
Abstract
Background:
In Switzerland, continuous deep sedation until death (CDSUD) is not legally regulated and the current clinical practice guidelines on palliative sedation from 2005 do not refer to it. In contrast, in France, a neighbouring country, CDSUD is regulated by a specific law and professional guidelines. International studies show that in culturally polymorphic countries, there are variations in the end-of-life practices between linguistic regions and that a linguistic region shares many cultural characteristics with the neighbouring country.
Objectives:
This study aimed to explore the attitudes of palliative care physicians from the French-speaking part of Switzerland on the question of whether CDSUD should be legally regulated in the country, and to identify their arguments. Our study also aimed to assess whether a hypothetical Swiss law on CDSUD should be similar to the current legal regulation of this practice in France.
Design:
We conducted a multicentre exploratory qualitative study based on face-to-face interviews with palliative care physicians in the French-speaking part of Switzerland.
Methods:
We analysed the interview transcripts using thematic analysis, combining deductive and inductive coding.
Results:
Most of the participants were opposed to having specific legal regulation of CDSUD in Switzerland. Their arguments were diverse: some focused on medical and epistemological aspects of CDSUD, whereas others emphasized the legal inconvenience of having such regulation. None had the opinion that, if CDSUD were legally regulated in Switzerland, the regulation should be similar to that in France.
Conclusion:
This study allows to better understand why palliative care physicians in French-speaking Switzerland may be reluctant to have legal regulation of CDSUD. Further studies covering the whole country would be needed to gain a more complete picture of Swiss palliative care physicians on this question.
Keywords
Introduction
In the context of palliative care, continuous deep sedation until death (CDSUD) is an important therapy of last resort.1–3 However, this practice remains controversial at both the clinical and ethical levels, especially due to its irreversibility and the arguable lack of proportionality. 4
Although there are some international data on the prevalence of CDSUD,5,6 (including data gathered in Switzerland 7 ), it is impossible, or at least imprudent, to make comparisons and determine whether this practice is ‘rare’, ‘common’ or ‘frequent’, because of the terminological and conceptual inconsistencies, diverse applications and varying perceptions of these practices. Many international comparative studies show that CDSUD is influenced by the culture of the country in which it is practised, and particularly by the legal and social contexts. Several cultural differences in the attitudes of palliative care practitioners and the decisions and practices of CDSUD have also been observed between countries.8–10 However, all the data suggest a trend towards an increase in the use of CDSUD across the world. For example, in Switzerland, between 2001 and 2013, this practice increased from 4.7% to 17.5%. 7
According to linguistic theory, language is an important part of the culture of a country.11,12 Some studies show that in culturally polymorphic countries, there are variations in the end-of-life practices between linguistic regions and that a linguistic region shares many cultural characteristics with the neighbouring country of the same language.13–15 For instance, Van den Block et al. 15 have demonstrated that, while there is a tendency towards the use of CDSUD in the Walloon region (the French-speaking part of Belgium), euthanasia is more frequently practised in Flanders (the Dutch-speaking part of the country). A study performed by Chambaere et al. 14 shows that, in the metropolitan Brussels-Capital Region, where both language communities are represented, French-speaking physicians perform CDSUD more often than their Dutch-speaking colleagues. The findings suggest that these differences are present irrespective of the geographical separation, but more in line with the language used.
Switzerland offers an opportunity to explore in depth and from various perspectives the cultural-linguistic influence on end-of-life issues, such as CDSUD. The country has four official languages (German, French, Italian and Romansh), with their own linguistic-geographical areas of very different sizes. Previous studies confirm that there are cultural differences in medical end-of-life decisions and practices between the German-, French- and Italian-speaking regions of the country.16,17 For example, a study highlights that CDSUD is used more frequently in the Italian-speaking region than in the French- and German-speaking areas. 17 However, to the best of our knowledge, these findings were not compared with what is practised in the neighbouring countries, such as Italy, France and Germany. Another study, performed by Faeh et al., 18 although not dealing with end-of-life issues but with risk factors and causes of death across Switzerland, clearly shows that the situation in the French-speaking part of the country is more similar to that in France and that the setting of the German-speaking part of Switzerland corresponds more to that in Germany. This suggests that issues relating to end-of-life care in the French-speaking part of Switzerland, especially CDSUD, may be influenced by the French context.
In this regard, it is interesting to consider that France is the first and only country in the world to have explicitly and precisely regulated CDSUD at the legal level. 19 The law enacted in February 2016, named the ‘Claeys–Leonetti law’ after its initiators, Alain Claeys and Jean Leonetti, members of parliament, allows CDSUD at the patient’s request in two situations: (1) in the case of a serious and incurable condition endangering life in the short term, in so far as the patient’s suffering is refractory to treatment, and (2) when the decision of a patient with a serious and incurable condition to stop treatment is life-threatening in the short term and is likely to cause unbearable suffering. The law also provides that where the patient is unable to express his or her will and the physician estimates that the life-sustaining treatment constitutes an ‘unreasonable obstinacy’, he or she can decide to forego it and apply CDSUD. 20 It should be noted that this CDSUD aims directly for the level of unconsciousness (Richmond Agitation Sedation Scale (RASS)-4/-5) and not patient relief. In other terms, the goal is a completely unresponsive patient, even if the patient experiences relief at lesser doses.
In Switzerland, CDSUD is not legally regulated, and in the current national clinical practice guidelines on palliative sedation this practice is not explicitly mentioned. 21 On the other hand, the new guidance issued by the Central Ethics Commission of the Swiss Academy of Medical Sciences, incorporated into the professional code of healthcare workers, explicitly mentions this treatment; CDSUD may only be performed in dying patients and, contrary to the rules of the ‘Claeys–Leonetti law’, 20 the depth of sedation applied is to be symptom guided. 22
The objective of our study was to explore how palliative care physicians working in the French-speaking part of Switzerland perceive a hypothetical legal regulation of CDSUD in the country. Our study also aimed to assess whether in the eyes of the participants such hypothetical legislation on CDSUD should be similar to the law in France. To the best of our knowledge, and at the time of writing this article, no studies have comprehensively investigated these questions.
Materials and methods
Study design
Between February and November 2019, we performed a multicentre exploratory qualitative study based on face-to-face interviews with physicians who were working or had previously worked in a specialized palliative care unit in the French-speaking part of Switzerland. The overall study focused on CDSUD as an alternative to assisted suicide in Switzerland. The results of this main study have been published elsewhere. 23 We conducted two secondary data analyses, one of which, focusing on assistance in suicide, has already been published. 24 Here, we publish the results of the other secondary data analysis of CDSUD. In this article, we summarize the methodological aspects of the main study (data collection) 23 and then elaborate on the method of the secondary data analysis concerning the legal aspects of CDSUD in Switzerland. All methodological aspects are detailed in Supplemental File 1 according to the COREQ (COnsolidated criteria for REporting Qualitative research) checklist. 25
Data collection
Four palliative care units certified by the Swiss Association for Quality in Palliative Care and located in the French-speaking part of Switzerland served as the basis for sampling. The inclusion process was progressive and the sample size was determined by data saturation. 23 MT, a postdoctoral researcher in palliative care, with expertise in ethics, law, linguistics and qualitative research, conducted face-to-face interviews with physicians, using the interview guide.
Prior to this study, MT had no relationship with the participants. At the beginning of each interview, the researcher clarified that this study was carried out as part of her postdoctoral project and provided comprehensive research-related information.
Data analysis
All the interviews were transcribed by MT, who was the only person with access to the recordings and integral transcripts. RA and RJJ had access to anonymized parts of the transcripts. The data were manually analysed by MT; no software tools were used.
The thematic analysis was performed using a hybrid approach of deductive and inductive coding. For the analysis of the transcripts, a deductive approach was followed using a simple framework. 26 Two major themes were identified beforehand: (1) a hypothetical legal regulation of CDSUD in Switzerland in general, including arguments for and against and (2) the specific legal regulation of CDSUD as it exists in France, and arguments for and against. For this second theme, the researcher explained the French law on CDSUD in detail beforehand, clarifying precisely the three situations in which CDSUD can be requested by patients (see ‘Introduction’ section). These two main themes were researched in all the transcripts. In the next step, minor themes were identified inductively as they emerged from the analysis and were not predefined. After that, transversal analyses of all the transcripts were conducted, and all the themes were synthesized. It is important to note that the analysis was carried out on the original French versions, and only the results and quotations were translated into English. RA and RJJ contributed to the process of data interpretation.
Results
Sample size and characteristics
We contacted nine palliative care units in the French-speaking part of Switzerland and received responses from all of them. Of the nine units, six agreed to participate and we included four of them in the study. We conducted interviews with 12 physicians from these four palliative care units, but we were only able to transcribe and include 10 of the interviews in our analysis. We excluded two interviews: one because it was too short and the other because of a technical problem rendering the recording inaudible. The duration of the interviews ranged from 13 to 46 min. Detailed characteristics of the participants can be seen in Table 1.
Characteristics of the participants.

Palliative care is not a specialty in Switzerland but only a subspecialty.
For example: Certificate of Advanced Studies (CAS), Diploma of Advanced Studies (DAS) and/or Master.
Until 2019.
Various configurations, depending on the percentage of the work.
Hypothetical legal regulation of CDSUD in Switzerland
Only one participant was fully in favour of the legal regulation of CDSUD. Two participants hesitated, without giving a clear answer: they presented arguments both for and against. Most of the participants were firmly against legally regulating CDSUD in Switzerland. The results presented in this section are schematically summarized in Figure 1. All quotations are presented in Table 2.

Main results.
Arguments for and against the legal regulation of CDSUD: Quotations 1–17.
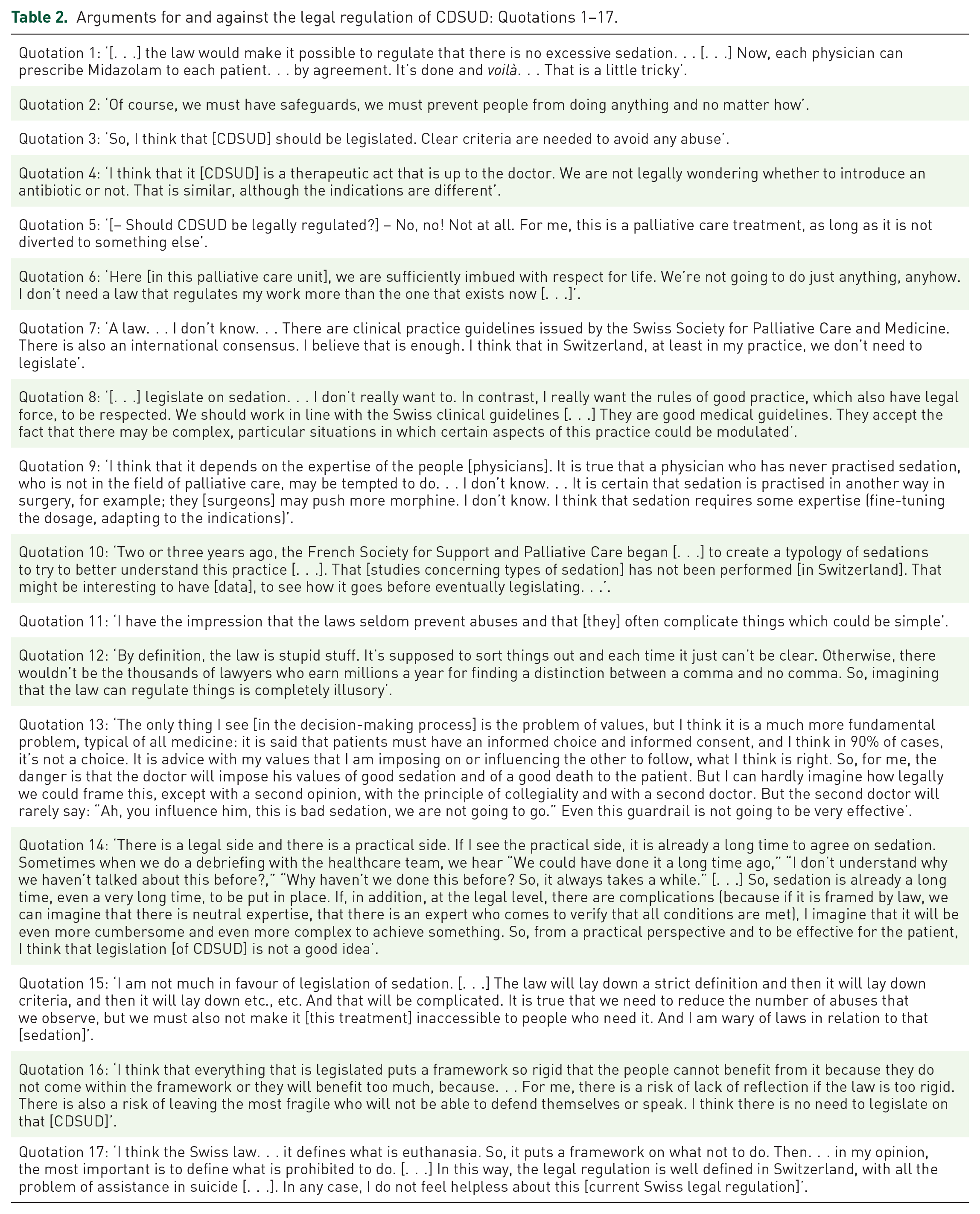
Arguments for the legal regulation of CDSUD
Only one argument for the legal regulation of CDSUD was identified. Some participants stated that legislation of CDSUD could reduce the risk of ‘excessive sedation’ (see quotations 1–3).
Arguments against the legal regulation of CDSUD
Arguments against the legal regulation of CDSUD were diverse: they focused on medical, epistemological and legal aspects of this practice. Many of the participants based their argument on the risks of the legal regulation of this practice.
Medical aspects of CDSUD
Participants pointed out that CDSUD is a therapeutic act in line with the philosophy of palliative care and, for this reason, would not need to be legally regulated in a specific way (see quotations 4–6). Some participants considered clinical practice guidelines on palliative sedation to be sufficient safeguards (see quotations 7 and 8). One participant pointed out that training healthcare professionals to correctly perform palliative sedation would be more important than a law in ensuring safe and correct practice (see quotation 9).
Epistemological aspects of CDSUD
One participant suggested that, prior to potential legislation, it would be appropriate to gain more information by conducting research on CDSUD in Switzerland by using the work of the French Society for Support and Palliative Care, for example (see quotation 10).
Legal aspects of CDSUD
Several participants stated that any law would be, by definition, imperfect; it would never solve the problem and, despite the law, abuses would always be possible (see quotations 11 and 12). One participant stated that the main problem during the decision-making process with regard to CDSUD is imposing a particular point of view on the patient, and a law would not be able to solve that satisfactorily (see quotation 13). Most of the participants highlighted the potential risks of having detailed legal rules on CDSUD. They stated that it would risk complicating the clinical situation by being too rigid, to the detriment of patients. For example, this could risk delaying the implementation of CDSUD due to additional procedures (see quotation 14). Legislation also risks making this therapy inaccessible for some patients who do not meet the predefined legal criteria, although from a clinical perspective, these patients may need it (see quotation 15). One participant confirmed that legislation of CDSUD may make it impossible for some patients to access the therapy, adding that it may also pass it on to others who, from a clinical perspective, do not need it (see quotation 16). One participant stated that the current Swiss law [Swiss Criminal Code] already regulates all prohibited issues and that seems sufficient (see quotation 17).
Hypothetical legal regulation of CDSUD in Switzerland, as in France
The question concerning the hypothetical legal regulation of CDSUD in Switzerland, as in France, was put to some of the participants, mainly those who had put forward or tried to put forward arguments for the legislation of this practice. No participant who was asked this question was familiar with the French law on CDSUD. Following the explanation of the French law (see ‘Materials and methods’ section) they agreed that if CDSUD were legally regulated in Switzerland, the rules should in no way be inspired by the French regulation.
Discussion
Our exploratory study of the opinions of palliative care physicians working in the French-speaking part of Switzerland on the hypothetical legal regulation of CDSUD in their country is the first of its kind. Most of the participants were opposed to having specific legal regulation of CDSUD in Switzerland. Their arguments were diverse: some focused on the medical and epistemological aspects of CDSUD, whereas others emphasized the legal inconvenience of having such regulation. None had the opinion that, if CDSUD were legally regulated in Switzerland, the regulation should be similar to that in France. To the best of our knowledge, no similar studies on this topic have been conducted in Switzerland. Consequently, direct comparisons are not possible.
Contrary to Faeh et al., 18 our study shows that the participants were not influenced by the French context in terms of wishing to imitate its law. We found that most of them were not even aware of the specific legal regulations regarding CDSUD in France. One of the reasons for this may be that CDSUD is not (yet) broadly practised in France. 27 From a legal point of view, CDSUD is also legal in Switzerland as long as it acknowledges the general legal conditions for medical interventions (i.e. medical indication and informed consent). The French emphasis on patients’ individual right to request CDSUD is, however, lacking in the Swiss legal system.
Our results could be useful for elaborating a national study aiming to explore this topic in depth. It would be particularly interesting to conduct an interview study with physicians working in the three large linguistic regions of Switzerland: the German-, French- and Italian-speaking areas. Such a study could investigate their opinions on the current situation in Switzerland, its impact on clinical practice in these linguistic regions and whether there is a need to introduce specific legal regulations at the federal or cantonal level (i.e. regional level).
Most of the participants in our study were fully opposed to the legal regulation of CDSUD in Switzerland. They pointed to medical, epistemological and legal aspects of CDSUD. First, they stated that CDSUD is a therapeutic act in line with the philosophy of palliative care and, for this reason, would not need to be legally regulated. On the one hand, this argument may seem intuitive. Indeed, since the beginning of palliative care movement in the 1960s, this treatment of last resort, referred to as ‘sedation’ or ‘terminal sedation’, has been an integral part of the approach.28,29 However, from the beginning, this practice has also sparked controversies and debates worldwide.30,31
Considered ‘a slow euthanasia’, 30 ‘an extreme facet of end-of-life sedation’ 4 or ‘an exceptional last resort measure’, 32 CDSUD can be used inappropriately and contrary to the philosophy of palliative care. International studies have highlighted numerous abuses of this treatment, especially when it is performed as a form of euthanasia – that is, with the intention and the effect to hasten death – in countries with legal regulation of medically assisted dying.33–35 Overbeek et al. 36 have even concluded that the legal distinction between euthanasia and ‘palliative or terminal sedation’ may not always be clear in clinical practice. Our previous study has shown that CDSUD is sometimes used as an alternative to assisted suicide in Switzerland. 23 In this situation, it is legitimate to ask whether a specific regulation of CDSUD may help prevent abuse. This is in line with the opinion of some participants in our study, whereby the legislation of CDSUD could reduce the risk of ‘excessive sedation’. However, due to the lack of studies exploring this topic in depth in France – a country that is unique in its specific legal regulation of CDSUD – it seems difficult to develop this aspect. A recent international survey across eight European countries shows that ‘palliative sedation’ is commonly considered within the general medical law, in legal protections regarding patient autonomy and through clinical practice guidelines. 37 In some countries, specific recognition of the right to receive ‘palliative sedation’ is included in national laws. However, to the best of our knowledge, studies evaluating the impact of these specific legal regulations on clinical practice, especially on the reduction of the risk of excessive sedation, are lacking thus far. Moreover, it also seems relevant to ask whether such studies would be feasible from a methodological perspective.
Although the Swiss palliative care physicians in our study were rather opposed to a specific law on CDSUD, they acknowledged the importance of some quality assurance and tended to attribute this task to the medical profession. Some study participants considered the present professional guidelines on palliative sedation to be sufficient safeguards. As previously mentioned, in many countries, palliative sedation is only regulated by clinical practice guidelines. Our recent systematic review shows that such documents exist not only in Europe, but also in North America, Australia and Asia. 38 These texts have been developed to help palliative care physicians address the challenges related to this practice but also to close the gap between research and practice and, eventually, to improve care for patients and their relatives. 39
However, clinical practice guidelines are not legally binding per se, as they are recommendations developed by professional societies, not by a politically legitimate legislative body. In spite of this, they are not legally irrelevant. They can, for instance, be used by courts in assessing physician responsibility by helping to clarify what is an acceptable standard of a particular medical treatment, according to the state of the art. 40 As some participants of our study mentioned the risk of paternalistic abuse when administering CDSUD, it will be pivotal for clinical practice guidelines to include a statement on ethics, including the principles of respect for patient autonomy and shared decision-making. 41
It is important to mention that in 2005 a group of experts in the Swiss Society of Palliative Medicine and Care developed clinical practice guidelines on palliative sedation. The document was published in German, French and Italian,21,42,43 and interestingly, does not explicitly mention CDSUD. Although this text has existed for more than 15 years, it is still not clear whether and how it is implemented across the country. We know that there are institutional policies in several palliative care units, but the content of these documents is widely ignored; to the best of our knowledge, no review of these texts has been published thus far. Finally, at the time of writing this article, a group of Swiss experts is revising the current clinical practice guidelines.
Methodological limitations
Our study has one main methodological limitation that should be taken into account when interpreting the results. As previously mentioned, our principal study was focused on CDSUD as an alternative to assisted suicide in Switzerland, 23 and the present study, as did another one, 24 was based on a secondary analysis of the data. For the main study, 23 a progressive inclusion of participants (i.e. inclusion until data saturation was reached) was performed. Data saturation was defined as the point at which no new themes emerged from the analysis of the interviews. The present article shows a sub-analysis of the data from this study as, at the time of the analyses, we discovered interesting elements that were not directly related to the objective of our main study. Data saturation on that particular point of interest in the secondary data analysis could therefore not be sought as the data collection had already finished. Moreover, theoretical saturation was not sought either because there was no literature that would allow us to establish the theoretical saturation point. However, the data were sufficient to explore this topic and to provide ideas for further studies in this area.
Conclusion
This study, which is the first of its kind in Switzerland, allows a better understanding of why palliative care physicians in the French-speaking part of the country may be reluctant to support the legal regulation of CDSUD. The results of this study could be useful for academic research and for societal debate, although additional studies covering the whole country would be needed to gain a more complete picture of how Swiss palliative care physicians see this question. Further studies are also required to explore the impact of the current lack of legal regulation of CDSUD on clinical practice and on the relationship between physicians, patients and patients’ families.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524231219509 – Supplemental material for Should continuous deep sedation until death be legally regulated in Switzerland? An exploratory study with palliative care physicians
Supplemental material, sj-pdf-1-pcr-10.1177_26323524231219509 for Should continuous deep sedation until death be legally regulated in Switzerland? An exploratory study with palliative care physicians by Martyna Tomczyk, Roberto Andorno and Ralf J. Jox in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors are grateful to the heads of the palliative care units for responding to the call of MT and facilitating contact with palliative care physicians. They also thank all the participants in the study for sharing their knowledge, experience and reflections regarding this topic. In addition, they would like to give their warm and sincere thanks to the Editor of this journal and the two reviewers for their expertise and time, which helped them reflect on this complex topic and greatly increased the quality of the manuscript. The first author would also like to express her gratitude to Prof. Jacek Łuczak (1934–2019) from the Palium Hospice and Chair and Department of Palliative Medicine at the Poznan University of Medical Sciences in Poland for his invaluable medical and existential reflections, and to Liz Eggleston, native English speaker and professional proofreader, for her excellent linguistic suggestions.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.