
Abstract
Background:
Physicians are frequently asked what they would do in the position of their patients, and they have significant influence on end-of-life decisions. Therefore, it is crucial to understand the connection between physicians’ personal end-of-life preferences and their clinical practice and the impact of this connection on patient care.
Objectives:
To explore how physicians perceive and manage the impact of their end-of-life preferences on their clinical practice and end-of-life decision-making.
Design:
Exploratory qualitative study using in-depth interviews.
Methods:
Forty-five interviews were conducted from January to November 2022 using a semi-structured interview guide. Participants included three types of physicians: general practitioners, palliative care physicians, and other medical specialists in Belgium (Flanders), Italy, and the United States (Wisconsin). Data collection and analysis were informed by the reflexive thematic analysis approach. Audio recordings were transcribed verbatim, and NVivo 12 was used for coding and analysis. Consolidated criteria for reporting qualitative research (COREQ) was followed.
Results:
Physicians acknowledge the impact of their personal end-of-life preferences on their clinical practice and emphasize the importance of maintaining objectivity and centering decision-making on patient preferences. Physicians adopt strategies to mitigate potential biases. There is a divergence of opinion about whether it is appropriate to share when asked what they would do in the position of their patients. Most believe focusing on patients’ values and priorities is essential and others feel sharing is crucial to maintain trust. Physicians struggle with ethical tensions and moral discomfort, particularly when patients’ requests conflict with their beliefs. Physicians experience personal and professional growth through end-of-life discussions and reflection.
Conclusion:
Physicians recognize and attempt to manage the impact of their own end-of-life preferences on their clinical practice. Physicians are not in agreement about sharing when asked what they would do in the situation of their patients.
Introduction
Physicians are pivotal in guiding patients and shaping healthcare decisions, which are particularly complicated at the end of life. These decisions may involve withholding or withdrawing life-sustaining treatment, palliative sedation, or assisted dying (a term encompassing voluntary-assisted dying, medical aid in dying, euthanasia, and physician-assisted suicide (PAS)).1 –3 Since physicians encounter confronting medical scenarios and are frequently asked by patients for guidance based on what they would do in similar circumstances, it is reasonable to assume that they have reflected on their personal preferences.4,5 The extent to which physicians’ personal end-of-life preferences and beliefs impact their clinical end-of-life practice raises important ethical and clinical considerations.
Physicians face challenges balancing their personal end-of-life preferences and beliefs with professional practice, particularly in the context of end-of-life decision-making. 6 Personal values, emotions, and external pressures can influence their practice, at times making it difficult to maintain full neutrality. 6 This internal struggle can become more pronounced when physicians’ personal treatment preferences unconsciously shape their perceptions of patient desires and preferences, further complicating their ability to remain impartial. 7 The difficulty of navigating these dilemmas during end-of-life discussions is considerable, as personal biases can inadvertently interfere, creating professional hazards and hindering the goal of providing truly patient-centered care. 8
Physicians also encounter difficulty reconciling their personal ethical integrity and conscience with their professional practice, particularly when confronted with ethically controversial situations or when asked to perform or refer for practices they find morally objectionable.9,10 Some physicians prioritize their moral integrity by refusing to be involved in some end-of-life practices or by referral to colleagues. 9 There can also be an emotional toll on physicians who provide care that conflicts with their personal preferences or professional judgment, particularly when they perceive the care as being futile, harmful, or inappropriate. 10 In some cases, deeply held religious beliefs also shape physicians’ approaches to treatment, leading to internal conflict for physicians. 11 This emotional strain can have a negative impact on their psychological and physical well-being and job satisfaction. 10 These challenges illustrate the importance of exploring the complex relationship between physicians’ end-of-life attitudes and preferences and the end-of-life care they provide.
Existing research examining the relationship between physicians’ end-of-life preferences and their clinical practice are generally focused on limited end-of-life decisions (e.g., withholding and withdrawing treatment), a specific influence (e.g., religious beliefs), or are restricted to one geographic region.2,6,7,9 Consequently, a comprehensive understanding of how physicians perceive and manage the connection between their end-of-life preferences and clinical practice is lacking. International comparative research can provide valuable insights into how cultural, social, and system-level differences influence physicians’ personal end-of-life preferences. A qualitative study design allows for a deeper and more nuanced understanding of physicians’ diverse perspectives and can shed light on how they perceive and manage the link between their personal preferences and the end-of-life care they provide. It does this by providing rich data and illustrative quotes that can reveal and clarify complex notions. Qualitative methods can also reveal important commonalities and challenges faced by physicians, enhancing our global understanding and potentially fostering alignment between clinical care and patient values. To the authors’ knowledge, no international comparative qualitative studies have been conducted in this domain. Given the lack of current qualitative data and the pivotal role physicians play in shaping complex end-of-life decisions, it is crucial to better understand how physicians’ personal end-of-life preferences relate to their clinical practice, particularly how they balance personal beliefs, preferences, and ethical integrity with professional responsibilities.
Our guiding research question was: How do physicians perceive and manage the impact of their personal end-of-life preferences on their clinical practice and end-of-life decision-making?
Methods
Study design
This exploratory qualitative study employed semi-structured in-depth interviews and an inductive analytic approach, using reflexive thematic analysis.
Context and setting
We selected physicians practicing in jurisdictions with diverse cultural environments and varied levels of experience with assisted dying legislation. We included physicians in Belgium (Flanders), Italy, and the United States (Wisconsin). Belgium has had an assisted dying law in place since 2002, while Italy currently lacks such legislation, and in Wisconsin, despite legislative debates over the past 20 years, assisted dying remains illegal. These jurisdictions were selected based on their assisted dying status, prior research collaborations, professional connections, and feasibility of participant recruitment.
Participant recruitment
We used a convenience sample in each country. Due to their varied levels of experience treating patients at the end of life, we sought to include three types of physicians: general practitioners, palliative care physicians, and other medical specialists with a high likelihood of seeing patients facing end-of-life issues (i.e., cardiologists, emergency medicine, gastroenterologists, geriatricians, gynecologists, internal medicine, intensivists, nephrologists, neurologists, oncologists, and pulmonologists). Our goal was a distribution of physician types that included a minimum of five general practitioners, five palliative care physicians, and five medical specialists in each jurisdiction, amounting to 15 in each jurisdiction and 45 total physicians. Physician participants were identified through the networks of our research partners in each country, and via outreach through medical associations, professional societies, and self-identification after completing an online survey linked to this study. This qualitative exploration is part of a multi-method international study called PROPEL: Physician Reported Preferences for End-of-Life Decisions. The study objectives are to explore physicians’ personal end-of-life preferences and the factors that shape them, and the connection between physicians’ personal end-of-life preferences and their clinical practice.12 –14 Following initial contact by email or telephone, potential participants received an email invitation detailing the study, information on the research team, and eligibility for participation.
Inclusion and exclusion criteria
Currently practicing physicians in the following groups were eligible for participation: general practitioners, (specified) clinical specialists, or palliative care physicians. Participants were excluded if they had less than 2 years of clinical experience or were unable to do the interview in English. We originally planned to include only physicians with five or more years of experience. However, since we encountered recruitment challenges and most of the previously recruited physicians had 10–40 years of experience, eligibility was expanded.
Data collection
Data was collected between January and November 2022 using a semi-structured interview guide. The interview guide (Supplemental Appendix A) was developed following an exploration of the literature and discussions among the research team. It was then pilot tested with three physicians and adjusted for clarity and appropriateness before use. Most interviews were conducted online using a video conferencing platform (Zoom or Teams) due to COVID-19 restrictions. However, five interviews were conducted in person, at the office or home of the participant, and one at a public library. The interviews varied in length from 30 to 80 min, and no repeat interviews were conducted. Notes were made following each interview. All interviews were conducted by the lead author (S.M.), a female doctoral researcher with previous experience conducting qualitative research with physicians (credentials—MSc, MPH). S.M. had no prior relationship with the participants, apart from two Wisconsin physicians who had previously provided care for her mother. Due to the complex nature of the interview topic, participants were offered language support through the attendance of a second researcher who spoke their native language and could explain complex questions or responses. Some European physicians accepted this option (Italy 4, Belgium 1). A demographics form was completed at the start of each interview.
Data analysis
Interviews were audiotaped and transcribed verbatim. Data collection and analysis were informed by the reflexive thematic analysis approach. A reflexivity statement was developed by the lead researcher (Supplemental Appendix B). Reflexive thematic analysis is an ideal approach for this study as its flexibility allows for a deep examination of the multifaceted nature of end-of-life preferences without the constraints of rigid frameworks, making it well-suited to capture the complexity of this topic. 15 It emphasizes personal meaning and perception and aligns with our focus on physicians’ subjective experiences and reflections. This method’s iterative, reflexive nature ensures that the researcher’s role in interpreting sensitive, personal data is acknowledged, providing room for richer, more nuanced insights. 15 It excels in exploring the intersection of broader social and cultural contexts with individual decision-making, making it ideal for understanding the varied influences on physicians’ preferences and identifying patterns across the data. In addition, it is an inductive, data-driven approach, which allows for open exploration, making it particularly useful for research without predefined categories, enabling the discovery of unexpected themes. 15
Interview transcripts were imported to NVivo (version 12) for analysis. Thematic saturation was achieved with 15 interviews in each jurisdiction. Data were evaluated during collection to ensure that saturation was reached. Consistent with reflexive thematic analysis, we interpreted saturation as analytic sufficiency, meaning that the data corpus was rich and detailed enough to support fully developed themes rather than being tied to a fixed numerical threshold. In each country, after approximately 15 interviews, recurring patterns appeared consistently, and saturation was considered reached when three consecutive interviews failed to reveal any major new themes, indicating that further data collection was unlikely to meaningfully deepen or alter the thematic structure. The lead author (S.M.) coded all transcripts, and another team member (F.D.) independently coded four transcripts for comparison. Transcripts were not shared with participants. Initial codes were discussed and refined (by S.M. and F.D.), and themes and sub-themes were developed. The themes were then refined and discussed further by the full research team, and similar or overlapping themes were collapsed or removed. A thematic map was then developed and evaluated, and the research team identified, discussed, and selected associated interview quotes. Participants did not provide feedback on the findings. The consolidated criteria for reporting qualitative research (COREQ) checklist was followed.
Results
We collected data from interviews with 45 physicians—15 in each country—reaching our recruitment goal. Participants included 23 female and 22 male physicians (Table 1). Most were white/European (43), identified as either Christian (23), non-religious (16), or another religion (6), and fell within the age groups <40 years (18), 40–59 years (22), and >60 years (5). We nearly achieved our target balance of selected specialties with 15 general practitioners, 14 palliative care physicians, and 16 other medical specialists participating.
Characteristics of participating physicians, per jurisdiction.
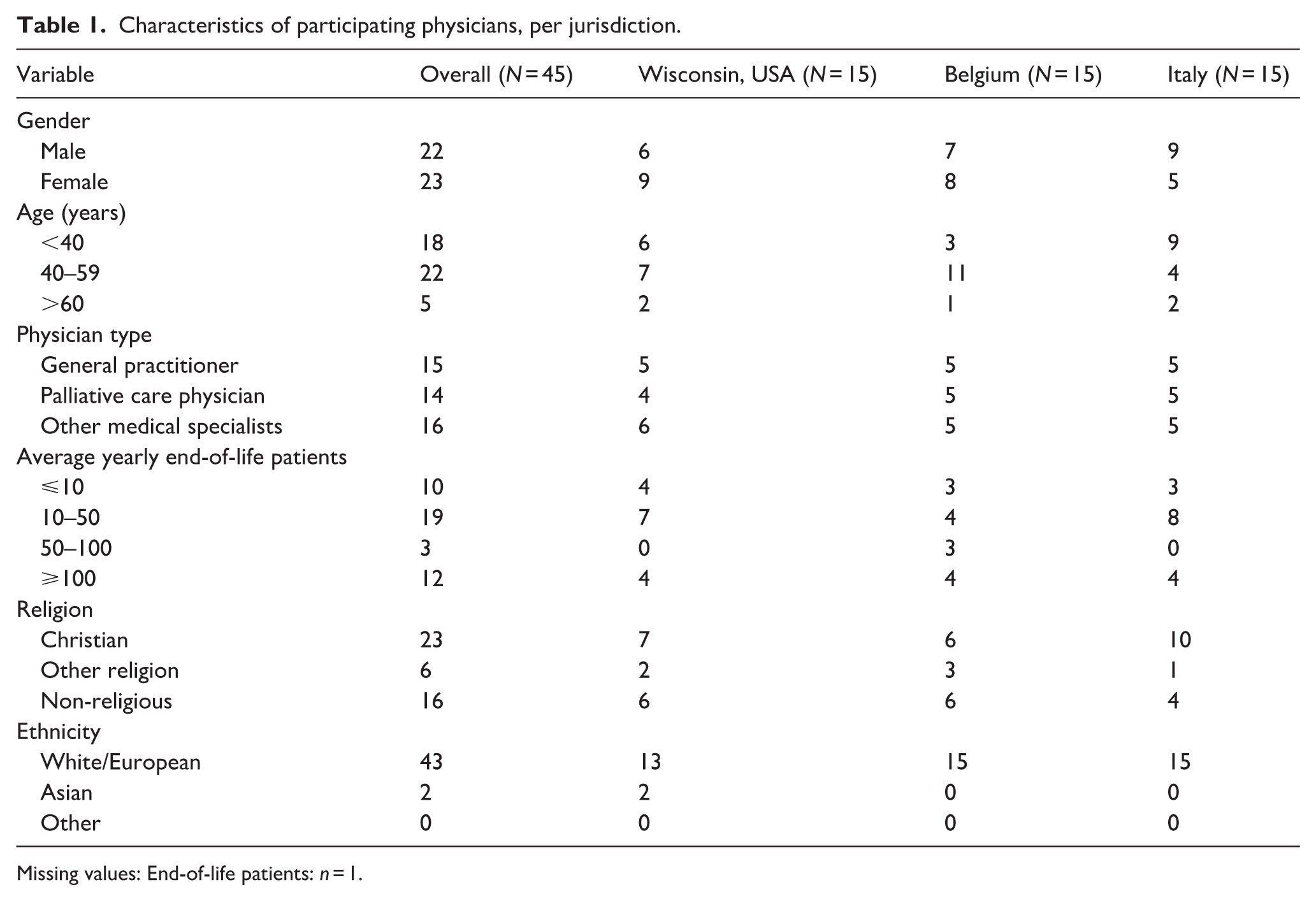
Missing values: End-of-life patients: n = 1.
We identified four main themes and two sub-themes related to how physicians perceive and manage the impact of their own end-of-life preferences on their clinical practice (Figure 1).

Main themes related to physicians’ perceptions and management of their personal preferences on clinical practice.
Theme 1: Balancing personal and patient preferences
Physicians feel it is natural and unavoidable to bring their own values and preferences into their practice, but try to be cognizant of it and remain objective in order not to impose their own preferences on patients.
Physicians openly acknowledged that their own values impact their clinical encounters and say they work to keep patients and patients’ priorities at the center of the decision-making process and not provide too much influence or allow their own beliefs and values to direct decisions. They emphasized the importance of being aware of their own preferences and respectful of patients’ wishes.
Theme: Balancing personal and patient preferences
Connected quotes:
I hope that I don’t push people in any direction because these are my values. But I think it’s a little bit normal that you take your own values with you when you have conversations with patients and families. But I hope I give my patients and families enough freedom to make their own decisions. (Medical specialist, Belgium)
Some physicians described it as an ongoing struggle to be conscious of their personal feelings and preferences during clinical encounters without allowing their feelings to interfere with patient decisions.
It’s been challenging for me to set aside my personal beliefs because as a physician, and I didn’t realize this until probably my third year in practice, where, how much influence you can have and how to separate the discussion on end of life care from your own personal beliefs. And it’s still a struggle, but it’s easier to talk about and it feels less personal. (General practitioner, Wisconsin)
Physicians work to understand their patients’ values and preferences and consider it crucial to ask thoughtful questions and listen carefully to patients to really understand their wishes and remove themselves from the discussion. Physicians reported that even when trying to set aside their own beliefs and values and keep them separate from their clinical interactions, their preferences always infiltrate to some degree.
I always put up that wall because what I want for myself is probably going to be different than for my patients, right. But I, I think about, I think the general framework of what you think is right, what we all think is right, like shapes, shapes the way we practice in our decision making. But I think, like my number one job is not to do what I want to do, it’s to do what my patients want to do. And there is a wall. I think there’s not as much of a wall as we think. (Medical specialist, Wisconsin) Every time is an effort, of course. The fact I have the, a clear idea for me and the fact I have a way of a point of view about these things. It’s not, it doesn’t make my work easy, easier. No. Many, many times. It could be . . . that I disagree. But I don’t express my disagreement, of course. (Palliative care physician, Italy) Often it’s quite easy to lengthen the life of a patient. Adding some days, weeks, months to a patient’s life. Often this works, but without the prospect of a normal life, or a life with, with any form of quality in the future and this is a personal opinion, quality of life. We always try to have a view about what would this person’s view be on quality of life. So we talk if it’s possible, with the patients and with the family, with the general physician to have a little bit an idea of how this person would value quality of life. But still then I think you also have your own values that infiltrate a little bit this this process, I, I think it’s not possible to really set this completely aside because you, you get information from many parties, from many persons but I think that your own preferences will always infiltrate a little bit. (Medical specialist, Belgium)
Nuanced differences in attitudes were identified between physician groups. Some general practitioners emphasized the importance of exercising caution with respect to exerting influence and giving patients room to consider their values and respecting their wishes. Palliative care physicians stressed the importance of personal reflection and understanding their own preferences and shared that doing this allows them to remove themselves during clinical encounters and have less influence. Some medical specialists shared a desire to limit the influence of their preferences on patients by listening and learning about patients’ wishes and keeping them at the forefront of the decision-making process. Physicians across all countries shared that they try to keep a separation between their personal preferences and clinical practice, and there is sometimes a struggle to do so. Italian physicians, in particular, highlighted the difficulty and occasional struggle of distancing themselves during clinical interactions.
Sub-theme: Collaboration to manage personal influence
Physicians recognize the connection between personal preferences and clinical practice and highlight the importance of actively managing their influence by talking with colleagues and making decisions as a team to reduce the impact of personal influence.
Physicians cited discussions and collaboration with colleagues as a way to share responsibility for making important end-of-life decisions, recognize personal bias, and reflect collaboratively to make the best possible decision for patients. This method also allows them to gather diverse perspectives for making future decisions.
Sub-theme: Collaboration to manage personal influence
Connected quotes:
That’s one of the benefits of doing this work in a team. So, you know, when your little alarm bell goes off that you’re feeling sort of personally, you know, engaged or you wonder if your own beliefs or preferences might be clouding the situation for you, you can ask a team member to, you know, give you feedback and so try to be help you be a bit more objective. (Palliative care physician, Wisconsin) It’s very important that you make decisions in a team, because in that way you have a lot of people, a team and every person in the team has this in his or her values. So that’s why it’s important never to make the decision alone, I think because the decision will be influenced by personal values. (Medical specialist, Belgium)
Sub-theme: Sharing personal preferences at the request of the patient
Physicians shared that they are frequently asked in clinical encounters what they would do if they were in the position of the patient, or the patient were their loved one.
Most physicians reported that they try to respond to this question by turning the focus of the discussion back to the patients’ priorities and offering to evaluate the available options. However, some physicians feel they have a responsibility to be open and honest and share what they would do in the patient’s situation. Physician responses varied greatly, with some feeling it was appropriate to share their own preferences, others being very opposed to sharing, and some saying they may share depending on the situation. We found that more physicians were opposed to sharing because they felt their preferences, values, and priorities may differ from those of their patients, and they considered it ethically inappropriate to influence their patients in a direction that may not be in line with the patient’s own preferences.
Sub-theme: Sharing personal preferences at the request of the patient
Connected quotes:
Sometimes people will ask me, what would you do? Or what if this was your father or something like that? And so I think that some separation is definitely important. So I, I try my very best not to just give an answer after a question like that, but to say, well, I would want to talk to my father and see what his wishes are. And then kind of transition it back or reflect that back to the patient and their family to make sure that that we’re really focusing on what he or she wants or would want, rather than my projected values onto them. Certainly that’s not perfect, but at least try to have some separation. (Medical specialist, Wisconsin)
The physicians who support sharing their own preferences do so because they feel it is necessary to maintain a trusting relationship by being open and honest with patients when asked. Others share because they hold a more informed position due to their medical knowledge and experience, and feel they would be in the best position to provide requested counsel. Some also said they share their own preferences as a way to model decision-making for patients.
I always say to the patients what I would do if they were my father, my mother, my brother or sister, I gave you the advice as if you were my family. And that is really respected by the patients. Many of them followed me in that direction. (Palliative care physician, Belgium)
General practitioners and palliative care physicians were divided on whether to share their own preferences with patients, while most other medical specialists said they would not. Physicians across all specialties stated they would typically attempt to redirect the conversation to the patients’ priorities to minimize their own influence on decisions.
Theme 2: Personal preferences shaping clinical guidance (Act according to the golden rule)
Physicians say they hold their own preferences as an ideal to guide interactions with patients, and some strive to treat others as they would want to be treated themselves (the golden rule).
Many physicians shared that they work to keep a balance and separation between their personal beliefs and preferences and their clinical practice to maintain focus on the patient’s priorities. However, some physicians shared that they feel it is a natural response to a situation to consider what one would want for themselves, and this can be an appropriate starting point for discussions and decision-making, before they focus on the patients’ desires.
Theme: Personal preferences shaping clinical guidance
Connected quotes:
I think my own end-of-life preferences probably completely shape my clinical practice for patients who might be in a certain scenario . . . I’m trying to do what I think is best for patients, is in their best interest, and is in their family’s best interest. So, since we all think a lot about ourselves, in some ways that’s what I operate at if I don’t hear anything else, I always ask people what they want first, you know. But the thing that generally guides what I think people might like is my own preferences, and then easily guided by whatever someone really wants or needs. (Medical specialist, Wisconsin)
Several physicians, particularly Italian physicians, cited the phrase “treat others as I would want to be treated.” This maxim, found in many religious and philosophical traditions, represents a general moral guideline upholding the principles of empathy and ethical reciprocity, encouraging people to treat others with the same respect and kindness they would wish for themselves. Physicians shared that they try to consider patients’ situations also from their own perspective of wanting to avoid futility and suffering. They understand the patient’s final decision may be quite different from their own, but feel it can be a useful and positive point to begin contemplation.
I think that generally a physician tries to do his or her best depending on what you think could be the best for himself or herself in the same condition. (Medical specialist, Italy) I think I treat my patients as I want people to treat me, or I treat my patients as I want others treated. (Medical specialist, Belgium) That’s the most reliable way to know that I’m being honest and diligent and fair in my work with patients is to imagine, you know, how I would want to be approached and counseled and guided, offered in that type of decision making knowing that the end result might be a very different decision than I would make. But I think it’s, you know, maybe quite natural to want to, you know, to hold as a, as an ideal to extend to our patients what we think might be, the, again, how we would want I said as the health care provider, how I personally would want to be allowed to make decisions. I don’t think it’s a . . . negative. I guess, I would say I think it can be a positive. (Palliative care physician, Wisconsin)
Theme 3: Maintaining personal ethical integrity
Physicians are not comfortable acting against their own values in their clinical practice.
Physicians described a sense of moral distress and personal conflict between respecting and honoring patient wishes and acting according to their own convictions and values.
Theme: Maintaining personal ethical integrity
Connected quotes:
If you imagine that you’re practicing completely the opposite of your own conviction, it would be difficult. (Palliative care physician, Belgium) I think I need to be consistent. This doesn’t mean that I have to do to people exactly what I would do to me. But this means for me that I have to, I need to always check my beliefs and think about what I think, . . . what are my beliefs and what I’m doing to see if I am consistent with my values in my, that, and my values influence both my clinical choices and my work are the themes of my work, my values, and also the basis for my choices, . . . of my own preferences. (Palliative care physician, Italy)
Some physicians said they struggle when asked by patients and families to provide what they consider futile treatment. Physicians have encountered situations where they felt uncomfortable caring for patients with strong personal or religious beliefs that motivated them to request all possible medical efforts to prolong life at a point when the physician felt it was no longer appropriate. Others described situations of patients requesting assisted dying, which, for some physicians, was in conflict with their own beliefs and values. This was most prominent among Italian physicians, several of whom expressed opposition to assisted dying based on personal or religious beliefs. Several physicians said they would not be comfortable or willing to practice in a way that was not in accordance with their personal values.
An important part of our job, as this might be true in many, many fields. Like check your, check that the two are not putting your vision, your personal values into other people’s brain or taking decision for them. And it’s part of my value that everyone has the right to express their preferences on their own death. At the same time, it’s part of my values that I cannot decide to take their lives. (Palliative care physician, Italy)
Physicians across all specialties and countries described the importance of aligning their personal values and their clinical practice. Belgian physicians, in particular, discussed issues related to euthanasia as a source of ethical difficulty or discomfort.
My wife, she finds it difficult to think about me assisting in euthanasia, for example, so you have to balance that also. Your personal relationship with people can also have an influence on your work. Yeah. It can make you less comfortable when someone asks you for euthanasia. (General practitioner, Belgium)
Theme 4: Personal and professional growth through end-of-life discussions
Physicians reported that end-of-life discussions can be rich and help them grow as a person and a doctor.
Physicians described the potential for great value in dealing with complex issues and walking alongside patients during the difficult end-of-life phase. Some shared that engaging in end-of-life conversations was initially daunting or uncomfortable, but over time, the encounters became more comfortable and could be an extremely rewarding part of caring for patients and provided opportunities for growth, beauty, and lessons for them personally. Physicians also describe this engagement as a chance for meaningful connection with patients as fellow human beings. This finding also highlights that there is a bidirectional impact with physicians’ preferences impacting their practice, but also the practice impacting physicians.
Theme: Personal and professional growth through end-of-life discussions
Connected quotes:
If you are quite sound and . . . are happy with your work, and if you are curious and careful with patients, then your ability to cope with this decision and to create moments of discussion with relatives, with the patient becomes a very rich, very, a very rich moment. . .. because over time, you know that you are making yourself better in a certain related, and more able to work in a good way and more able to lead in a good way. (Medical specialist, Italy) I was always very comfortable in difficult conversation but I feel like in the last five years maybe I am, I feel more connected with people and that’s a very good thing for me and I hope for my patients. (Palliative care physician, Italy)
Some palliative care physicians shared that they were particularly drawn to palliative care as a way to be involved in meaningful connections with patients and believe there is a particular connection between the self and the delivery of palliative care that cannot be disconnected. No other clear differences were observed by medical specialty or country related to personal and professional growth through end-of-life discussions.
Discussion
Summary of main findings
This study offers novel insights into the relationship between physicians’ personal end-of-life preferences and their clinical end-of-life practice. Findings reveal that physicians acknowledge the impact of their personal values and beliefs on their end-of-life decisions; however, they emphasize maintaining objectivity and centering patient preference in their clinical decision-making. Some physicians adopt collaborative strategies, consulting with colleagues to mitigate potential biases and strive to balance personal ethical considerations with patient autonomy. A significant finding is that there is a divergence of opinion among physicians about whether it is appropriate to share when asked what they would do in the position of their patients. Most physicians believe focusing on patients’ values and priorities is essential. Some physicians feel it is necessary to maintain an open, trusting patient-provider relationship. Personal values, including the concept of treating others as you would like to be treated, underlie and guide the clinical interactions of some physicians. Physicians also report grappling with ethical tensions and moral discomfort, particularly when patients’ requests conflict with their own beliefs, such as in cases perceived as involving futile treatment or requests for assisted dying. Physicians report experiencing personal and professional growth through reflection and challenging discussions and find value and connection in end-of-life conversations.
Interpretations of main findings
Our findings confirm and expand on research suggesting a connection exists between physicians’ personal preferences and their clinical practice. 7 Physicians acknowledge that their personal values and preferences naturally emerge in clinical practice, particularly during intense end-of-life care situations, and they stress the importance of balancing these forces by maintaining professional distance and prioritizing patients’ wishes in decision-making. This balance appears challenging for physicians, as some describe it as an ongoing struggle to prevent their personal beliefs from influencing patient choices. While they manage this with practical strategies, it is important to consider the underlying normative question of whether it is appropriate for physicians to consider their personal preferences in a professional context. Since physicians also report using their personal preferences as a guide for what might be desirable in a given situation, it may be perceived as a natural and appropriate starting point in the decision-making process. However, this finding might be considered against research which suggests that, in practice, physicians often provide end-of-life care for patients, which differs from what they would choose for themselves.16,17 While the reasons for this are complex, they may stem from physicians’ desire to preserve patient trust, reluctance to extinguish hope, or systemic incentives toward treatment. It also raises important questions, such as: how does the emotional toll on physicians for providing care that is not in line with their own values impact clinical care? Is variability in practice a concern if physicians diverge in the extent to which they incorporate their preferences into their clinical practice? Could physicians frame guidance as the provision of their perspective while anchoring it in the values and goals of their patients.
It may also be that in striving to manage the interaction between personal preferences and clinical practice, some physicians are employing a skill called decentering, which is maintaining awareness of one’s thoughts and feelings and striving to view them as temporary and objective. 18 In this practice, thoughts and feelings are simply observations that can be accepted as they are, and do not define one’s self. 18 This technique was not specifically mentioned by physicians, but they may be doing this when revealing their own preferences, taking care not to impose their own hypothetical wishes. Decentering is not a simple practice, and the theme of maintaining integrity illustrates that physicians’ individual moral rules and guidelines are being considered, and some physicians are imposing limits on themselves. These findings must also be considered in terms of their implications for patients. Physicians’ personal preferences may not have a limiting effect on patients if physicians do not impose their preferences or they share them in a neutral way. However, a more concerning scenario could arise if a physician were to limit a patient’s choices due to the influence of their personal preferences.
In comparing our findings across physician groups and countries, we found that most physicians reported striving to separate their personal preferences from clinical practice. Some physicians face challenges doing so, which was particularly emphasized by Italian physicians. Since more Italian physicians also cited the maxim of “treating others as I would want to be treated,” it may be that a cultural or religious component is associated with this strong connection to personal preferences. Across all specialties and regions, physicians generally try to steer conversations back to patients’ priorities to minimize personal influence, which indicates consensus among physicians about the importance of maintaining patient-centered care. This is reflected in existing research that suggests physicians recognize the importance of limiting information that may bias the patient. 4 Physicians also highlighted the importance of aligning their personal values with their clinical practice. Italian and Belgian physicians especially identified assisted dying as a source of ethical difficulty or discomfort. This finding is in line with the literature that indicates more religious physicians and those confronted by requests for assisted dying may experience moral distress when providing care that conflicts with personal values.9,10 The finding that end-of-life discussions can be both professionally and personally enriching was particularly pronounced among palliative care physicians. This may be because palliative care physicians routinely encounter end-of-life scenarios and opportunities for meaningful connection with patients, which is confirmed by existing research. 19
Our findings are also largely consistent with what we learned from the PROPEL online survey, which was conducted alongside this qualitative study. 12 We found that nearly two-thirds of physicians consider their own end-of-life preferences when caring for patients, almost one-third believe the recommendations they make to patients are influenced by their preferences, and nearly a quarter of physicians believe it is appropriate to do so. Palliative care physicians, however, are less likely to let their personal preferences impact patient care. This is relevant for its clinical implications and is confirmed by the physician interviews. The survey also indicated that physicians often prefer less life-sustaining treatment for themselves than they recommend for patients, and they would opt for palliative sedation and assisted dying more for themselves than for their patients. We found culture, religion, practice type, training factors, and legislative environment influenced preferences. The results of this qualitative study reinforce our survey findings and add more depth to the connection between physicians’ personal beliefs and preferences and their clinical practice. It is noteworthy that physicians consider it somewhat inevitable that their personal values and preferences enter into clinical encounters. It is also essential to appreciate the methods used by physicians to maintain objectivity and preserve ethical integrity.
The division among physicians on whether to share their personal end-of-life preferences when asked by patients has potential implications for clinical practice, medical policy, and medical education. In practice, this lack of consensus may lead to variability in patient experiences and potential confusion about what constitutes appropriate guidance, particularly in emotionally charged end-of-life scenarios. From a policy perspective, the absence of clear standards risks leaving physicians without consistent frameworks for navigating the ethical tension between transparency and avoiding undue influence, which could in turn impact patient trust and autonomy. In medical education, these findings underscore the need for training that equips physicians to navigate these nuanced situations by teaching communication strategies that honor patient values, clarify available options, and acknowledge relational contexts, while also helping future physicians discern when, how, and if it is ethically appropriate to share their own preferences.
Another important finding of this study relates to the moral distress and professional discomfort physicians feel when asked to provide care that does not align with their ethical values. As with existing research, we found this discomfort is especially evident in cases where patients request treatment perceived as futile or assisted dying, which some physicians feel violates their personal or religious beliefs. 20 This may be the case for the Belgian physicians who reported difficulty or discomfort related to euthanasia requests. The complex emotions physicians experience are often influenced by their personal preferences and moral interpretation of clinical and personal experiences, which may also be shaped by their religious beliefs. This internal conflict may sometimes manifest as reluctance to engage in practices such as withdrawing life support or assisted dying. There is also a clear preference among physicians not to continue or initiate life-saving treatment for themselves, though this occurs often with patients 21 and presents another potential internal conflict. While the issue of patient autonomy is central, physicians strive to preserve their own ethical integrity, which can lead to internal discord.
Physicians’ reflections across Belgium, Italy, and Wisconsin illustrate how legislative environments shape both their internal reasoning and their clinical comfort with end-of-life decisions. In Belgium, where euthanasia has been legal since 2002, physicians described being frequently confronted with euthanasia requests and noted that this legal permissibility can nonetheless generate ethical discomfort or tension when such requests conflict with their personal values or relationships. In contrast, Italian physicians work within a context where assisted dying is not legally permissible, and this absence of a legal framework appeared to reinforce a stronger emphasis on moral integrity, particularly among those whose religious commitments directly informed their unwillingness to participate in life-ending practices. Wisconsin physicians, practicing in a state where assisted dying is likewise illegal despite decades of debate, described similar moral unease with requests for life-prolonging or life-ending interventions they perceived as misaligned with their values, but tended to frame their reasoning through a more pragmatic lens of maintaining professional boundaries and redirecting conversations back to patient values. These jurisdictional differences suggest that the presence or absence of assisted dying legislation shapes and greatly influences how physicians perceive and negotiate the boundaries between their personal preferences and their professional duties.
Cultural and religious influences further differentiated how physicians across the three settings reasoned about their role in end-of-life care. Italian physicians most explicitly invoked religiously rooted moral principles, sometimes grounding their orientation in the “golden rule” and emphasizing the importance of acting consistently with one’s conscience, particularly when they viewed certain practices, such as assisted dying, as fundamentally incompatible with their values. Belgian physicians also discussed the influence of personal and relational values, but the cultural normalization of euthanasia within clinical practice appeared to create a distinct form of moral negotiation, wherein the challenge lay not in the idea of euthanasia but in determining whether participation in a specific request aligned with their ethical integrity. Wisconsin physicians, operating in a culturally heterogeneous context, tended to focus more on managing personal–professional boundaries and mitigating the influence of their preferences in emotionally charged conversations. Despite these differences, physicians in all three jurisdictions described the ongoing struggle to remain aware of and manage the influence of their own beliefs, highlighting a shared cross-cultural tension between personal conscience, professional integrity, and patient-centered care.
This study indicates that end-of-life care is recognized by physicians as a rich environment for personal and professional growth, allowing them to form meaningful connections with patients, confront ethical challenges, and deepen their personal insights and compassion through difficult conversations. This underscores research that emphasizes the clinical significance of conducting realistic and compassionate end-of-life conversations, which enable patients to maintain their autonomy and dignity while enhancing their quality of life as they approach death. 22 These conversations need not merely be a way to convey medical information but are also an opportunity to engage with human beings confronting imminent mortality—an experience that can be transformative for everyone involved. 23
Strengths and limitations
A strength of our study is the qualitative design using purposive sampling of physicians across three jurisdictions representing varied legal and cultural environments, and the participation of three groups of physicians—general practitioners, palliative care physicians, and other medical specialists. Our preferred balance of physician groups was successfully recruited. By focusing on how physicians’ personal end-of-life preferences impact their clinical practice, we provide a much-needed addition to the current literature on physicians’ end-of-life preferences. The study had certain limitations. Although the final sample comprised varied physician groups from three countries, it was ethnically homogeneous. In addition, selection bias is possible, as the interview study may have attracted participants with a particular interest in end-of-life issues, resulting in a sample more likely to have reflected deeply on the topic.
Policy and practice implications
These study findings suggest several important policy and practice implications. First, to support physicians in managing moral conflicts and maintaining professional boundaries, clear clinical practice guidelines should help ensure that clinical recommendations are based on patient preferences rather than personal beliefs or biases, particularly in end-of-life care. Ethical guidelines can also support physicians in navigating complex decisions, such as those involving PAS, or euthanasia. Second, the promotion of consultation with local palliative care experts or palliative care training and end-of-life conversation training, which fosters a person-centered approach, could support physicians in managing the influence of their personal preferences on patient recommendations. Third, addressing cultural and religious influences on physician decision-making through cultural competency training could also be important, particularly in jurisdictions where strong religious traditions impact patient care.
Conclusion
This study confirms the connection between physicians’ personal end-of-life preferences and their clinical practice. While there is divergence with some physicians striving to keep a separation and others using their personal preferences as a guide, most participants stress the need to keep the patient’s priorities at the center of decision-making. These findings underscore the complex interplay between physicians’ beliefs and preferences, personal ethics, and patient autonomy, highlighting the nuanced decision-making process involved in end-of-life care. Further research is essential to ensure that the interplay between physicians’ personal preferences and clinical practice is understood well enough to inform policies and training that promote ethical, patient-centered decision-making at the end of life.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251413284 – Supplemental material for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study
Supplemental material, sj-docx-1-pcr-10.1177_26323524251413284 for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study by Sarah Mroz, Frederick Daenen, Sigrid Dierickx, Freddy Mortier, Ludovica De Panfilis, Luca Ghirotto, Toby C. Campbell, Luc Deliens and Kenneth Chambaere in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524251413284 – Supplemental material for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study
Supplemental material, sj-docx-2-pcr-10.1177_26323524251413284 for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study by Sarah Mroz, Frederick Daenen, Sigrid Dierickx, Freddy Mortier, Ludovica De Panfilis, Luca Ghirotto, Toby C. Campbell, Luc Deliens and Kenneth Chambaere in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524251413284 – Supplemental material for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study
Supplemental material, sj-docx-3-pcr-10.1177_26323524251413284 for How do physicians perceive and manage the influence of their personal end-of-life preferences on clinical practice and end-of-life decision-making with patients? An international qualitative study by Sarah Mroz, Frederick Daenen, Sigrid Dierickx, Freddy Mortier, Ludovica De Panfilis, Luca Ghirotto, Toby C. Campbell, Luc Deliens and Kenneth Chambaere in Palliative Care and Social Practice
Footnotes
Ethical considerations
The study protocol was approved by the medical ethics committee of the Brussels University Hospital, which acts as the central ethics committee (BUN: 1432021000562, September 29, 2021). Approvals were also obtained from the ethics committee in Italy (AUSL, Comitato Etico dell’Area Vasta Emilia Nord: 748EE93B, April 7, 2022). The other participating institution did not require formal ethics approvals.
Consent to participate
Participants signed a written consent form at each interview.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by internal funding from the Vrije Universiteit Brussel and Ghent University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets are available upon request. Requests may be addressed to the first author. Every request will be evaluated on an individual basis, and the ethics committee of the Vrije Universiteit Brussels will be contacted for approval before any sharing of participant-level data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.