieved.
Gröne and Garcia-Barbero 7 state that integration is ‘the act of making a whole out of parts; the co-ordination of different activities to ensure harmonious functioning’. Integration is the process, methods and tools to achieve the harmonious functioning of the different dimensions of a healthcare system.8,9 These different dimensions need to be coordinated to ensure patients and families have access to PC when they need it. These dimensions are complex and interlinked and there are a number of theories describing them. This research draws from Valentijn’s so-called ‘Rainbow Model of Integrated Care’. Valentijn et al. 10 linked integrated clinical health care with an integrated health system. This framework takes account of the dynamic nature of a health system and the non-linear patterns of integration. 10 It identifies six integration dimensions, namely, clinical, professional, organizational, system integration, functional and normative integration. According to this model, integration of services can happen at different levels, namely micro (clinical integration), meso (professional and organizational integration) and macro (system integration). In addition, Valentijn’s theoretical framework also discusses that integrative care requires normative integration at all levels of care. It is the final step to integration and describes the development of mutual values, vision, trust and culture. Valentijn et al. 11 also describe functional integration as including key support functions and activities structured around the service to ensure accountability and decision-making. Functional and normative integration are interconnected at all levels, 11 and the prevailing hospital organizational culture plays a vital role across all these levels.
Organizational culture is a complex phenomenon, universal but challenging to define, dynamic and indistinct. 12 Martin describes it as shared sets of understanding and meaning guiding behaviour and social interactions in a particular organization. 13 ‘This is the way things are done around here’ is a layman’s and easily understandable description of organizational culture. 12 Therefore, formal change may be easily introduced, for example, a new policy or dress code, but the unwritten values and rituals must be tackled with sensitivity and understanding. For this reason, disruption of ‘how we always do things’ in an organization is not always welcomed and can be met with the marginalization of a new intervention. 14 For example, PC challenges stakeholders to acknowledge the suffering and death of patients, and, sometimes, their mortality. This produces uncomfortable feelings and may even disrupt an individual’s way of thinking about their discipline. Thus, the integration of PC into the culture of an ATH and the normalization of PC may be one of the most significant dimensions of integration. There is a need to evaluate both functional and normative integration, and especially culture when evaluating a new service, such as the VNLDS.
The integration process may also vary in the ‘intensity’ thereof may vary depending on the unit of care. 15 Some stakeholders may prefer activities to be linked with an adequate referral process only with good communication between the referring service and the PC service. 15 Other stakeholders would prefer activities to be coordinated where clinical information is shared to manage the transition of patients between different units, such as a multidisciplinary meeting. Furthermore, stakeholders will not engage in PC interventions deemed inappropriate and unresponsive to their and their patients’ needs. 16 In addition, these clinical needs cannot be addressed in isolation – for example, patients cannot be referred to a unit unless the unit forms part of the hospital’s standardized referral process, which requires technology, standard operating procedures and monitoring. 17 This is especially true in an ATH, where functions are too complex to operate only in one domain. Therefore, achieving in-depth, appropriate, responsive but sustainable PC health service integration may require further health system integration. Kaasa et al. 18 recommend that PC integration in oncology needs to have both vertical and horizontal aspects as well as multi-dimensional integration.
To manage the complexities of providing PC, a dedicated PC team works in GSH. It currently consists of two PC-trained professional nurses (one acting as a coordinator), two auxiliary social workers, an administrator and two volunteer PC-trained medical doctors. This research evaluated the ability of VNLDS services to strengthen the integration of PC in ATHs in South Africa. Understanding why and how things happened during the development and implementation of the VNLDS is essential to the evaluation. Principles of a theory-driven evaluation are used to gain information additional to the performance and merit of the program. 19 This approach was chosen because an experimental evaluation may not reveal how and why the strategies brought about the change. Astbury and Leeuw 20 state that how programmes bring about change is called ‘unpacking the black box’ to explore the inner components and logic of programmes.20,21 Although counterfactual evidence is important in an evaluation, the national policy implies that there should be no ATH without a PC-integrated service. 6 Furthermore, PC is a complex intervention and its integration into the ATH may be influenced by multifaceted aspects, for example, individual, hospital and societal factors. 22 Most importantly, understanding causal pathways of integration may assist with identifying improvements needed as well as implementing the strategies in other settings.
A conceptual framework was developed by drawing on Valentijn’s theory on integration and its dimensions, further literature on integration as well as PC integration. 10 This was developed in the research team and speaking with PC advisors in the field. We can thus conceptualize that a VNLDS service affected functional integration in the functional domains and dimensions, as illustrated in Table 1.
Domains of PC integration drawing from multiple sources.

PC, palliative care.
Contextual factors include the environment it is being integrated into, such as the PC need, patient issues, existing frontline services, resources as well as governance structures. In this research, these multiple factors can be further organized into clinical care as well as professional, organizational and systems integration to distinguish the aspect of integration. Having introduced these different factors, normalizing PC by addressing the organizational culture remains core.11,12
In this evaluation, organizational culture refers to the norms, values and behaviour that stakeholders have towards working with patients with life-threatening illnesses, the assumptions they have regarding PC and its role in the health system. Their vision and goals of PC integration form part of the normative process of integration. 10
The research aims to evaluate how a vertical nurse-led doctor-supported PC team served as a strategy to integrate PC into GSH. To make recommendations regarding an effective strategy for integration, it is important to evaluate current PC integration implementation strategies and how they align or do not align with contextual factors, as well as functional and normative integration.
Methodology
A mixed-method sequential design was followed, synthesizing retrospective quantitative data from a PC service delivery database (PC REDCap), qualitative data from semi-structured interviews and document analyses. This research was conducted from March 2020 to July 2022. A narrative literature review was conducted prior to the study to understand PC integration in hospitals and how it can be achieved. The conceptual framework for the research study draws from the Rainbow Model of Integrated Care and the principles of PC.10,18,25 This research was conducted in GSH, a large tertiary/quaternary academic hospital with 975 beds, which serves the Cape Metropole and attracts patients from across South Africa for specialized care. It is also a training hospital supporting both undergraduate and postgraduate education and a centre for research.
In phase I, demographic and clinical quantitative data were extracted from a REDCap database from the period January 2017 to June 2021. It was analysed statistically to describe the profile of the referred patients, the sources and timeline of the referrals, the PC services rendered to the patients and families, as well as the discharge process. The provincial data centre was also approached to access the date of death.
Also, in phase I, semi-structured interviews (n = 5) were conducted with VNLDS staff to describe the services delivered in 2022. Face validity of the interview guides was ensured by presenting the questionnaire to experts in the field of normative and functional integration and experts in the field of PC. Construct validity was derived by aligning this tool with the theoretical framework. The methodological triangulation of data strengthened trustworthiness by asking permission from sources about using information obtained outside the formal research process and sharing results with participants before any publications. 28 This is embedded research; therefore, assumptions held by the researcher were explored before commencing data collection via a recorded reflective interview between the researcher and supervisors. Reflexivity was further ensured by the researcher and research assistant keeping journals with short notes on discussions, as well as after interviews.
The qualitative data from the staff interviews were analysed using the framework analysis approach using deductive coding. 29 The interviews were transcribed and imported into NVivo version 14.23 (Lumivero). The researcher familiarized herself with and immersed herself in data sources. The coding framework was developed from the conceptual framework as discussed in the ‘Introduction’, drawing from Valentijn’s theory on integration. 10 Themes and sub-themes identified in the analysis of the interviews were coded. Codes and analyses were discussed with the supervisors and research assistant and attention was given to emerging themes not identified by the framework so as not to overlook any data. Negative cases or outliers were included and discussed. Codes were also discussed with advisors to check for bias of the researcher. These codes were applied to all the data sources and the data were charted across all the data sources of the study. Selected representative data were used to illustrate the resulting themes of the analysis.30,31
In phase II, analysis from the database and the interviews with the VNLDS service were merged, and these findings were discussed with the VNLDS staff to confirm and explain the data. This assisted in connecting with organizational documentation (n = 14) (see Appendix A) that explains and confirms the service delivery. The documents were thematically analysed using deductive coding and drawing from the conceptual framework as discussed in the ‘Introduction’. A data extraction sheet was used to analyse documents with regard to the name of the document, how, when and why the document is used, and for themes of functional and normative integration. Where PC is/is not in the document and how it is referred to. These factors were further supported by discussing them with the research team.
The data were further expanded by identifying wards and services with distinct referral patterns. The wards with limited PC were determined by listing all wards in GSH and discussing with the PC staff the logical explanation for limited referral to PC in these wards. For example, it is understandable that there will be limited PC referrals from an ophthalmology ward. If there was incongruence between the disease profile of patients in the wards and the number of referrals, interviews were conducted with staff from those units. These sequential interviews (n = 5) were conducted with purposively selected senior ward staff outside the PC service. Interviews were performed using a semi-structured interview guide drawing from the conceptual framework, analyses of the VNLDS interviews, database and PC literature.
Finally, all the data sets were integrated to evaluate the effect of the VNLDS in both the different domains. These findings were discussed with an independent observer and with the VNLDS.
Figure 1 illustrates how, in Phase I, quantitative and qualitative were merged to expand on the phenomena. Further interviews and document analyses were done to explore the findings further. If all four data sets confirmed the findings, it was deemed to be strong convergent evidence and if one dataset did not confirm the findings, it was reported as divergent evidence. The merging of the data and the inferences drawn from the data was done in discussion with the research team. The details of the merging and inferences are attached in Appendix A.

Schematic representation of the methodology.
Results
Results from the integrated findings are presented in nine main clusters concurrently, as described by the conceptual framework and the dimensions of integration.
Clinical profile of referred patients and dimensions associated with clinical integration
This dimension explores person-focused care provided by the PC service.
The provision of patient and family-centred care
The literature review found that clinical PC is provided when patients and families receive pain and symptom control; psycho-social and spiritual care, informed participatory decision-making; and families are informed and are seen as part of the care team; patient and family education is provided; and bereavement care is provided.18,25,27
Clinical PC service delivery
Interviews with the VNLDS staff indicated that the VNLDS delivers a consultancy service across the whole hospital. There is evidence of increasing numbers of patients being referred to the VNLDS service from across the hospital with multiple conditions. The majority of patients were bedbound (43%) or required assistance (41%), with very few being fully mobile (15%). On average, 58% of PC patients were referred specifically for end-of-life care as a reason for referral. However, this decreased from 91% in 2017 to 36% in 2021 (see Table 2). Other reasons for referral are comprehensive care, including symptom control, counselling, education, social support and placement.
Referral data to the PC service from 2017 to June 2021 (REDCap database).
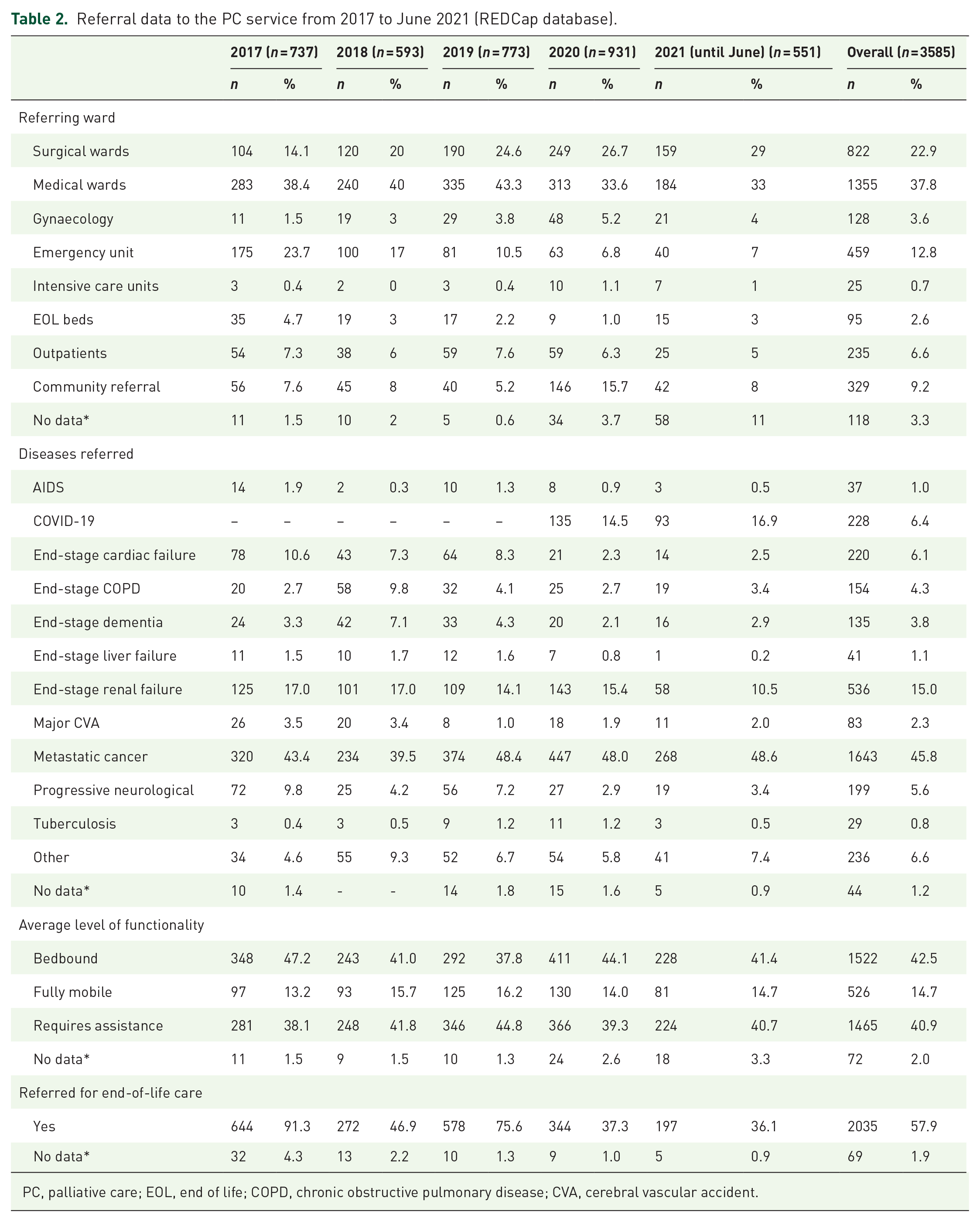
PC, palliative care; EOL, end of life; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident.
Reviewing available mortality data (n = 1894) of these referred patients on the REDCap database, most patients (53%) were referred in the last week of life. See Figure 2.

Time of PC referral to death.
The data centre confirmed that place of death of (n = 1188), 27% of patients died in hospitals (Table 3). It further confirmed that 191 (16%) died at home. The data centre could only provide the death data for 33.1% of patients because home deaths are not always recorded on the provincial data system, which is not linked to the Department of Home Affairs, where deaths are recorded. All hospital death data are available; if no place of death is recorded, we can assume the place of death is home.
Place of death.

Pain and symptom control
There is strong converging evidence from the database, document review and interviews that patients referred to the VNLDS receive pain and symptom control. The database indicated that 97% of the referred patients received pain and symptom control.
This is further supported by evidence of routine pain and symptom control in document review of the PC stationery. There is also evidence that pain and symptoms are important markers by which other staff evaluate the impact of a VNLDS: For me, it is when they come and initiate the pain control; it helps the patient a lot. The patient is then very comfortable and so. The palliative care is good, they tick all the boxes. (Wardstaff2)
Psycho-social and spiritual referrals
The database and documentation indicate that 100% of the patients received psycho-social support. The majority (89,6%) of the patients are classified by their social circumstances by the hospital as ‘poor’ (family unit earns less than R100,000 per year); (51,4%) or ‘very poor’, which is classified as formally unemployed, no formal income (38.2%), emphasizing the need for social support: Is the patient working? If the patient is still working, I do it. Referral to the social worker so that I, the social worker can help the patient with the work papers. (Pallsocial1)
Interviews with the VNLDS show that the team also links with a multifaith spiritual team who liaises with the team daily. There is evidence in the documentation of routine spiritual assessment and referral to a spiritual team.
Informed and participatory decision-making
The interviews with the VNLDS indicated that the treating teams must break bad news and share prognoses. However, the VNLDS service assesses patients’ understanding of the disease and prognoses and assists in deepening this understanding and exploring care options with both the patient and family. Routine data collected by the service indicate an average of 50 family meetings a month, and there is a specific family meeting stationery in the documentation analysed, including educational material provided to patients and family education of the illness, the care and medication that is and will be required.
Bereavement care
There is evidence of bereavement follow-up (28.9%), and the stationery includes a section to record a bereavement call. However, most patients are referred to community resources for PC and bereavement care after discharge.
Patient and family education
This domain is both clinically and organizationally important. Patient and family educational material in the form of pamphlets is available. Staff outside the VNLDS service identify the role of the VNLDS service inpatient and family education as a positive contribution to care and empowers the family to continue on their own: There are patients, the family members, actually, I’ve seen the family members before palliative team is involved and after you the PC, are involved. And there’s a huge difference. There’s, there’s the unanswered questions, you know, the PC answer those questions. The family members feel the sense of, not so much control, but understanding, so they they’ve come to terms with what is to be expected, and what they can do. So, that they actually have this, this empowerment. (Wardstaff3)
Dimensions associated with professional integration
The provision of collaborative care
The provision of collaborative care is conceptualized as the appliance of automatic triggers, multidisciplinary care provision, ensuring continuity of care and the provision of end-of-life care across the hospital.10,23
The use of automatic triggers to initiate PC
There is divergent evidence on applying automatic triggers on when to refer to PC. There is documentation (a referral sheet and a PC indicator tool). Still, the referral patterns demonstrate that mainly cancer patients (45%) (Table 1) are referred with few cardiac patients (6%) and HIV and TB patients (1.5%) referred, suggesting that the indicator tool is not used regularly. There is further evidence that referrals are late in the disease trajectory: I do not know if all the patients (needing palliative care) are referred to palliative care. (Wardstaff3)
Multidisciplinary care implementation
There is very little evidence of multidisciplinary care during the evaluation period at GSH. According to the VNLDS staff interviews, the PC team works and provides care as an interdisciplinary team. However, the PC is linked but not integrated into the ward teams. The VNLDS refers to rehabilitative services. This lack of multidisciplinarity has not been impacted by the VNLDS: It’s more the doctors that are giving the orders. There’s no multidisciplinary approach. There’s no, like a combined view on the patient. So, if there’s a doctor’s rounds, the nurse will accompany the doctor and take the orders. (Pallnurse2) Yes, so I don’t; I don’t think the nursing staff feel empowered enough to actually make suggestions, not only with regards to the palliative team, but I mean with any other, whether it’s dietitian or, you know, if there’s any social services. (Wardstaff1)
Ensuring continuity of care
According to the literature, PC systems integration occurs when there are clinical care pathways for patients to ensure continuity of care. The VNLDS refers patients to Community Health Care and Hospices. The service also follows the patients up 1 week after discharge to ensure community care is in place: Then I do a follow up with the patient to see if they got the community key services; then if not, I will follow up with the coordinator working in that specific area where the patient stays to find out the delay. (AdminPC)
The provision of end-of-life care
Documents provide evidence that comprehensive end-of-life care is provided for patients referred to PC but not to all dying patients in the hospital: And it’s almost like they want to push the patient to a side cubical, fine when they are dying. (Wardstaff2)
Dimensions associated with organizational integration
The availability of information systems
Drawing from the literature, one of the aspects of organizational integration is that there are monitoring and evaluation tools available to evaluate the PC in the hospital. 16 Currently, there are monitoring and evaluation services available in the VNLDS but no other PC monitoring and evaluation in the hospital.
There is evidence of monitoring within the service: And yes, then also daily daily, weekly, monthly. I will do the stats. (PCAdmin)
However, outside the service, the outcomes of patients who need PC are not always known: No, I may not always know the outcomes of those patients. (Wardstaff2)
Education in PC at various levels
Conceptually, PC education should be provided at various levels. 1 Furthermore, continuous medical education and patient and family education should be available. 25
Basic education
There is evidence that 100 of the 3400 healthcare professionals employed by GSH 32 from various disciplines have been trained in basic PC. From the interviews with the VNLDS staff, 100 HCPs in the hospital have received basic PC training. The VNLDS service is involved in final year medical students’ training once a week and in the training of Gynaecology Oncological Fellows.
Intermediate education
From the interviews, family physician registrars rotate for 6 weeks through the service. There is also intermediate training for oncology registrars in the hospital linked to the university. However, neither family physicians nor oncologists refer to the VNLDS. There is no further intermediate-level training in the hospital.
Advanced training
From the interviews, there is no advanced PC training in the hospital. Both the doctors volunteering in the VNLDS service have specialized PC training.
Continuous medical education
The documentation indicated that the VNLDS provided a quarterly lecture as continuing education on PC open to the hospital but this stopped during COVID-19. There is an acknowledgement that there is a need to provide further continued education in PC across the hospital: There needs to be more empowerment of the current team in the ward and further continuous education. (Pallnurse2)
Leadership and governance
Data analysis included a review to assess whether there is a strategic plan for PC in the hospital, managerial oversight and accountability, financial and resources support and clinical leadership.
No strategic PC plan was found. There is documentation evidence of clinical, administrative managerial oversight through minutes of meetings. Quarterly meetings are held with management as a whole team, and staff report to their clinical managers weekly. Medical clinical leadership is provided by university staff.
Guidelines and policies
Hospital documentation was reviewed for integrated guidelines and standard operating procedures to provide evidence of organizational integration. Stand-alone guidelines and policies do exist in the VNLDS but not in other areas of the hospital: No, I don’t, I don’t have any policies. I was actually going to speak to sister at palliative care because we need, not only an SOP for nursing, but also if we can actually incorporate it from doctors as well. (Wardstaff1)
Five documents were found as stand-alone policies or guidelines supporting the VNLDS PC service. PC was integrated into one stand-alone PC chapter in the surgical guidelines and one question in the home oxygen referral system.
PC workforce and resource support
Two professional nurses, two auxiliary social workers and a clerk are employed in PC by the hospital. The university employs medical doctors volunteering in the hospital. The professional nurses are not in dedicated PC posts. The VNLDS have a dedicated office, family meeting and teaching space. The university contributes to the resources of the service. There is a debriefing service for the PC staff. There are two further nurses in the hospital with intermediate PC training in other departments who work in oncology and surgery.
The availability of essential PC medication
Essential medications, as specified by the WHO Essential PC Medicine list, are all available in the hospital.
Researching PC
There is evidence of PC research in the VNLDS but no evidence of dedicated PC research outside the service.
Normative integration (norms, values, behaviour)
There is the assumption that PC services are only for end-of-life care. This assumption has not been changed by the VNLDS: I think that most are walking around with the assumption or going around with the assumption that palliative care is just for patients who are going to die or are now diagnosed with cancer and they gonna die at the end of the day. (Pallnurse2)
The behaviour of avoidance of end-of-life care and referring when no further curative management can be done has been shifted by the VNLDS service as evidenced by more patients being referred for reasons other than end-of-life care.
The outside wards value the VNLDS service for both clinical and staff care. The PC staff has assisted the ward staff in managing their distress and has assisted in creating spaces, like a butterfly, room for reflection: The palliative care sister assisted us in addressing the moral distress and how to manage death and dying. (Wardstaff3)
Normalizing
The VNLDS service has become part of routine care, contributing to the service’s acceptability and value: Um, you know, I think, I think what makes a big impact is to see people who do it regularly. So, I think, I think people talk about palliative care and refer to palliative care more because they see it happen, uh, and they see the clinical benefit of it. So, I think it’s a bit of a chicken and egg situation, but I think the, the more active a palliative care team is in a ward with clinical decision making, uh, the more it’s used and the more valuable it becomes and the more engaged with it other doctors are. (Wardstaff4)
Discussion
The extent of integration achieved
The VNLDS service has successfully implemented the integration of PC at a clinical level, in accordance with the recommendations outlined in the conceptual framework, across the majority of hospital wards. 11 There is both quantitative and qualitative evidence of pain and symptom control, family involvement, and patient and family education.18,25 The VNLDS has demonstrated the importance of family meetings, which empower patients and families in decision-making. Carolan et al. 33 highlighted that family distress may have a significant ripple effect, impacting the entire family system. Family meetings are thus core to assessing family structure, support and educating patients and families on the required care, as essential components of a PC service.18,25,27 The impact of family support by the VNLDS has allowed most patients to be discharged home with referrals to support from home-based care organizations rather than dying in the hospital. Continuity of care is further strengthened by linking them with community services. 25 Linking hospital PC and networking beyond the hospital is essential to both clinical hospital integration and strengthened PC care in the community system. 28
How the service improved the valuing of PC and PC integration
The clinical service expansion is attributed to observing the positive outcomes of working with the PC team. As stated by one of the participants, ‘the more you see it, the more valuable it becomes’. Observing the positive engagement and improved outcomes of referred patients and their families ensures value is assigned to PC, which assists in integration. Patients’ continuity of care is ensured; most patients referred to the GSH PC service are discharged and receive PC in the community and die at home. These observed perceived benefits and compatibility with current service needs affected the adaptability of the PC approach. 16 Users are more receptive to the PC approach, which, in turn, provides legitimacy to the PC service. 16 For example, a senior staff member states that the VNLDS makes a ‘huge difference’, and subsequently, this unit refers to PC regularly.
The acknowledgement of the impact of the end-of-life is as important for staff as it is for their patients. The open engagement with the suffering and actual dying process has assisted in addressing the staff’s personal moral distress, which has been an important finding of this research study. PC has provided staff outside the VNLDS with the tools to care and also to engage with their own home and work experiences openly. For example, a butterfly room was opened in a ward as a place for contemplation for families and staff. Subsequently, vulnerability around death and dying is respectfully acknowledged and managed in this ward. There is thus a realization of the benefit of PC service through attending to the staff’s needs, which enhances the receptiveness towards PC. 16
Limitations in the extent of clinical integration
Unfortunately, most patients are referred for end-of-life care, an average of 7 days after hospital admission. In addition, most of these patients already require assistance with activities of daily living or are fully bedbound. Therefore, the fully recognized impact of early specialized PC services has yet to be reached as demonstrated in global research. 28 For example, Temel et al. 34 demonstrated that specialized PC services early in the disease trajectory of patients with metastatic lung cancer improve quality of life, reduce anxiety and depression in patients and marginally prolong life. However, as indicated by this research and other studies, late referrals to PC may result from an assumption that PC is only for actively dying patients.3,35 This, together with the observed behaviour of avoidance of patients at the end of their lives, may result from limited, late referrals. 36 The medical world has assisted in what Sallnow et al. 35 describe as an ‘unbalanced’ societal approach to death, dying and grieving focuses on unnecessary clinical interventions and may exclude the psycho-social and spiritual dimensions of dying. Therefore, the referral to PC services may be convenient at this stage of care to avoid the dying process and accompanying complex care and emotions. Subsequently, this behaviour of disengagement with patients at the end of their lives may also cause disengagement with the whole PC process, and not recognizing the benefit of PC at an early stage of the disease trajectory. However, this behaviour is challenged by the VNLDS service by persistently stating that PC starts long before the end-of-life. Subsequently, one of the normative aspects of integration accomplished by the VNLDS service is the normalization of death in accordance with the WHO definition of PC and a global movement to value death and dying as an important and integral part of life.35,37,38
A further limitation in the extent of integration is that VNLDS is not reaching all disease-specific populations that require PC. The incidence of metastatic cancer patients referred to the VNLDS compared to other life-threatening illnesses and the causes of mortality in South Africa are disproportionate. 6 In South Africa, TB, diabetes, cerebrovascular disease, heart disease and HIV were the leading causes of death in 2018. 39 Despite this, very few TB and HIV patients (1.5%) were referred to the VNLDS, and of note, the cardiology outpatients were the lowest source of outpatients referrals. This disproportionate referral pattern leaves many patients with cardiac and infectious diseases without access to PC. Automatic triggers and awareness on when to initiate PC are well established within oncology, but in organ failure and infectious diseases, PC needs are not met. 40 The VNLDS service has initiated automatic triggers in patients with pancreatic adenocarcinoma and end-stage renal patients, which are reflected in the referral patterns. For example, all patients in GSH who are declined for dialyses are automatically referred to PC services. 41 This is evident in the number of patients with renal failure referred to PC. However, the PC service currently works mainly on voluntary referral and linkage has not been uniformly successful. Automatic triggers specific to the context are thus core to further integration and universal PC access. 42 The SPICT-SA indicator, specifically designed for South Africa, considers the unique patient burden and wide range of patients who require PC. 42 The assumption that PC is only for metastatic cancer or EOL care is a significant assumption that requires further professional interaction to address this gap in access to PC.
Enabler
This commitment and the drive to integrate PC on a professional level comes from inside the VNLDS service and the university’s Faculty of Health Sciences. The VNLDS staff are passionate and committed to integrating PC. Rhee et al. 43 identified factors affecting PC integration in Africa and named advocates and pioneers as key factors driving integration. However, they warn that integration fuelled only by advocates is high risk as sustainability further requires other strategies and infrastructure support. 43 PC being driven by only a small group of passionate PC advocates, lack of commitment from organizational leadership, limited trained PC staff and lack of PC education are all factors in GSH echoing barriers experienced across the African continent. 43 Sustainable PC leadership in the hospital and across Africa will be important to ensure PC integration. Admittedly, moving this paradigm is beyond a clinical service and was thus not achieved by the VNLDS service.
Linking PC to the prevailing culture
The organizational culture of siloed service delivery results in a need for more professional integration across all disciplines, including PC. Disciplines stay in their ‘own lane’ and that is the ‘way things are done’. Most services in the ATH are only at a level of integration where services are linked with doctors working in parallel and disciplines functioning in their siloes. 15 It may be ambitious to imagine a horizontal PC service in a hospital with limited PC-trained staff, where disciplinary excellence is core to organizational culture. 7 Consequently, a PC service that is only linked may be appropriate, at first, within the ATH context to align with the prevailing culture of vertical excellence. However, currently, innovation and technical excellence are celebrated, and an intervention that deals with death and dying may not be perceived as key. Although the VNLDS service is valued, it does not yet form part of ‘excellence’. Labelling PC as excellent care is one of the most significant paradigm shifts to normalize PC and align it with the prevailing culture of excellence. The prevailing structure of ‘how things are done’ will be important as the initial pathway in integration.12,16 To ensure this, linkage across all the appropriate disciplines will not be successful if further aspects of functional integration do not anchor it at all levels of care. 28
Limitations in functional integration
This lack of functional integration is evident when we observe that nurses are not in dedicated PC posts, there is no PC strategic plan, and the accountability structures are not integrated. Atun et al. 16 advise that integrating an intervention into the broader health system governance structure will require alignment with existing regulatory mechanisms, creating unified accountability frameworks, integrating reporting and establishing a joint performance management system. 16 All of the above integration structures mentioned by Atun require action on an organizational level. This action can be unpacked as decision-making, commitment, support and willingness of key leaders to achieve PC integration. 19 Furthermore, the current GSH team needs to conform to the recommended staffing, especially the requirement for PC-trained nurses and medical doctors. 6 Kaasa et al. 18 confirm the lack of trained PC specialists is a substantial barrier to the integration of PC and hampers the confidence by which other specialists refer to PC services. Furthermore, as stated above, this impact of limited-service delivery and specialist PC training in an ATH may impact beyond the ATH. This is evident when we review the limited research and education in the PC discipline, which impacts nationally and in the rest of Africa. 44 This need for whole system integration is especially evident when we evaluate the lack of PC education in South African ATHs. Physicians and surgeon trainees receive no PC training, and there are no PC mentors in these departments due to the absence of PC-trained consultants in most ATH. Overloaded curricula and services may underpin this lack of training, resulting in ATHs’ workforce having very limited PC knowledge and skills. However, the Departments of Radiation Oncology across South Africa have successfully integrated a PC course into registrars’ training without overburdening registrars or consultants. 45 This leaves the VNLDS as a small group of healthcare workers within the hospitals with PC skills.
This lack of investment in PC may be an overburdened and under-resourced healthcare system, and another new intervention may be deemed an extra burden on the healthcare system. 46 GSH is a well-functioning hospital in South Africa but is also overburdened by limited resources. Waddington and Egger 47 highlight that integration of new interventions is not always welcomed because, in a system where the wider health system is not functioning well (South African healthcare sector), it is questionable to change aspects of the system that are working. Furthermore, a new intervention has to demonstrate a significant impact on cost containment. 47 Unfortunately, the VNLDS service has no economic evidence that it is cost-effective apart from discharging 72% of patients home for EOL care. The need for contextually specific economic evidence is paramount to enable further integration. This is further complicated by the limited research and costing models for PC in low-resource settings.48,49 Shifting the functional aspects of integration will require economic commitment from leaders and willingness and commitment to integrate PC.
Limitations
This is embedded research and the researcher is explicit about her support of PC, which may introduce bias with stakeholders and their responses to her. Most of the data were obtained through interviews and participants may also have recall bias. Participants not in favour of PC integration may also not want to be interviewed, which may limit counterfactual information.
Data in the databases also depend on the actual input of the records. However, as part of the database management process, data are validated regularly following set data management operating procedures. The limitation of the database was that it contained limited data on the patients’ deaths.
Conclusion
The VNDL service has been able to harmoniously integrate clinical PC services in specific units and disease profiles and has brought about an organizational culture of normalizing a PC approach. Observation of the service by hospital staff outside of the specific units and realizing the benefits have further contributed to the adoption of PC integration. However, PC has yet to be adopted across all units or disciplines. The context of vertical service delivery among all disciplines and the lack of organizational integration may underpin the reasons for this. In conclusion, PC integration will require organizational commitment and economic evidence to ensure PC integration in an ATH to have an overall impact on national PC integration.