
Abstract
Background:
Over the next two decades, the numbers of people who will need palliative care in the United Kingdom and Ireland is projected to increase. Hospices play a vital role supporting people who require specialist palliative care input through community-based and inpatient palliative care services. Evidence is needed to understand the role of these different services to inform future service development.
Objectives:
To describe the reasons for admission, and outcomes at the end of the stay, for patients admitted to two hospice inpatient units (IPUs).
Design:
This was a mixed-methods study using a convergent, parallel mixed-methods design.
Methods:
We reviewed the case notes of all patients admitted to two hospice inpatient units from July to November 2019; conducted semi-structured interviews with patients and families; as well as brief structured interviews with inpatient unit staff.
Results:
Two hundred fifty-nine patients were admitted to a hospice IPU, accounting for 276 admissions in total. Overall, 53% were female; median age was 71 years (range: 26–95 years). Most patients (95%) were White British or Scottish, and 95% had a cancer diagnosis. Most patients were admitted from the community, under one-third were admitted from hospital. Most (85%) had previous palliative care involvement. Nearly, half had district nurse support (48%). Worry and anxiety was frequently reported as a reason for admission, alongside physical concerns. Median length of stay was 12 days, and 68% died during their stay. Hospice was recorded as the preferred place of care for 56% of those who died there.
Conclusions:
Sustained efforts to promote the hospice as place of care for people with conditions other than cancer are needed alongside greater clarity regarding of the role of the hospice IPU, and who would benefit most from IPU support.
Background
Palliative care can improve quality of life for patients with progressive advanced diseases and their families. 1 Most people are likely to benefit from a palliative care approach before they die. 2 Over the next two decades, the numbers of people who will need palliative care in the United Kingdom and Ireland is projected to increase significantly.3–6 Palliative care services designed to support increased demand need to be developed and evidence to support decisions relating to the settings in which palliative care is provided is essential.
Hospices play a vital role supporting people with an advanced progressive illness who experience complex symptoms and require specialist palliative care input. Much of hospice funding comes from the local community, and hospices offer a diverse range of services to meet the palliative care need of their local population. Across the United Kingdom, hospices typically provide community-based specialist palliative care support provided by palliative care clinical nurses specialists, doctors and allied health professionals; hospice inpatient care within a inpatients unit, for people who cannot be cared for at home, and a range of outpatient services including day therapies that offer psychosocial support and a variety of individual and group-based services (e.g. complementary therapies, rehabilitation, peer support groups, art and music therapy, etc.).7,8
Hospice inpatient units (IPUs) provide multi-disciplinary specialist palliative care to patients with complex palliative care needs. In the United Kingdom, there are 2760 inpatients beds for those patients who are not able to be cared for in their homes, accounting for 16% of the services hospice offer. 9 More specifically for Scotland, there are 14 hospices providing care and support for adults and their families, including 254 inpatients hospice beds. 10 People admitted to an IPU are treated for intractable physical symptoms alongside psychosocial concerns; or for end-of-life care (EOLC) where that is not possible in the person’s usual place of residence. In the United Kingdom, about 4%–5% of the population die in hospice IPUs.3,11
The demand for palliative care is projected to increase along with complexity of need. 3 A shared understanding of the role of hospice inpatient services, and who would most benefit is therefore needed. As a starting point, evidence on current usage, reason for admission, and outcomes of IPU stay would provide initial insights to inform decision-making on the role of the hospice IPU.
Methods
Aim
To gain insight and understanding of who is admitted to a hospice IPU, the reason for admission, the factors that contributed to the decision, perspectives on the care received and outcomes at the end of the stay.
Design
We conducted a prospective mixed-methods study using a convergent parallel mixed-methods design. 12 This involved bringing together qualitative and quantitative data, so that, they could be combined to generate a more complete understanding of the needs of those cared for in a hospice IPU
We undertook (1) case note review to gather information on the patients documented symptoms on admission, duration of admission, services accessed prior to admission, (2) face-to-face semi-structured interviews with patients (or family member as a proxy) to explore their experiences regarding IPU admission and (3) short-structured questionnaire for staff that could be administered either be face-to-face or left with them to fill out and send back to the researcher team, considering time restrictions. The questionnaire explored staff perspectives on the patient’s admission, and reasons for this.
Setting
Data were collected in two hospices in Scotland. Both hospices offered hospice inpatient services, community services, day therapies and outpatient clinics. At the time of the study, the hospices together had 50 inpatient care beds, with 20 beds in one hospice and 30 in the other and served a population of 870,000 people.
Quantitative data collection and analysis
Data were collected prospectively by a nurse researcher (MB) from case note review of all those admitted to the two IPUs over a period of 4 months between July and November 2019. Routine data were extracted using a standardised MS EXCEL form developed specifically for this study, to capture demographics, clinical characteristics, referral route and health and social care services in place, prior to admission and outcomes for each patient admitted to the hospice IPU. Quantitative data were imported from EXCEL into IBM SPSS Statistics, V24 and analysed descriptively.
Clinical data collected included:
Phase of illness
‘Phase of Illness’ describes whether the plan of care needs to change or not, based on changes to the patient’s condition. ‘Unstable’ indicates that the current plan of care needs to be radically and urgently developed. ‘Deteriorating’ indicates the plan of care needs to be adapted to reflect that the person’s condition is changing. ‘Dying’ notes that the plan of care needs to ensure all end-of-life measures are in place. ‘Stable’ indicates that the current plan of care does not need to be altered, although clearly being admitted to the hospice is in itself a change in the plan of care. 13 This is typically assessed by a hospice clinician, either a member of the medical or nursing team caring for the patient.
Adapted Karnofsky Performance Scale
The Adapted Karnofsky Performance Scale (AKPS) describes the patient’s functional status, with 100% being absolutely independent in all areas, and 10% being completely bedfast and unable to care for themselves. 14 This is typically assessed by a hospice clinician, either a member of the medical or nursing team caring for the patient.
Integrated Palliative Outcome Score
The Integrated Palliative Outcome Score (IPOS) describes the patient’s own assessment of their issues and symptom burden. If the patient is unable to manage, a staff member can complete the scale on their behalf. This is a self-reported 5-point assessment scale where a patient rates their symptoms over 10 physical domains, and seven psychological/spiritual/social domains leading to a maximum possible score of 68.15,16 This is typically assessed by a hospice clinician, either a member of the medical or nursing team caring for the patient.
Delirium status
Delirium status was based on the 4AT delirium assessment tool. 17 This is a simple and short (< 2 min) delirium detection tool designed for easy and effective clinical use. It does not require special training. The 4AT consists of four items and is scored from 0 to 12. A score of 4 or more suggests delirium.
Descriptive data
Descriptive data included primary diagnosis, ethnicity, age, gender and cohabiting status.
Service use data
This included ‘place referred from’, ‘reason for admission’, ‘health and social care services patients were receiving prior to admission’, ‘length of stay’ and the ‘outcome of the admission on completion of stay’ as if the patients died, was discharged to another service or discharged home.
Qualitative data collection and analysis
Patient and carer recruitment
All patients admitted to a hospice IPU during the study period were considered for inclusion in the qualitative study, with those patients who were actively dying, or were considered by staff to be extremely distressed excluded. A convenience sample of 22 patients was sought for face-to-face semi-structured interviews. Carers were included as a proxy if the patient was too unwell to participate. MB, a palliative care nurse with many years of experience, was given training and support in carrying out qualitative interviews by AL an experienced qualitative researcher. MB sought support from the ward-based staff before making any approach on day 1 or 2 of the patient’s admission. Written information about the study was shared with the patient, or with their family if they lacked capacity to take part. Before agreeing to take part, participants were able to have questions answered by MB. Written, informed consent to participate was obtained from all patients and carers prior to inclusion.
Health Care professional recruitment
For those patients interviewed, we also sought to recruit the health care professional that carried out the admission to offer their perspective in a semi-structured face-to-face interview. The referring health care professional was also invited to complete a brief structured interview giving the reason for referral, what they believed the patient’s preference was for their place of care and if this was to stay at home what could have facilitated this choice. Written information about the study was provided, and written and informed consent to participant was obtained prior to inclusion.
Data collection and analysis
Brief interviews with patients’ carers and admitting clinicians took place in the hospice during the study period of July–November 2019. All interviews were transcribed verbatim with anonymity ensured by removing identifiable place and allocating anonymous identifiers in place of names in the transcripts. Structured interviews with the referring clinician took place by telephone to clarify the context surrounding the admission.
Data were grouped according to each patient as the central case with information from professionals linked to their admission. This allowed a broad understanding of the reasons for each admission and for convergent or divergent views to emerge. Qualitative data from interviews and case were analysed using thematic analysis by AL and reviewed by EH. 18 Themes were developed and refined inductively, through re-reading the transcripts. These were then discussed with the wider team. Initial coding was carried out using NVivo12. The research team agreed the data gathered was sufficient to answer the aims of the study.
Governance and ethics
The South East Scotland Research Ethics Committee (SES REC) confirmed that ethical approval was not required for this ‘service evaluation’. The research was reviewed by the hospice research governance groups with all methods performed in accordance with the relevant guidelines and regulations.
Results
Overview
During the study period, there were 259 patients admitted to a hospice IPU, accounting for 276 admissions in total as some people were admitted more than once 126 admissions were to site 1 and 150 admissions to site 2. Overall, 53% were female; median age was 71 years, with ages ranging between 26 and 95 years. The characteristics of those admitted are outlined in Table 1.
Characteristics of patients admitted to two hospice inpatient units over 4 months.

A total of 22 semi-structured interviews were carried out with a patient/relative and lasted on average of 15 min. In addition to this, eight health care professionals who had referred the patients to the IPU and 11 health care professionals who had admitted the patient answered structured interview questions either face-to-face or by written pro forma Characteristics of patient or relative proxies interviewed and additional interviews are outlined in Table 2.
Interview participants – patients and carers (N = 22) and additional structured interviews.
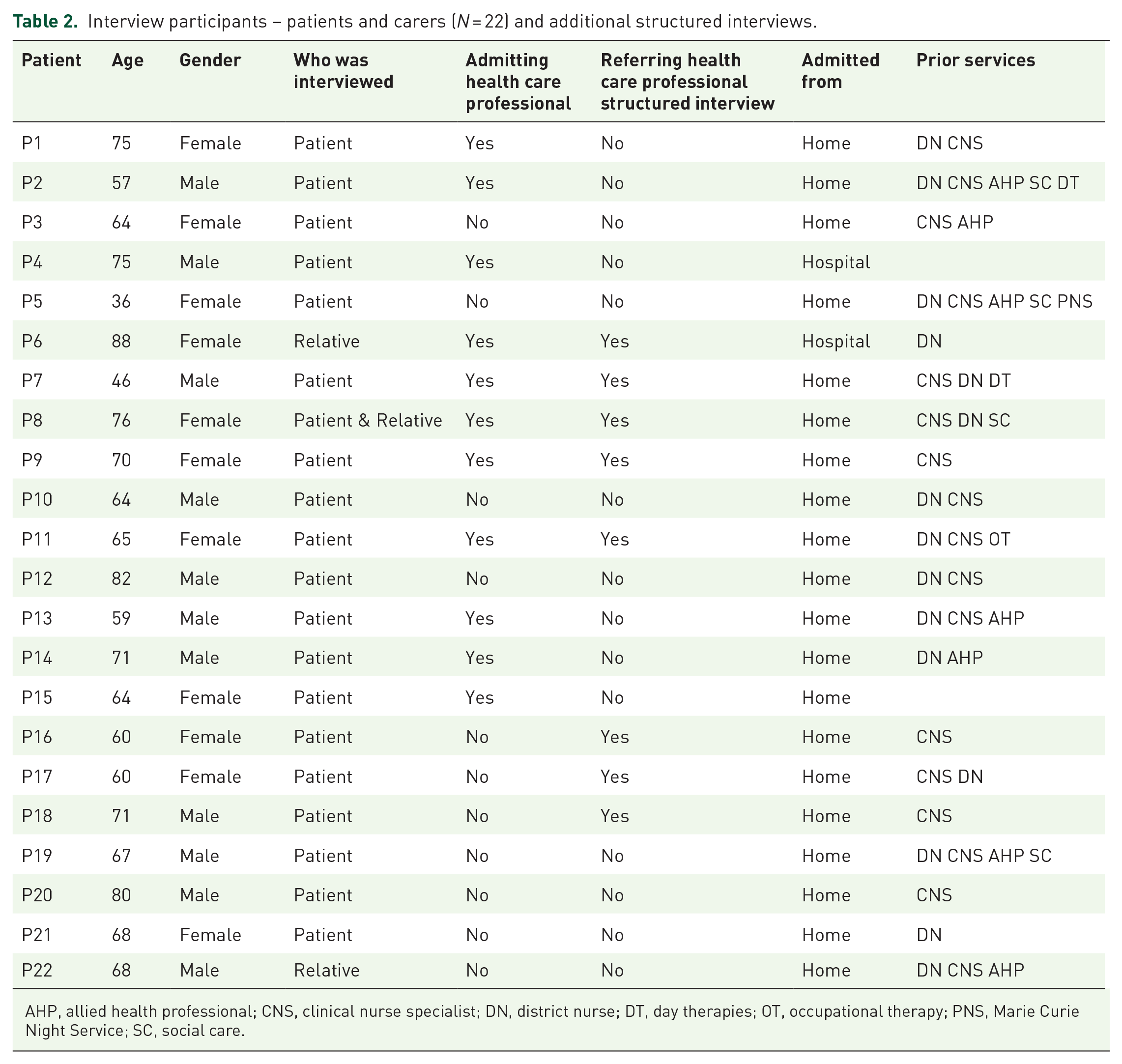
AHP, allied health professional; CNS, clinical nurse specialist; DN, district nurse; DT, day therapies; OT, occupational therapy; PNS, Marie Curie Night Service; SC, social care.
In the following sections, we synthesise both quantitative and qualitative data relating to three general areas: (1) description of patients on admission to hospice IPU, (2) circumstances and support prior to admission and (3) outcome of admission.
Description of patients on admission to hospice IPU
Diagnoses
The vast majority of patients (95%) had a malignant condition as their primary diagnosis. The most common diagnosis was lung cancer (52/259 patients; 20%) followed by breast cancer (21/259; 8%). The most frequently seen non-malignant conditions were pulmonary fibrosis (four patients; 1.5%) and cardiac failure (four patients; 1.5%).
Phase of illness and delirium assessment
Phase of illness data was recorded during 238 admissions (Figure 1). 33% of patients were assessed as unstable (n = 79), 35% as deteriorating (n = 84) and 5% as dying (n = 13). The remaining 27% (n = 62) were assessed as stable (Figure 1). Overall, 28% screened positive for delirium; and a further 14% had possible cognitive impairment.
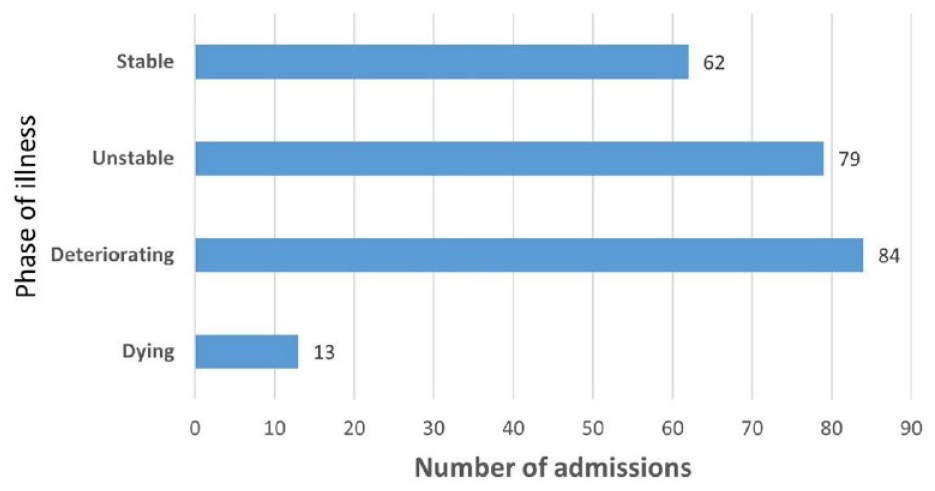
Phase of illness (N = 238).
Performance status
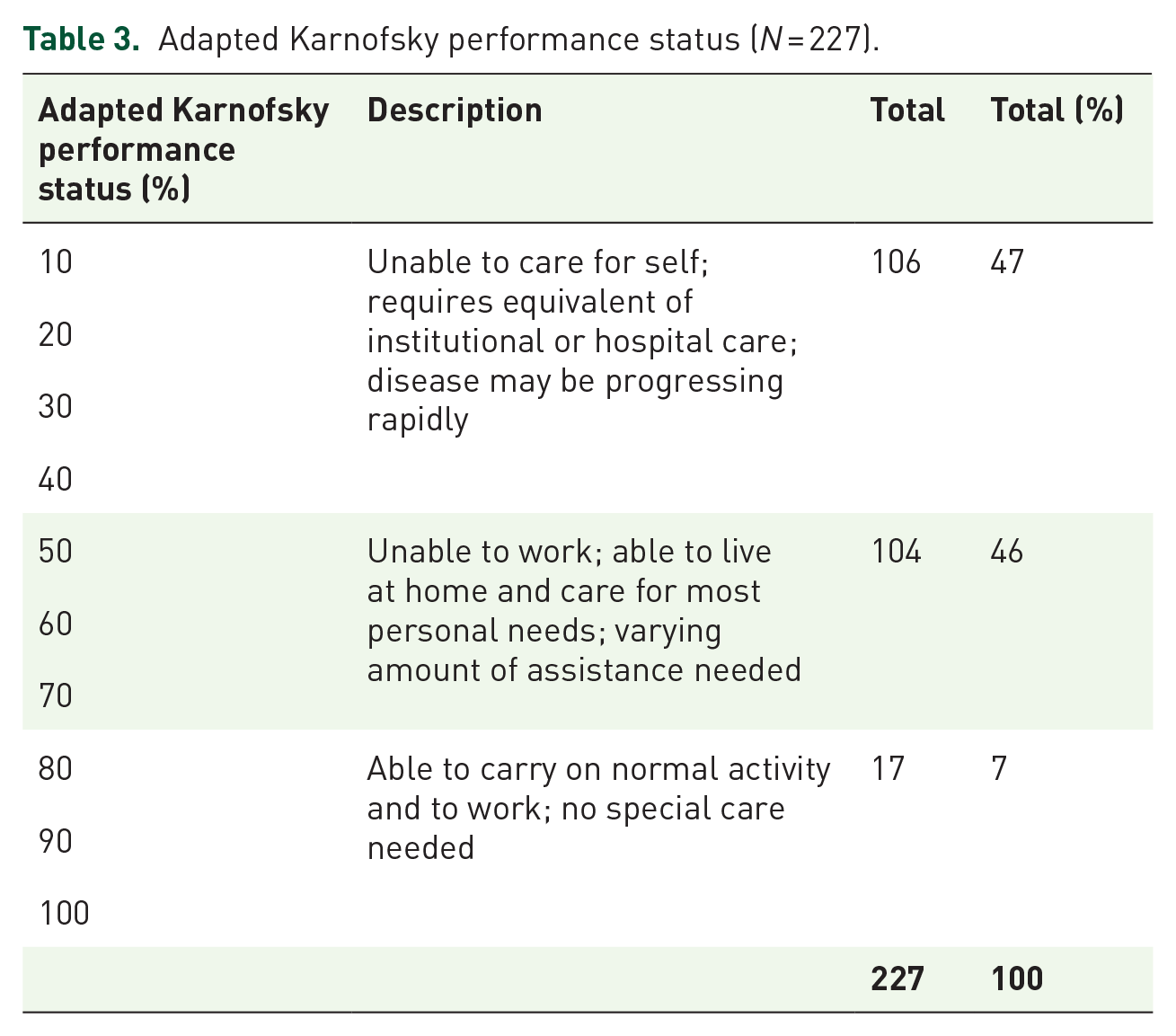
The adapted Karnofsky performance status was recorded during 227 admissions; 47% were in the lowest performance category of being completely unable to care for the self, with 46% in the middle range and thus requiring some assistance with their day-to-day care. The remaining 7% were those who were still able to care for themselves (Table 3).
Adapted Karnofsky performance status (N = 227).
Palliative care concerns
IPOS scores were documented during 78 admissions (28% of all admissions). The issues that patients identified as the most concerning for them covered a wide range. However, the most prevalent was their belief that their family were worried about them, closely followed by feelings of weakness/lack of energy and poor mobility (maximum possible score for each domain is 4). Pain was also a commonly expressed issue, as was distress and lack of peace (Figure 2).
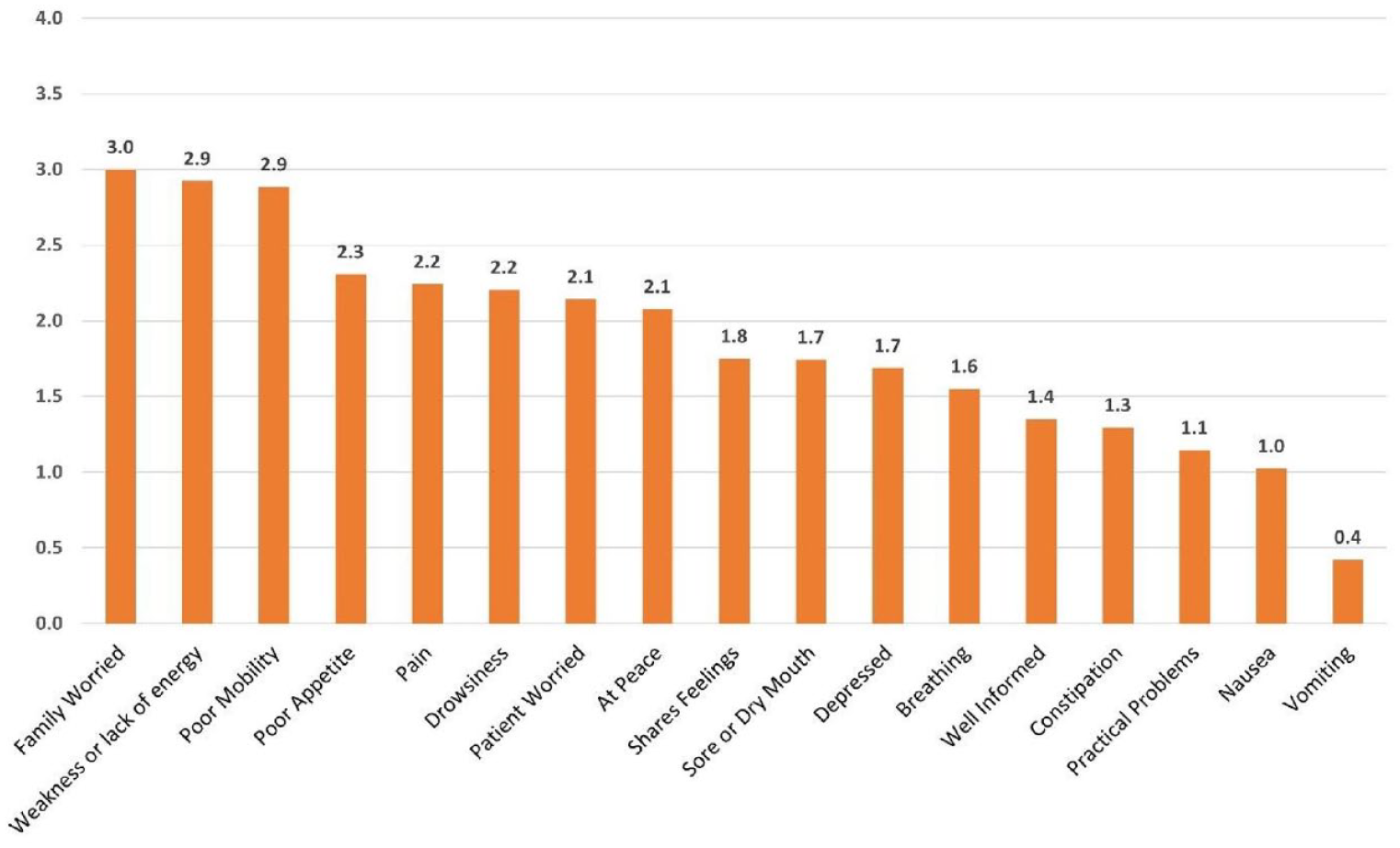
IPOS scores on admission (n = 78 admissions).
Reasons for admission
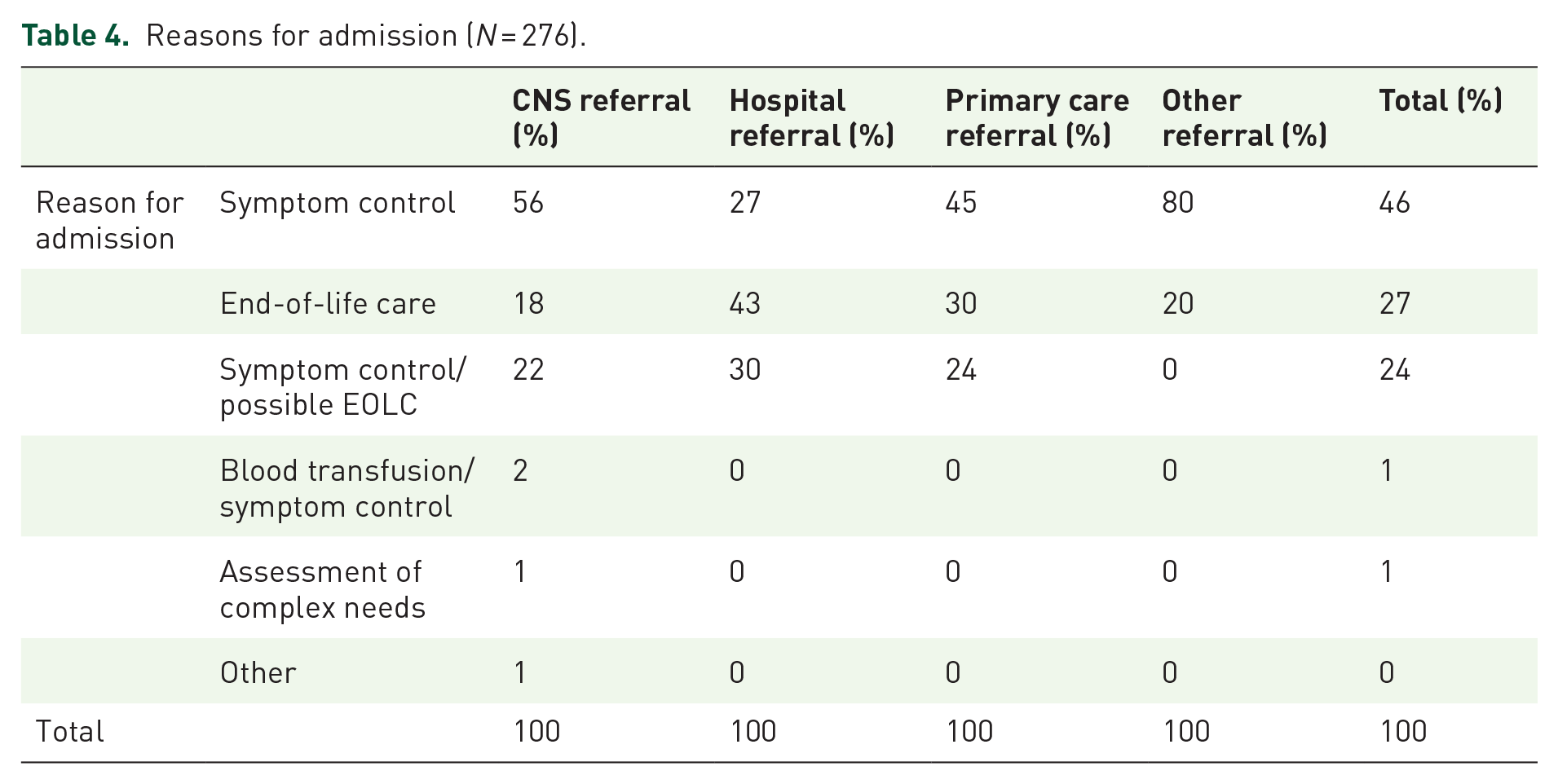
Reasons for admission identified by the referring clinician in case notes were symptom control for 46% of patients, EOLC for 27% and both symptom control and EOLC for 24% of patients. Admissions from home were more likely to be for symptom management, whereas admissions from hospital were more likely to be for EOLC (Table 4).
Reasons for admission (N = 276).
The thematic analysis of the qualitative date provides further insights into why people were admitted to hospice IPU. The main reasons that were given by patients or family members and those that admitted them were symptom control, anxiety and fear, social isolation or EOLC either through the wish of the patient or because the family were struggling to cope. These themes clearly overlap and interact although were evidenced as follows.
Symptom control
As demonstrated in the quantitative data, control of physical symptoms was a prominent reason for admission. These included pain, shortness of breath and nausea. The following quotes detail patient views of these admission reasons, which were echoed by admitting staff members in qualitative interviews.
P2: ‘just constantly hiccupping all the time, and throwing up, severe stomach pains’ ‘I just physically deteriorated’ ‘They ahhh doubled up that medicine but even that didn’t work’. ‘I wasnae gonna say no [to coming into the hospice] cos there’s no better place to be like for like pain relief and that, [you know], press a wee button, and get pain relief if you’re feeling sick, [you know] press a button, cos I was having tae phone up the nurses on the emergency, [you know] on the after house line for them to come out and give me anti-nausea’. P17: I was put on medication for nausea and dizziness and I’ve still had problems so that’s the reasons I’ve ended up in here. It was to sort it out regarding the dizziness, breathlessness and just general fatigue.
Anxiety and fear
Qualitative interviews showed that anxiety and fear also played a prominent role in the decision to go to the hospice. Patients and family members articulated fears of struggling to control symptoms. However, these could become more general anxiety and fear perhaps to the point of existential anxiety. Staff members could recognise this more readily.
P14: If I’m just here at home – I can’t cope with things. I um get a bit anxious in terms of being on my own and something happening. P14 staff: I think he’s very frightened. He lives alone and the symptoms that he’s experiencing now; though they don’t appear to be very severe at present; he felt that things couldn’t get any worse for him and that he is dying’. ‘He was frightened and didn’t appear to be managing anymore. P22 wife: AS soon as the breathing thing happened, that was the change in him. And he was like-I can’t breathe. But some of it I think was mental’ ‘But he started to go into almost like a panic mode. P22 staff: So for somebody like him I think it’s an anxiety type thing and it’s comforting for him to be in this situation rather than the hospital.
Social isolation
Social isolation was an issue that compounded other issues, including anxiety and physical symptoms. These issues are best illustrated by giving a greater degree of context through a patient’s story. The story of P9 illustrates the interaction between psychological aspect and practical elements of social isolation. Living alone made it more difficult to cope with unexpected problems and also perhaps, amplified fears of symptoms that may come with dying. For this patient, having people care for her in her home was something that she could not accept.
P9: So I did tell the Marie Curie nurse I did want to come in – cos I didnae want, didn’t want people coming into the house looking after me or my sons finding me in a disgraceful situation you know what I mean? So that was the reason for [admission to the hospice].
She had experienced being weak and unable to help herself during the night and her distress at being without help at this time, and so that, admission to the hospice alleviated much of this anxiety.
P9: I feel like I’m a lot happier now I’m here, and quite settled on going, you know what I mean.
Once in the hospice she was able to allude to other fears that being admitted must have alleviated as she discussed her wishes for medication.
P9: ‘I don’t want to be screaming out in pain, you know what I mean, so I’m ready to go now’. ‘I said I’ll just drift then one day you’ll no be able to get me round, And that will be that. Another dose of morphine’.
Social isolation could affect a patient’s ability not only to stay at home but also on their capacity to cope with symptoms meaning that it could be difficult it to unpick the impact of social situation from disease progression and physical symptoms.
P2 Staff: ‘[his] situation as well, isolation, just yeah, I think [he’s] deteriorated a bit and a bit more fatigued I think [CNS] were worried that ‘is [the patient] tipping’ or ‘[is he] deteriorating’ but not clear, so just needing a little bit of assessment and a little bit of time here to see where [he] is at, ‘how much of it is social circumstances versus cancer progression’ ‘so rather than trying to struggle at home, and getting syringe drivers and things at home actually coming in is the preference’.
End-of-life care
Patients were also admitted to the hospice explicitly for EOLC. It was, at times, the wish of some patients to be admitted for this reason again directly echoing the quantitative data.
P14: I’ve known about this now for a long time. I’ve known this was terminal for a long time. So it’s allowed me to have conversations and make plans and all that kind of thing. And particularly my son and daughter, and I said to them ages ago: ‘when I die I’d far rather die at the hospice than alone, so yes’.
At other times, the family/carers simply were not able to cope with the level of EOLC needs.
P6 carer: ‘she was becoming iller and iller and we were having to give her morphine and having to administer morphine and we hadn’t anticipated that, we didn’t, we thought naively I think, I never realised naively we thought we’d get a lot of support at home from DN teams and to be fair to the district nurses when you call, they do come but it can take an hour or two so it’s not immediate and eventually we were not able to control her pain’. ‘She was getting less and less able to move, to walk’ ‘she started to have a reaction to the morphine which she was given, and she started to become paranoid and quite agitated’. ‘The Tuesday and the Wednesday she started to be really sick, so she was projectile vomiting and she was bringing up bile so that was quite alarming and upsetting for her, then they had to put a line up her nose to deal with the bile’.
Support prior to admission
Source of referral
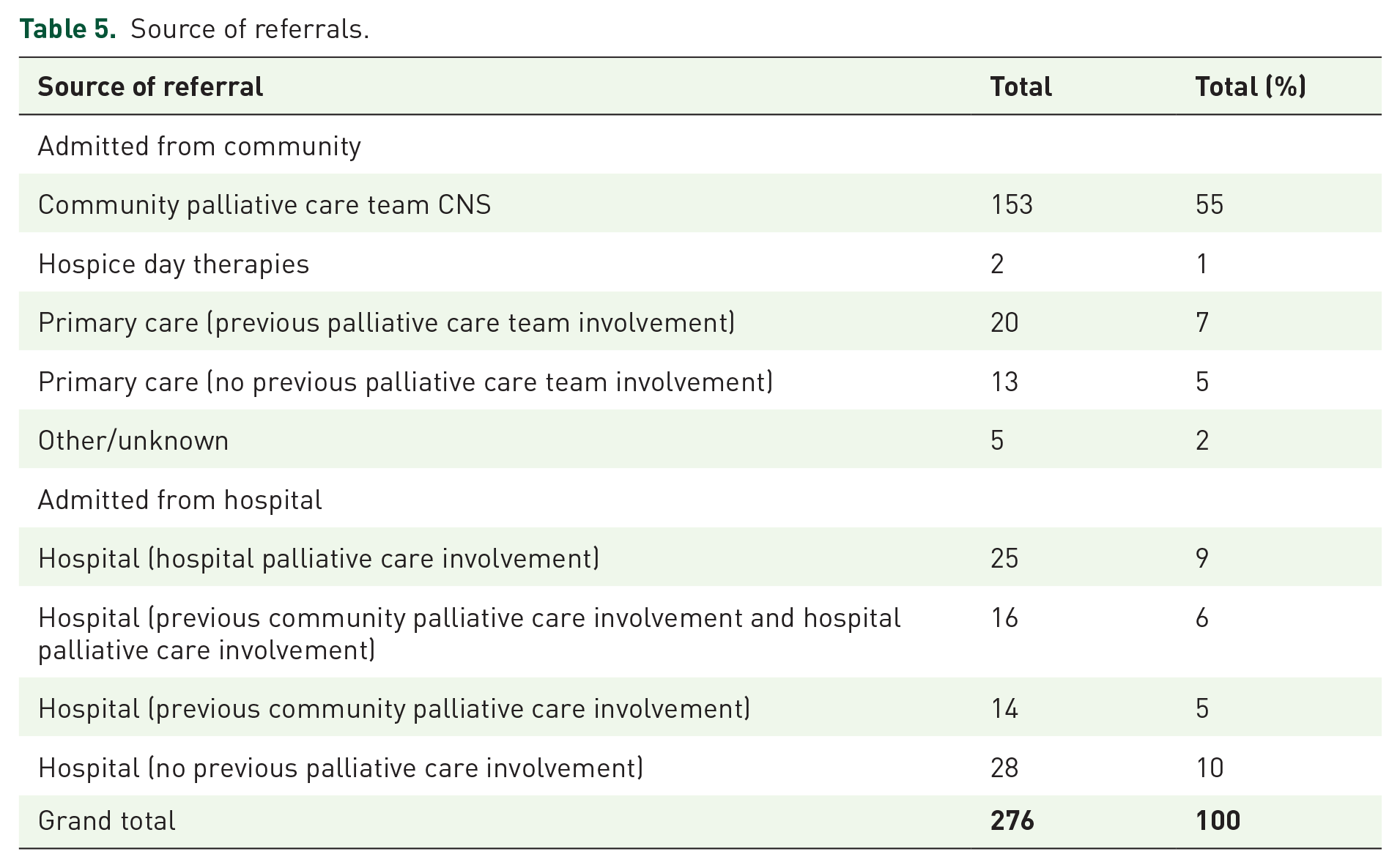
The majority of admissions to the hospice IPUs came from the community (70%, n = 193). Over half of all those admitted were referred by the Hospices’ Community Specialist Palliative Care teams (56%). 12% (n = 33) of admissions from the community were referred to the hospice by primary care. Nearly all those referred to a hospice IPU from the community had previous palliative care team involvement. Just under a third of admissions were directly from hospital (n = 83) with most having previous palliative care involvement (Table 5).
Source of referrals.
Support in place prior to admission
People came to the hospice IPU having had involvement from a wide range of services most notably 73% having input from a Community Clinical Nurse Specialist (CNS). Nearly, half of patients (48%) had input from district nursing and a third (33%) from allied health professionals, such as physiotherapy or occupational therapy. Other service involvement included social care services and specialist Marie Curie Overnight Nursing Care as detailed in Table 6.
Resources accessed prior to admission.

The qualitative analysis provided more in-depth data on the support, which was in place at home when patients were admitted to the hospices. This highlighted various support that was in place generally appropriate although not always effective in terms of actually meeting individual needs in a person-centred way. A more tailored approach was needed to meet specific needs, as illustrated in the examples below.
P19 brother: I was explaining that the carers weren’t coming in. He’s got tablets he’s on every 6 hours and it’s they’re coming in at 11 then at 4 then 8 which is no 6 hour gap. P5 patient: lots and lots of different people and I didn’t know the people, I met so many people and I was tired all the time and it was becoming problematic because I needed just a few people to do it. Interviewer: So you had some people that were kinda coming in, your carers, were they quite regular at coming in? P5 patient: ‘Yeah they would always [come], they were supposed to have 4 [carers], but they always [rushing you], really quickly, they didn’t want to do problematic things’ ‘they were always asking [me] “what you’ve got to do?” and what and I was tired’
Outcome of admission
Discharge or death
The median length of stay for those admitted to the IPUs was 12 days (mean was 17 days). This was shorter for those who died during their admission at an average of 9 days compared with 17 days for those who were discharged. Overall, over two-thirds, (68%, n = 188) of those who were admitted died during their stay while 31% (n = 87) were discharged. One patient was still receiving care in the unit at the end of the data collection period.
Eighty-six percent of admissions from hospital were for patients who died in the IPU during their stay with 14% being discharged. Seventy-three percent of admissions from primary care were for patients who died in the hospice IPU during that stay. Of those admitted via the Community CNS team 58% died and 52% were discharged. The majority (80%, n = 70) of those discharged were discharged to their home with the remaining 20% (n = 17) being discharged to care homes, hospital or community hospital.
Patient preferences for place of death
A preferred place of death was recorded during just over two-thirds of admissions. The hospice IPU was the documented preferred place of death for 56% who died in that location (Table 7).
Last recorded preferred place of death for those who died in the hospice inpatient unit.

While for majority of the patients wanted to die in the hospice, there remains a great deal of stigma about the terms hospice and palliative care. This was evident in how people had considered the hospice prior to admission. However, fears could be countered by reassurance from hospice staff or experience of being in the hospice.
P1: ‘when you hear a hospice – It’s full of people that’s dying, that is what I thought’. ‘[nurses] told me what a nice place it was and how the nurses were great and I wasnae coming in to die I was coming in to get help’. ‘I had to get it in my head that I wasn’t coming in here to die’. ‘I’m quite confident now and not half as scared as I was’. P17: [I was scared] because of my perception of a hospice. That you never get out. And that they’re cold places but I found that to be entirely the opposite situation. I find it – I mean I’m on a nice wee ward here, its very quiet. I told the CNS about [my daughter’s] baby and she says well if she does have the baby while you’re in, you can go. Which I didn’t know. Yes so that was encouraging.
Any level of familiarity with the setting was helpful for this. If a patient had been in a hospice before or had experience of visiting someone in the hospice, then they were more well-disposed to coming in. Familiarity reduced fear and anxiety.
P21: ‘a friend of mine who had Motor Neurone Disease was in here a couple of years [ago] for respite – well maybe three years ago. For respite care and it was lovely you know’. ‘[aunt] was so well looked-after here that she felt safe’.
Once admitted to the hospice, people described their experiences of hospice care in very positive terms.
P1: I’d just be sitting at home right now in pain and knowing that nobody could get on top of it. Where I’m here I’ve got to take because they are trying to get my bowels to move, but I’m not in pain, I’m quite comfortable lying here. P4: It’s not something I wanted but it’s been an ideal choice so far, good choice, no one wants to be anywhere where you are sick and [not] getting better, but eh, yeah, the hospice has been good.
Discussion
This rigorous service evaluation study found that, over a 4-month period, the vast majority of people admitted to two Scotland-based hospice IPUs had cancer; over two-thirds were admitted from the community; most had community palliative care CNS input prior to admission; and nearly, half had district nurse support. Nearly, all (95%) were White British, which is reflective of the population of Scotland as a whole. About half were admitted for EOLC or possible symptom control/EOLC. Patient concerns rated most highly across all patients were worry and anxiety, weakness and poor mobility. Median length of stay was 12 days. Mortality was high with over two-thirds of patients dying during their admission, reflective of the advanced stage of illness experienced by those admitted.
Our finding that nearly all patients admitted to two hospice IPUs had a primary diagnosis of cancer (95%) is a higher proportion than reported in other related studies. 8 In a mixed-method study of all patients referred to community and inpatient services at four UK hospices 87% had a primary diagnosis of cancer. 8 In a national retrospective cohort study involving 64 UK hospices, Allsop et al. 7 found that 77% had cancer and 20% had a non-cancer diagnosis. Our study reflects findings from other studies highlighting those patients with non-cancer diagnosis are less likely to access palliative care and hospice services. In a cross-sectional post-bereavement survey, Kasdorf et al. compared health care experience of patients with cancer and non-cancer diseases in their last year of life in Germany. They found that patient with non-cancer diagnosis were disadvantaged when it came to access to palliative care services. 19 Moens et al. 20 in a literature review highlighted while non-cancer patients have the same symptom burden as cancer patients, they are less likely to be considered for palliative care and hospice service.
The present study is the first to focus specially on the hospice IPU and suggests that the proportion of people accessing inpatient hospice services may be very low for people with conditions other than cancer. This may be because they are less likely to be referred for specialist palliative care, or that their palliative and EOLC needs are sufficiently met via disease-specific community-based services. Challenges associated with increasing access to palliative care support, including specialist support, for people with non-malignant disease have been documented. 21 These include greater uncertainty in their illness trajectories and challenges in identifying a terminal stage. However, our findings, that so few people with non-malignant conditions accessed IPU support in two hospices, suggest that inpatient specialist palliative care support for people who do not have a diagnosis of cancer may be very limited.
Most patients admitted to hospice IPU were unstable, deteriorating or dying and had low physical functioning. Over two-thirds died during their admission. Thus, a significant majority of IPU admissions were for EOLC – even a higher proportion than initially expected based on ‘reason for admission’ initially documented by clinicians. Most hospice IPU patients were approaching the end of life; and the care provided was focused on symptom management and holistic support in the last days and weeks of life. Interview data revealed inadequately managed physical symptoms as the main reason for admission but also highlighted future fears and anxieties relating to struggling to control symptoms or of imminent death. This contributed to increasing existential anxiety for themselves and their family members, leading to a lack of sense of emotional safety at home. Living alone also made it more difficult to cope with unexpected problems, again amplifying fear of symptoms and imminent death. Previous research has shown that loneliness often accompanies dying; this may be social loneliness due to a loss of role and decreasing networks; emotional loneliness due to lack of an attachment figure and existential loneliness when people have great difficulties expressing their concerns as death approaches. 22 The hospice IPU provided a safe alternative setting where patients could be cared for in a supportive setting, and where physical symptoms, loneliness and fear and anxiety associated with death and dying could be better managed.
Admission to hospice IPU is inadequately explained by physical symptoms alone. Rather our findings suggest that dynamic personal, social and service-level contextual systems were interlinked and interdependent. For example, increasing the level of community input may not be enough to support an individual at home where the social or family system is struggling due to fear and anxiety around impending death or uncontrolled fluctuating symptoms. Similarly, an individual may be managing at home with family support to a point where physical deterioration or anxieties build and increased community input may be needed to prevent overburdening.
The cumulative and progressive nature of symptoms and functional difficulties over time strongly impact on the ability to cope. 23 Some patients in this study reached a point of becoming overwhelmed by various struggles where they began to lose a sense of emotional safety, thus leading to hospice admission that was often described as a last resort. By considering total pain or overall burden, clinicians may be able to identify those at increasing risk of becoming overwhelmed and instigate appropriate coordinated support to prevent or delay admission if this is preferred. Certainly, for those who had a preferred place of death ‘documented’ and subsequently died during their stay, for over three quarters of them a death at home had been their preference. However, for some, coming to the hospice is the only way that they can be gain a sense of emotional safety for them and their families as symptoms and difficulties progress. Yet, if support is tailored and suitable within the community setting this may prevent this crisis point being reached, allowing home to remain a place of comfort and security.
It was evident that community support prior to admission varied widely for patients. Just under half of all patients had district nurse support prior to admission. It is possible that the practical care provided by district nurses may have allowed some patients to remain in the home setting for longer, where that was their preference. Greater access to community-based non-specialist palliative care support is needed; a review of current community based palliative care support may be useful prior to admission to a hospice IPU.
It is also important to consider the cohort of patients for whom EOLC at home was deemed to be impossible by them, their family/carers or a professional. Some admissions to the hospice had low symptom burden and low complexity but did need admission. This suggests that a less intensive place of care might offer an alternative to a specialist admission. This could be a designated bed in a care home or community hospital or could be a lower intensity nurse led bed in a hospice. From this analysis, it would seem this merits further investigation and testing.
Staff and patient reported outcomes measures were collected routinely in the hospices examined, however the rate of completion varied. Staff-reported outcomes, such as the Karnofsky Performance Scale and the Phase of Illness, were completed during over 80% of admissions. However, the integrated palliative outcome scale was completed for just over a quarter of admissions (28%). Regular outcome assessment in clinical practice facilitates monitoring of the patient’s situation, better symptom management and insight into the patient priorities. 24 However, barriers to completing patient reported outcome measures are common and include fear of change, feeling that one is being assessed or monitored and fear of added workload. 25 Factors influencing the implementation of outcome measures reside at both the individual and organisational levels. 26 Individuals need to be confident in their understanding of outcome measures, and why they are used. They also need to be consulted as part of the implementation process. Organisations need to provide regular training for staff and ensure that electronic systems are adapted to ensure that outcomes can be easily input and consulted when needed. 26 Bradshaw and colleagues provide useful questions to facilitate outcome measurement in palliative care settings; and drawing on this line of work to improve outcome measurement is recommended. 26
Strengths and limitations
Strengths of this study are in the ability to offer insight into who is using hospice IPU services and why; using prospective, real time admission information, over the geographical area of one UK city. Using mixed-methods and a range of data sources gives a rounded perspective on the quantitative data and captures the perspectives of patients and family members and clinicians. The study, while conducted in 2019 meets the current needs for high quality data on what hospices do who they support and how, essential to enable hospices to improve their services, address unmet needs and provide the most appropriate services for the population. 27
Limitations are in the difficulty in gaining perspectives of those who were admitted to the hospice units close to death as staff within the IPU felt not appropriate to include them in the study as they are deemed as too weak or unwell to be interviewed. Patients who were assessed by staff as being extremely distressed were also excluded from the study. Further limitations are in the incomplete data and documentation of preferred place of death and IPOS scores.
Implications for research and practice
Despite the increasing focus on the need for specialist palliative care support for all who would benefit, irrespective of diagnosis, the findings from our service evaluation suggest that at least some hospice IPUs mainly support people with cancer. Hospice IPUs need to consider whether they can support people with other diagnoses, plan how this can be done equitably and promote their services more widely to referrers so that more people with complex needs towards the end of life can benefit from hospice inpatient care.
Greater formal acknowledgement of the non-physical needs of patients, and their families, that result in an admission to a hospice IPU would be helpful. Existential loneliness, anxiety, and inability to cope, are reasons for admission alongside physical symptoms.8,28 Documentation of these needs would provide a more in-depth picture of the holistic care required by the patient admitted to the IPU, and their family. Similarly, routine outcome assessment can help monitor whether interventions are working, and needs are being addressed; thus, training and support for routine outcome assessment is warranted.
Care in the community needs to be tailored to meet the individual needs of patients and their families, allowing for flexibility in the way care is provided.
Developing alternatives to hospice admission should be explored, to support those patients who are close to end-of-life, whose symptoms and needs are not complex, but for whom care at home becomes impossible. These could be nurse led beds in the hospice, or alternatives, such as care homes or community hospitals.
Conclusion
Evidence from two Scottish hospice IPUs found that most patients admitted had cancer and were near end of life. Sustained efforts to promote the hospice as place of care for people with conditions other than cancer are needed alongside greater consideration of the role of the hospice IPU, and who would benefit most from IPU support.
The role of hospice IPU is meeting important need for patents and their family whereby social isolation and lack of emotional safety impacts on the physical burden of the disease. While most patients in this study had access to specialist palliative care support prior to admission unmanageable physical symptoms, worry and anxiety led to admission. More emphasis needs to be placed on well-coordinated and flexible care in the community with increased involvement from primary care and social care as this may avoid admission into Hospice IPU for those who would wish to be cared for and die at home.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524231182724 – Supplemental material for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study
Supplemental material, sj-docx-1-pcr-10.1177_26323524231182724 for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study by Erna Haraldsdottir, Anna Lloyd, Martyn Bijak, Libby Milton and Anne M. Finucane in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524231182724 – Supplemental material for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study
Supplemental material, sj-docx-2-pcr-10.1177_26323524231182724 for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study by Erna Haraldsdottir, Anna Lloyd, Martyn Bijak, Libby Milton and Anne M. Finucane in Palliative Care and Social Practice
Supplemental Material
sj-docx-3-pcr-10.1177_26323524231182724 – Supplemental material for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study
Supplemental material, sj-docx-3-pcr-10.1177_26323524231182724 for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study by Erna Haraldsdottir, Anna Lloyd, Martyn Bijak, Libby Milton and Anne M. Finucane in Palliative Care and Social Practice
Supplemental Material
sj-docx-4-pcr-10.1177_26323524231182724 – Supplemental material for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study
Supplemental material, sj-docx-4-pcr-10.1177_26323524231182724 for Inpatient hospice admissions. Who is admitted and why: a mixed-method prospective study by Erna Haraldsdottir, Anna Lloyd, Martyn Bijak, Libby Milton and Anne M. Finucane in Palliative Care and Social Practice
Footnotes
Acknowledgements
The authors wish to thank all patients, families and clinicians who took part in the interviews as well as the hospice staff who supported the gathering of clinical data and in identifying participants for interview as well as their support and welcome of our researcher.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.