
Abstract
Background:
Spousal loss is a profoundly challenging experience, often leading to heightened risks of anxiety, depression, and prolonged grief. In the context of cancer, bereavement is further complicated by the caregiving role and the emotional toll of anticipating the end of life. Palliative care plays a crucial role in alleviating suffering, with Continuous Deep Sedation Until Death (CDSUD) being one approach to managing end-of-life distress. However, the impact of CDSUD on the grieving process remains underexplored.
Objective:
This study explores the emotional trajectories of bereaved spouses about CDSUD, aiming to identify differences in grief experiences between those whose spouses received CDSUD and those who did not.
Methods:
From September 2022 to April 2024, 13 participants were recruited from French hospital facilities. They were divided into two groups: Group 1 (n = 7) spouses of patients who received CDSUD, and Group 2 (n = 6) whose spouses did not. Data were collected through online semi-structured interviews and analyzed using ALCESTE software.
Results:
Group 1 revealed two main themes: (1) Palliative Care, Sedation, and Disease History; (2) Grieving Process, Social Relationship Changes, Couple’s History, and Difficult Moments. Group 2 presented three themes: (1) Disease History, (2) Family Background, and (3) Final Hours and Care Team. CDSUD was associated with an abrupt loss, while in its absence, bereaved spouses described extended caregiving and heightened emotional distress.
Conclusion:
Bereavement experiences varied based on CDSUD usage, with implications for anticipatory grief and bereavement support. Both groups highlighted the need for enhanced support systems for grieving spouses.
Plain language summary
Losing a spouse is an incredibly difficult experience that can lead to sadness, anxiety, and long-term grief. This study looks at how a specific medical practice—Continuous Deep Sedation Until Death (CDSUD)—affects the way surviving spouses cope with loss. CDSUD is a method used in palliative care to relieve severe suffering in terminally ill patients by keeping them unconscious until they pass away. However, its impact on the grieving process of spouses has not been well studied. We interviewed 13 people in France who had recently lost a spouse to cancer. Seven of them had spouses who received CDSUD, while six did not. Their experiences were analyzed to understand the emotional effects of CDSUD. The results showed that spouses whose partners received CDSUD often felt the loss was sudden and abrupt. On the other hand, those whose spouses did not receive CDSUD experienced a longer, more gradual decline, with extended caregiving responsibilities. Both groups faced emotional challenges but in different ways. Our findings suggest that the way a loved one passes away can influence how their spouse grieves. This highlights the need for better emotional support for bereaved spouses, regardless of whether their partner received deep sedation or not.
Introduction
The loss of a spouse represents one of the most painful and destabilizing life events, often accompanied by intense psychological distress. Literature suggests that bereaved spouses are particularly vulnerable to developing anxiety, depression,1,2 and prolonged grief.3–5 This vulnerability is even more pronounced without adequate social and emotional support, such as psychological counseling, emotional guidance, and consistent communication with healthcare professionals, 6 increasing the risk of isolation, loneliness, and a forced redefinition of one’s identity and life purpose.
The grieving process becomes particularly complex when the spouse’s death is preceded by a long terminal illness, often requiring intense caregiving efforts from the surviving spouse.
Given these challenges, specialized medical support becomes essential in accompanying both patients and families through this process. In this context, palliative care is crucial. It offers an integrated approach to managing physical symptoms and provides psychological support to the patient and their family.7–13
Among the various strategies used in palliative care, palliative sedation (PS) plays a specific role when suffering becomes refractory to standard treatments.
PS is one of the approaches used in palliative care to alleviate unmanageable symptoms by inducing a controlled reduction in the patient’s level of consciousness. 14 PS can be proportional—this includes practices such as intermittent, light, or temporary (respite) sedation, which are commonly used to relieve episodic distress while maintaining patient responsiveness—or deep and continuous until death (Continuous Deep Sedation Until Death, CDSUD). 15
The intermittent, light, or temporary sedation follows best medical practices and clinical guidelines, is reversible, and is governed by general principles of palliative care.
By contrast, CDSUD induces a permanent loss of consciousness until. Furthermore, unlike euthanasia or Medical Assistance in Dying, which explicitly aim to hasten death,16–19 both proportional sedation and CDSUD align with the principles of palliative care by aiming solely to relieve refractory suffering without directly accelerating death.
However, the clinical use of CDSUD is not uniform and can vary depending on the underlying illness and trajectory of decline. It is primarily used in oncology to manage refractory symptoms such as severe pain and dyspnea. 15 In these cases, where the end of life is generally more predictable, family members may feel better prepared, although they often experience a prolonged period of anticipatory grief.7–10 In non-oncological diseases, however, the use of CDSUD is less clearly defined due to the unpredictable clinical trajectory of conditions such as heart failure or respiratory diseases. 20
Multiple factors can influence caregivers’ perceptions of CDSUD, including their level of involvement in the decision-making process, the quality of communication with medical staff, and the emotional and informational support they receive during and after the terminal phase. 21
Beyond clinical aspects, CDSUD raises important ethical and legal issues that vary according to cultural and regulatory contexts. In France, the Claeys-Leonetti Law (2016) defines CDSUD as a right for terminally ill patients. 22 The law establishes that CDSUD must be implemented, upon the patient’s request, when suffering is considered refractory to standard treatments and the patient’s vital prognosis is engaged in the short term (i.e., within a few hours to a few days). 23 Decision-making is, therefore, primarily determined by clinical and legal criteria. However, institutional culture, the ethical and relational stance of healthcare providers, and patient or family preferences may influence how and when the possibility of CDSUD is discussed and perceived, particularly regarding the interpretation of suffering and therapeutic obstinacy. 14 However, when legal conditions are met and the patient requests it, CDSUD must be implemented, as established by the Claeys-Leonetti Law (2016).
Therefore, the use of CDSUD does not necessarily indicate greater overall suffering compared to cases where it was not implemented but rather reflects the variability of end-of-life clinical practices. This aspect is crucial to understanding caregivers’ experiences, as it shapes how they navigate the end-of-life process and adapt to the loss.
In France, this legal framework has also contributed to a broader ethical and social debate—one that differs significantly across countries—on how best to support patients and their families during the final stages of life. For example, CDSUD is subject to more restrictive laws or ethical controversies in Italy, Germany, and the United Kingdom,14,24–27 potentially impacting therapeutic decisions and shaping how families perceive the dying process.16,28–32
Despite the recognized importance of CDSUD in end-of-life care, empirical research on its impact on the bereavement experiences of surviving spouses remains scarce. Previous studies, such as Ortega-Pacheco (2023), have examined broader issues related to deep sedation and euthanasia, 33 while research initiatives such as the UNBIASED study 34 have focused primarily on medical decision-making processes surrounding end-of-life sedation. Yet, the specific emotional repercussions for bereaved spouses in the context of CDSUD remain largely unexplored.
Accordingly, this study aims to fill this gap by examining the experiences of bereaved spouses, comparing two distinct groups: those whose partners received CDSUD, and those who went through the same process without this type of intervention or with other forms of sedation—such as intermittent, light, or temporary (respite) sedation, which are typically used to relieve episodic distress without inducing irreversible unconsciousness. The goal is to offer an in-depth understanding of the dynamics of grief in these delicate circumstances.
Materials and methods
This study presents preliminary results from AFTERSEDATIO, a longitudinal, multidisciplinary research study conducted in France since September 2022, with completion expected by December 2025. It examines the consequences of spousal loss due to oncologic disease and the use of CDSUD. Participants are interviewed at three distinct timepoints following the death of their spouse: 3 months (T0), 6 months (T1), and 12 months (T2). The current article presents cross-sectional findings based solely on data collected at T0, that is, 3 months post-loss.
Participants
Thirteen participants were recruited from nine hospital institutions across France, specifically from palliative care units, in collaboration with physicians and psychologists, between September 2022 and April 2024.
Eligible participants were individuals aged 18 or older, able to speak and understand French, free of cognitive impairment, and who had lost a spouse due to an oncologic illness after the initiation of palliative care.
The participants and their spouses were distributed across the nine institutions, though not evenly, as some centers contributed more cases depending on patient volume and staff availability.
Quarterly meetings were conducted with medical professionals to review the study’s progress, address potential concerns, and clarify methodological aspects, ensuring effective coordination. Physicians and psychologists identified potential participants who met the inclusion criteria, provided them with detailed information about the study, and obtained their informed consent. Once consent was granted, the first two authors (L.S., Y.C.), who conducted the interviews, contacted the participants to proceed with enrollment.
While some eligible individuals initially consented, a few declined participation before the study began (T0). However, all participants who analyzed interviews using ALCESTE remained engaged in the longitudinal study. Approximately 10% of participants discontinued their participation after the study began, primarily due to personal circumstances such as health deterioration or the worsening condition of a close family member.
The sample was divided into two groups: those whose spouses received CDSUD (seven individuals, Group 1), and those whose spouses received other forms of sedation (such as intermittent or light sedation) or no sedation at all (six individuals, Group 2).
Group 1 included more women than men (4 vs 3), whereas Group 2 exhibited an equal distribution of genders, with three men and three women. The average age of participants was 64 (ranging from 43 to 77) in Group 1 and 58 (ranging from 40 to 70) in Group 2. A significant proportion of both groups lived alone.
The average age of the deceased spouses in Group 1 was 67.7 years (ranging from 49 to 78), comprising four men and three women. In contrast, the average age in Group 2 was 59.7 years (ranging from 40 to 73), with three men and three women. A considerable number of spouses had succumbed to solid tumors, constituting 92.4% of the cases.
All sociodemographic data were obtained directly from participants during the interviews and are based exclusively on their self-reports and subjective recollections.
As this article presents preliminary results, the findings are based exclusively on data collected at the initial T0 timepoint, offering an early snapshot of bereavement experiences within the broader longitudinal trajectory.
Procedure
Participants were interviewed from September 2022 to April 2024. Two authors (L.S., Y.C.) conducted the semi-structured interviews online via the BBB platform of the University of Strasbourg. BBB is a secure online platform specifically designed to meet the University’s privacy and security standards and is approved by the University’s Ethics Committee. All interviews were audio-recorded and transcribed verbatim. No repeat interviews were conducted, and no field notes were taken during or after the interviews.
Both (L.S., Y.C.) hold PhDs in Clinical Psychology and are trained psycho-oncologists with expertise in grief and palliative care. They were mindful of their potential influence on the interview process and took steps to minimize bias, including acknowledging their professional backgrounds to participants and avoiding leading questions. The researchers held reflective discussions regularly to address potential biases that could influence data collection or analysis.
The interviews for Group 1 lasted an average of approximately 38.20 (SD = 12.42), while for Group 2, the average was around 47.44 (SD = 13.24; Table 1). The interviewers, experienced in psycho-oncology and bereavement, ensured a respectful environment attentive to participants’ emotional needs.
Sociodemographic data of participants and deceased spouses.

No interview transcripts were returned to participants for comment or correction to avoid re-traumatization and preserve emotional safety in this sensitive context.
Table 2 presents the guide that the researchers/psychologists used during the interviews.
Examples of questions from the guide used to conduct semi-structured interviews.

Data analysis
Interviews were transcribed and then analyzed using ALCESTE (Lexical Analysis by Context of a Set of Text Segments), which enables quantitative analysis of textual data. 35
ALCESTE, conceived in 1979 by Max Reinert (Jean-Paul Benzécri Laboratory, CNRS, Paris), segments text into Units of Context, comprising one or more consecutive sentences based on punctuation and significant word count.
ALCESTE then evaluates co-occurrences in the text, assessing the frequency and position of words using chi-square analysis. Following this, it extracts and presents word classes found in the text, ranking them in descending order based on their degree of co-occurrence and further hierarchically classifying them.
The lexical analysis performed with ALCESTE identified various word classes based on frequency and co-occurrence. However, these word classes were not final themes on their own. Following the lexical analysis, a thematic analysis using a qualitative approach was conducted to organize these word classes into broader themes that capture the participants’ emotional and psychological experiences. This allowed for a deeper exploration of the participants’ grief and coping strategies.
Even within each class, the words (and the extracts of sentences selected from the text) are presented according to a hierarchical classification of the co-occurrences.
Thematic analysis, following Braun and Clarke’s six-phase framework,36,37 was employed to interpret the data qualitatively: (1) familiarization with the data, (2) initial coding, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the final report.
The first two authors independently reviewed the data and conducted an initial round of coding. They then compared codes, identified discrepancies, and discussed their interpretations to refine the themes. A third researcher (M-F. B.) was consulted to reach a consensus when disagreements occurred. This collaborative approach was crucial for enhancing the themes’ reliability and identifying the most significant and relevant patterns in the participants’ narratives.
To enhance credibility, member checking was not employed due to the sensitive nature of the data and the inability to return themes to participants without risking re-traumatization. However, thematic saturation was assessed throughout the analysis, and it was determined that no new themes emerged in the final stages of coding. This indicated that data saturation was reached. Although the sample size was small—seven participants in one group and six in the other—saturation was deemed sufficient because the themes identified were consistent across participants, and no novel themes emerged during the final stages of coding. While a larger sample could have provided more comprehensive insights, the robustness of the findings was ensured through data triangulation across participants and researcher consensus.
The reporting of this qualitative study conforms to the COREQ (Consolidated Criteria for Reporting Qualitative Research) checklist 38 (see Supplemental File 1), ensuring transparency and rigor in study design and reporting.
Furthermore, integrating ALCESTE’s quantitative lexical extraction with qualitative thematic analysis offered a balanced approach, combining objective word patterns with interpretative depth, enabling a comprehensive understanding of participants’ experiences.
ALCESTE was chosen for its efficiency in extracting lexical classes and themes from large datasets, supported by its proven validity in previous studies.39–41
Results
As previously mentioned, the study sample was divided into two groups. Group 1 comprised seven participants whose spouses received CDSUD, whereas Group 2 included six participants whose spouses received either intermittent sedation (23.1%), light sedation (9.3%), or no sedation at all (18.7%). These group classifications, along with all related data, were based on participants’ narratives regarding the type of end-of-life care their spouses received.
Participants in Group 1 reported that CDSUD was administered exclusively to relieve severe and refractory physical symptoms, primarily intractable pain and dyspnea, in accordance with established clinical guidelines. In contrast, participants in Group 2 described sedation—when present—as being used intermittently or at low doses to manage episodic symptoms such as agitation or breathlessness, often portraying these interventions as reversible and compatible with continued interaction.
The duration of sedation also differed between groups: in most CDSUD cases, sedation was initiated within the final 24 h of life, with two instances beginning in the last 5 h. Only one case involved sedation lasting more than 48 h (see Table 3).
Participant-reported sedation characteristics, decision-makers, and interview duration.

Regarding the decision-making process specifically related to PS, participants in Group 1 generally perceived physicians as the primary initiators of CDSUD. In contrast, participants in Group 2 more often described themselves—or their families—as actively involved in the decision to accept or decline sedation.
Beyond these descriptive accounts, the thematic analysis identified two main classes of words for Group 1: Palliative Care, Sedation, and History of the Disease (Class 1); The Grieving Process, Reshaping Social Relationships, History of the Couple, and Difficult Moments (Class 2).
Three main classes were identified for Group 2: History of the Disease (Class 1), Family Background (Class 2), and Final Hours and Care Team Member (Class 3).
Building upon the lexical classes identified through ALCESTE, a deeper qualitative analysis was conducted to explore the experiential and emotional content of participants’ narratives. This interpretative process enabled the refinement of initial categories and, where relevant, the subdivision of themes into more specific subcategories, thereby enhancing conceptual clarity and analytical depth.
Table 4 presents the resulting thematic categories, which reflect both the lexical structure suggested by the software and the nuanced interpretation derived from close reading of the data. Representative quotations are included to illustrate each theme and support the coherence of the analysis.
Thematic categories, subcategories (Classes 1, 2, 3), and illustrative quotations derived from qualitative analysis.
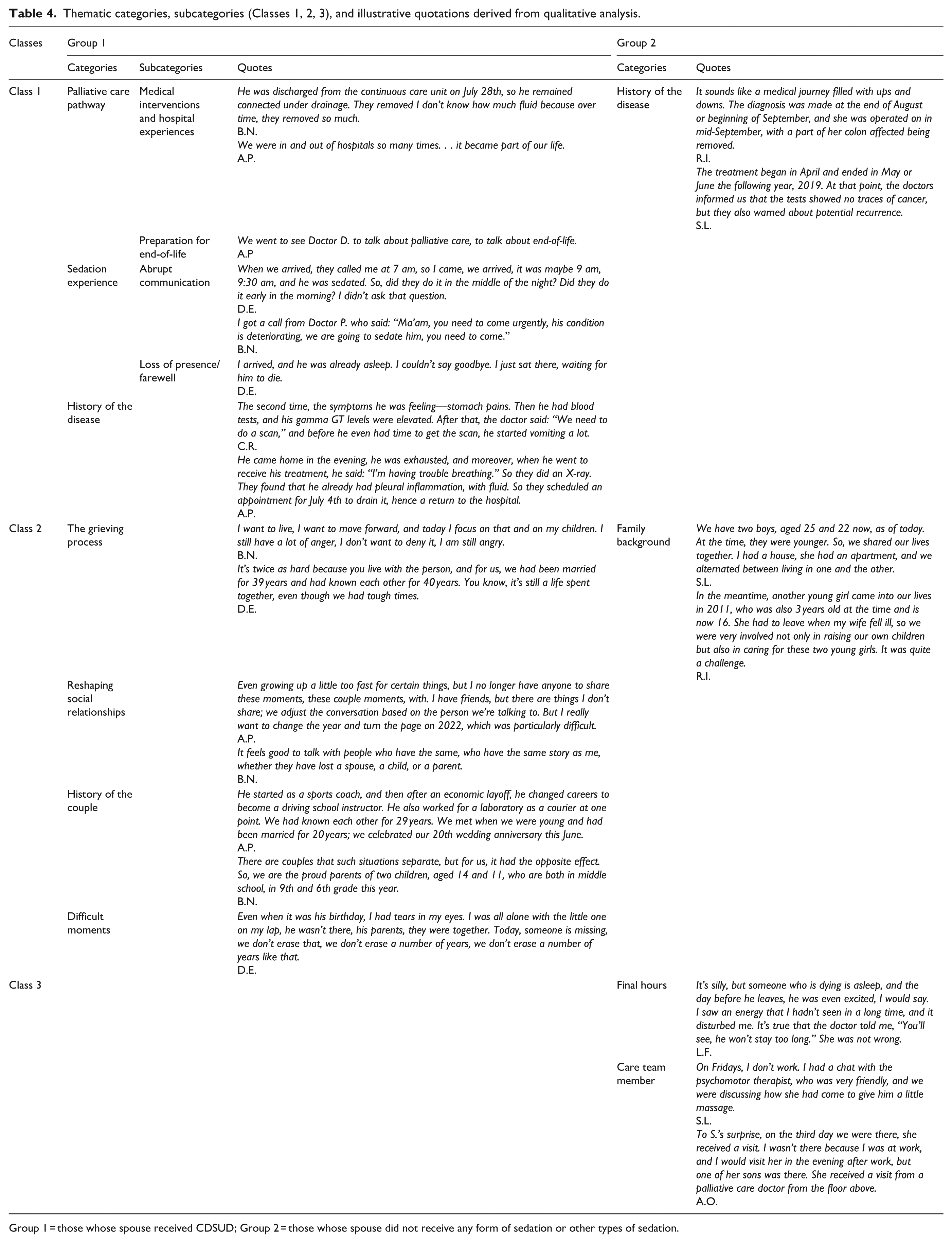
Group 1 = those whose spouse received CDSUD; Group 2 = those whose spouse did not receive any form of sedation or other types of sedation.
Group 1: Spouses of patients who received CDSUD
Class 1: Palliative care pathway
Palliative Care: Participants described their experiences navigating their spouses’ progressive illness and interactions with palliative care, including symptom management, care organization, and hospital trajectory. Subcategories included medical interventions and hospital experiences, and preparation for end-of-life. One participant said: “We were in and out of hospitals so many times. . . it became part of our life.” Another added, “We went to see Doctor D. to talk about palliative care, to talk about end-of-life.”
Sedation Experience: Participants often experienced sudden and emotional disruption during the implementation of CDSUD. This category includes the subcategories of abrupt communication and loss of presence/farewell. One spouse shared, “I got a call from Doctor P. who said: Ma’am, you need to come urgently, his condition is deteriorating, we are going to sedate him, you need to come.” Another added, “I arrived, and he was already asleep. I couldn’t say goodbye. I just sat there, waiting for him to die.”
History of the Disease: Participants detailed their partners’ trajectories, from initial symptoms and diagnoses to treatments and deterioration. One participant noted, “It started with fatigue. . . then came the tests, the chemo, the setbacks. . . I watched him disappear.”
Class 2: Grieving process and relational dynamics
The Grieving Process: Participants often described their grief as unresolved and prolonged, and in several cases, they linked this experience to the abrupt nature of their spouse’s death under CDSUD. A participant said, “I couldn’t tell him I loved him one last time. That haunts me.” In some accounts, the sedation was described not just as a medical act but as a symbolic point of no return.
Reshaping Social Relationships: Losing a spouse disrupted participants’ social and emotional worlds. “Since he died, I don’t talk to many people anymore. I feel invisible,” one said.
History of the Couple: The Spouses recalled their shared history with deep emotion: “We met in high school, built a life, a family. Now I feel like half of me is gone.”
Difficult Moments: Specific instances, like anniversaries or daily routines, reactivated grief. “Every Sunday, we had breakfast together. Now I can’t even go near the kitchen,” said one participant.
Group 2: Spouses of patients who did not receive CDSUD
Class 1: Disease trajectory
History of the Disease: Participants shared the ups and downs of their spouses’ illnesses, marked by moments of hope and disappointment. “She was better for a while. . . then the cancer came back. We knew it was serious this time,” one said.
Class 2: Family and relational dynamics
Family Background: Interviewees reflected on managing caregiving within family life. One participant noted, “Our children were amazing. We were all involved, taking turns, supporting each other. It brought us closer.” Participants in Group 2 often referred to the involvement of family members in caregiving roles, sometimes using language that suggested a shared experience.
Class 3: Final phase and support system
Final Hours: Many described a more peaceful and emotionally present end-of-life phase. “He was very tired, but he looked at me and said, ‘I’m not in pain, don’t worry’. That was the last thing he said,” recalled one spouse. Another shared, “She smiled at me. I kissed her forehead. We said goodbye.”
Care Team Member: The presence of compassionate healthcare professionals was repeatedly emphasized. “The nurse held my hand as he passed. I wasn’t alone,” said one. Another added, “The doctor explained everything. I felt supported, not just clinically, but as a person.” Participants highlighted how the quality of communication and support influenced their post-loss adjustment.
Discussion
This study shows how CDSUD is experienced not only as a medical intervention but also as a deeply relational and symbolic moment that can significantly shape the grieving process. The participants’ narratives underscore that when sedation is introduced suddenly or without sufficient communication, it can create a dual rupture: in the trust and communication between families and healthcare providers, and in the emotional continuity between families and the patient at the end of life.
In Group 1, CDSUD was often associated with an emotionally abrupt farewell and a disruption in the capacity to maintain presence at the end of life. This perceived difficulty may reflect the emotional weight participants associated with CDSUD, possibly due to its symbolic finality and the limited opportunities for final interaction. This aligns with prior research suggesting that a lack of anticipatory preparation can hinder the grieving process.42–44 Participants described grief marked by shock, unresolved emotions, and prolonged difficulty in adapting to loss.
Conversely, Group 2 participants often had the opportunity to witness a more gradual decline. Although both groups involved terminally ill patients, the timing and nature of sedation varied substantially. In Group 1, CDSUD was initiated only in the final hours or days of life, often with little time for interaction. In Group 2, intermittent or mild sedation was used earlier or allowed for continued consciousness. This distinction influenced participants’ ability to remain emotionally connected during the final moments. In Group 2, the absence of CDSUD allowed for ongoing interaction with the spouse and family involvement, often framing caregiving as a shared experience. These findings resonate with the notion of “relational continuity,” 45 where the ability to say goodbye or engage in final exchanges serves as a protective factor against prolonged grief.
Narratives of bereavement also differed in focus and emotional tone across groups. While Group 1 participants often expressed their grief in relation to the conditions surrounding CDSUD, those in Group 2 placed greater emphasis on caregiving and family dynamics. These differences may reflect variations in narrative emphasis rather than actual differences in the intensity or nature of the grief experienced.
Participants also emphasized the importance of being informed and emotionally supported throughout the dying process—particularly regarding how sedation was communicated (e.g., abrupt or compassionate), and the role of care team members in offering guidance and presence. Those who felt included and adequately prepared described smoother emotional transitions and greater resilience. These findings underscore the need for health professionals to foster clear, compassionate communication and to actively involve family members in the decision-making process, especially when sedation is under consideration. 46
Grief in both groups extended beyond emotional pain to affect identity and social functioning. However, spouses in the CDSUD group more frequently reported isolation and difficulty re-engaging socially.
Emotional preparedness, relational inclusion, and the quality of end-of-life communication are key mediators of bereavement outcomes. This aligns with existing literature on relational loss and prolonged grief,47,48 as well as systematic reviews showing that families’ emotional responses to sedation vary depending on how it is communicated and implemented.49–51
Such variability reflects a broader ethical and cultural ambiguity. Ortega-Pacheco (2023), for instance, examines the legal and ethical framing of CDSUD in France, 33 highlighting how it was established as a patient right under the Claeys-Leonetti Law (2016) as an alternative to euthanasia. While continuous deep sedation is practiced in several countries—such as Belgium, the Netherlands, and the United Kingdom—it is generally considered part of palliative care and regulated by clinical guidelines, rather than through specific legislation. Our findings suggest that, despite these legal distinctions, the emotional experience of CDSUD may blur with that of euthanasia for some families—especially when sedation is perceived as abrupt or poorly explained. Several participants described it as a definitive turning point, eliciting emotional responses that conflicted with its clinical intent to relieve refractory suffering, echoing Ortega-Pacheco’s concerns. 33
These insights also raise important ethical and cultural considerations. Several participants in the CDSUD group expressed a sense of exclusion or emotional unease related to the decision-making process, suggesting potential experiences of moral distress. This points to the need for shared decision-making, transparent communication of intent, and opportunities for families to express their concerns and values. Moreover, cultural attitudes toward death, autonomy, and medical authority likely shape how bereaved spouses emotionally interpret CDSUD. In France, the legal recognition of CDSUD as a right may provide a structured framework. Still, it may also carry symbolic weight that differs from countries where sedation is not legally distinguished from broader palliative care practices. These cultural and ethical dimensions should be further explored in future cross-cultural research. 52
Recommendations for clinical practice
Based on these findings, we recommend that palliative care teams adopt proactive communication strategies, including early, honest, and compassionate discussions with families about the potential use of CDSUD. Involving relatives in decision-making—when clinically and ethically appropriate—may reduce feelings of exclusion and emotional rupture. Healthcare professionals should be trained to recognize signs of moral distress in families and clearly explain the goals and ethical framework of sedation.
Communication between patients and spouses should be encouraged as early as possible—ideally during the first end-of-life conversations—so that both partners can express fears, hopes, and expectations. Palliative care professionals play a key role in supporting this connection and maintaining relational continuity, even in the final moments. It is also important to acknowledge that plans may not always unfold as expected. Preparing families for such uncertainty is an integral part of compassionate care.
Offering structured psychological support, such as anticipatory grief counseling and post-bereavement follow-up, can help mitigate the risk of prolonged grief—especially when sedation is introduced abruptly. These practices foster emotional preparedness, strengthen continuity, and support adaptive adjustment to loss.
Limits
His study has several limitations that should be acknowledged. First, the sample size was relatively small (n = 13), which limits the generalizability of the findings to the broader population of spousal caregivers in oncology palliative care. Although thematic saturation was reached, the limited number of participants may constrain the diversity of perspectives represented. Moreover, the qualitative nature of the study inherently restricts the extent to which findings can be generalized.
Second, the reliance on retrospective self-reports introduces the possibility of recall bias, particularly given the emotional intensity and temporal distance from the events described. However, this is characteristic of grief narratives, which are shaped over time and influenced by meaning-making processes.
Third, although the study focused on the impact of CDSUD, some form of sedation—albeit with varying intensity—was present in both groups. This introduces interpretive complexity and may contribute to thematic bias, emphasizing certain aspects of the end-of-life experience over others. Furthermore, we acknowledge two specific limitations regarding sedation categorization. First, the absence of a third group composed exclusively of bereaved spouses whose partners received no sedation reflects a structural limitation in palliative oncology. In clinical practice, it is uncommon for terminally ill cancer patients to receive absolutely no sedation, as even light or intermittent sedation (e.g., midazolam or morphine) is frequently administered to relieve distress. Second, our classification relied on participants’ subjective accounts rather than clinical records. Thus, their understanding of what constituted “sedation” may not fully align with medical definitions, introducing a layer of interpretive variability. In addition, demographic and clinical differences between the two groups—such as the higher average age in Group 1 and the greater severity of symptoms leading to CDSUD—may have influenced the nature of the dying process and, consequently, the bereavement experience. While these differences reflect real-life clinical trajectories, they should be considered when interpreting group comparisons. Moreover, the analysis did not deeply explore cultural and ethical dimensions—such as families’ moral perceptions, emotional responses to decision-making, or cultural attitudes toward end-of-life care—that may significantly shape how CDSUD is experienced. Future research should address these gaps by including more extensive and diverse samples, integrating quantitative measures to validate and expand findings, and possibly incorporating a third group exclusively composed of bereaved spouses whose partners received no sedation. This would allow for a more nuanced understanding of how sedation intensity interacts with grief and psychological adjustment. Finally, the perceived inconsistency of support described by some participants may reflect institutional differences, such as staff availability, workload, or organizational culture. These aspects were not analyzed in depth and warrant further investigation across varied care settings.
Conclusion
This study explored how bereavement experiences differ based on the use of CDSUD. Spouses whose partners received CDSUD often reported emotional disruption and unresolved grief, while those without CDSUD described greater relational continuity and a more gradual farewell. Across both groups, the quality of communication, emotional preparedness, and involvement in end-of-life decisions shaped the grieving process. These findings emphasize the emotional complexity of CDSUD, particularly when implemented suddenly or without sufficient explanation. Regardless of sedation use, bereavement remains a profoundly destabilizing experience requiring compassionate support. Palliative care teams should prioritize transparent, timely discussions about sedation options and provide tailored emotional support throughout the dying process. Enhancing relational continuity and recognizing individual needs can foster more adaptive grief responses. Future research should explore diverse settings and sedation practices to inform culturally sensitive and ethically grounded support strategies for bereaved spouses.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524251356301 – Supplemental material for End-of-life sedation and spousal grief: Exploring bereavement narratives with and without continuous deep sedation
Supplemental material, sj-pdf-1-pcr-10.1177_26323524251356301 for End-of-life sedation and spousal grief: Exploring bereavement narratives with and without continuous deep sedation by Livia Sani, Yasmine Chemrouk, Marthe Ducos, Pascal Gauthier and Marie-Frédérique Bacqué in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank our participants, the French hospitals helping us recruit bereaved spouses, and Mrs. Sandrine Amé.
Ethical considerations
The research protocol, which complied with Helsinki guidelines, was approved by the ethics committee of the University of Strasbourg on March 15, 2022.
Consent to participate
Participants provided informed consent before participation, and the collected data were anonymized.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the French National Cancer Institute (INCA_15908).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.