
Abstract
Background:
The coronavirus disease (COVID-19) pandemic has challenged palliative end-of-life care for people with dementia. The site of death can be considered as an end-of-life care quality indicator. Most people with dementia prefer to die at nursing or private homes; however, in Japan, they are often hospitalized in psychiatric hospitals for management of neuropsychiatric symptoms. As palliative end-of-life care for older adults with Alzheimer’s disease and related dementias has been further challenged by the COVID-19 pandemic, little is known about its effects on the place of death in patients with dementia.
Objectives:
This study aimed to investigate the shifts in place of death from dementia during the COVID-19 pandemic in Japan. Changes throughout the pandemic were compared between deaths from dementia and from senility.
Design:
Cross-sectional.
Methods:
Death certificate data of individuals aged 65 years or older who died in Japan between 1 January 2018, and 31 December 2021, were used to extract the cause and place of death. Differences in place of death between the periods were estimated using multinomial logistic analysis with reference to death in private homes.
Results:
Deaths from dementia mostly occurred in hospitals (59%), while deaths from senility were most frequent in nursing homes (37%). After adjusting for patient characteristics, the likelihood of hospital deaths significantly increased for patients with dementia during the pandemic. Meanwhile, the likelihood of senility deaths decreased in hospitals but increased in nursing homes during the pandemic.
Conclusion:
The shift to hospital deaths since the onset of the COVID-19 pandemic was uniquely observed in deaths from dementia. This hospital shift likely involved increased transfers from nursing and private homes to psychiatric hospitals. Further investigation is needed to examine the association between the pandemic-related change in long-term care workforce and palliative care practice in people with dementia.
Background
Since 2020, the coronavirus disease (COVID-19) pandemic has challenged palliative end-of-life care for older adults with Alzheimer’s disease and related dementias who have specific vulnerability to COVID-19 and related mortality. 1 Fulfillment of the person’s preference for place of death is identified as an essential component of end-of-life care.2,3 Most people with dementia prefer to die at nursing or private homes. 4 Therefore, home death in some cases can mean the archived concordance between preferred and actual place of death, which is an end-of-life care quality indicator. 5 However, dying at home usually requires a dedicated caregiver and significant medical and social support. 6 The healthcare crisis brought by the pandemic may have limited the capacity of the healthcare sector, while families may have hesitated to transfer patients to hospitals because of disallowed visits to dying patients.
Japan has also faced the challenge in palliative care for people with dementia since the onset of the COVID-19 pandemic. Even before the pandemic, half the deaths from dementia occurred at hospitals.7,8 Home-based palliative care for older adults in Japan, such as home-visiting nursing care and home care support clinics, typically serve patients with a primary diagnosis of malignant neoplasm.9,10 The shortage of home-based palliative care workers may have resulted in more hospital transfers, since 18.9% of inpatients with dementia in 2017 were hospitalized because home-based care services were unavailable.11,12 A considerable part of hospital deaths from dementia is assumed to occur at psychiatric hospitals, as 68% of the inpatients with dementia in June 2017 were hospitalized in psychiatric beds. 11 In Japan, psychiatric inpatient care is designated for managing neuropsychiatric symptoms with the aim of discharge to home. 13 However, of the inpatients with dementia in psychiatric facilities, 18% die in hospitals. 14 Management of neuropsychiatric symptoms in psychiatric hospitals may involve the use of physical restraint 15 and antipsychotic medication, 16 while international recommendations prioritize psychosocial interventions tailored to the patient’s needs.17,18 The COVID-19 pandemic added a burden of infection control measures to nursing home staff, resulting in suboptimal workforce to address neuropsychiatric symptoms. 19 As a result, such drastic workforce changes and accompanied challenges could facilitate the transfer of people with dementia into hospitals. In fact, the percentage of psychiatric hospitalization among dementia inpatients appeared to be higher in June 2020 (76%) 20 than in 2017. 11 However, no examination on the change in place of death of patients with dementia has been carried out to assess the pre- and post-pandemic trends.
This study aimed to measure shifts in place of death from dementia during the COVID-19 pandemic in Japan. Toward this goal, we compared pre- and post-pandemic change between deaths from dementia and from senility. We hypothesized that following the onset of the pandemic, hospital deaths due to dementia may have increased, but not deaths from senility. When it was the underlying cause of death, hospital deaths due to dementia were assumed to represent hospital deaths of patients with dementia at psychiatric hospitals but not at acute hospitals aiming at the treatment of physical illness.
Methods
This cross-sectional study used death certificate data from Japan. Deaths of individuals aged 65 years or older that occurred between 1 January 2018 and 31 December 2021, were extracted.
The underlying cause of death was obtained from death certificates using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes. In Japan, death certificates are completed by a medical doctor within 7 days of death, and the underlying cause of death is identified. Deaths resulting from dementia (F00-03 and G30), senility (R54), and COVID-19 (U07.1 and U07.2) were identified. Senility was chosen as a reference group to account for cases where an absence of acute physical illness required hospital transfer. Classifications of ICD-10 codes in dementia and senility were based on the Lancet Commission on Palliative Care and Pain Relief. 21 Deaths from COVID-19 were sampled as to measure the level of healthcare shortage during the pandemic period. Under the Infectious Diseases Control Law in Japan, patients with COVID-19 are admitted to specific care units for infection control. However, there were less than 2000 beds for infection control nationwide.1,22 Regional governments sequentially designated preexisting acute care units and workforce for replacement with COVID-19 units. Thus, we chose the number of deaths from COVID-19 as a surrogate indicator of the healthcare shortage. Owing to the smaller number of deaths compared with dementia and senility, deaths from COVID-19 were not included in the multivariate analyses.
Place of death was classified into the following categories: ‘hospital’, ‘intermediate geriatric care facility’ (rehabilitation facility aimed at home discharge), ‘nursing home’, ‘private home’, or ‘other place, unspecified’.
The pandemic period was defined to have started on 7 April 2020, the date of the first countermeasures against COVID-19. Additionally, as new infections and deaths resurged in 2021, a sensitivity analysis was performed, in which the pandemic period was defined to have begun on 8 January 2021, when a second set of countermeasures was introduced in Japan.
Covariates included the deceased’s sex, age at death, country of citizenship, marital status, and household working status, which were obtained from the death certificate data.
The distribution of places of death was calculated per month, as was the underlying cause. To examine the differences in place of death from dementia between the pre and during the pandemic periods, multinomial logistic analysis of place of death was performed with death in private homes as reference. Other decedent characteristics (sex, age at death, country of citizenship, marital status, and household working status) were also included as covariates. Multinomial logistic analysis was also performed for place of death from senility. In these analyses, full information maximum likelihood was used to handle missing data. 23 All analyses were performed using Mplus for Windows, version 8.8 (Muthén & Muthén, Los Angeles, CA, USA). Statistical significance was set as p < 0.05.
Results
A total of 5071,156 deaths occurred in older adults during the study period. Among these, 145,576 deaths (2.9%) were due to dementia, 508,383 (10.0%) due to senility, and 17,622 (0.3%) due to COVID-19. The decedent characteristics are reported in Table 1.
Characteristics of older adults who died from dementia, senility, or COVID-19 between January 2018 and December 2021.
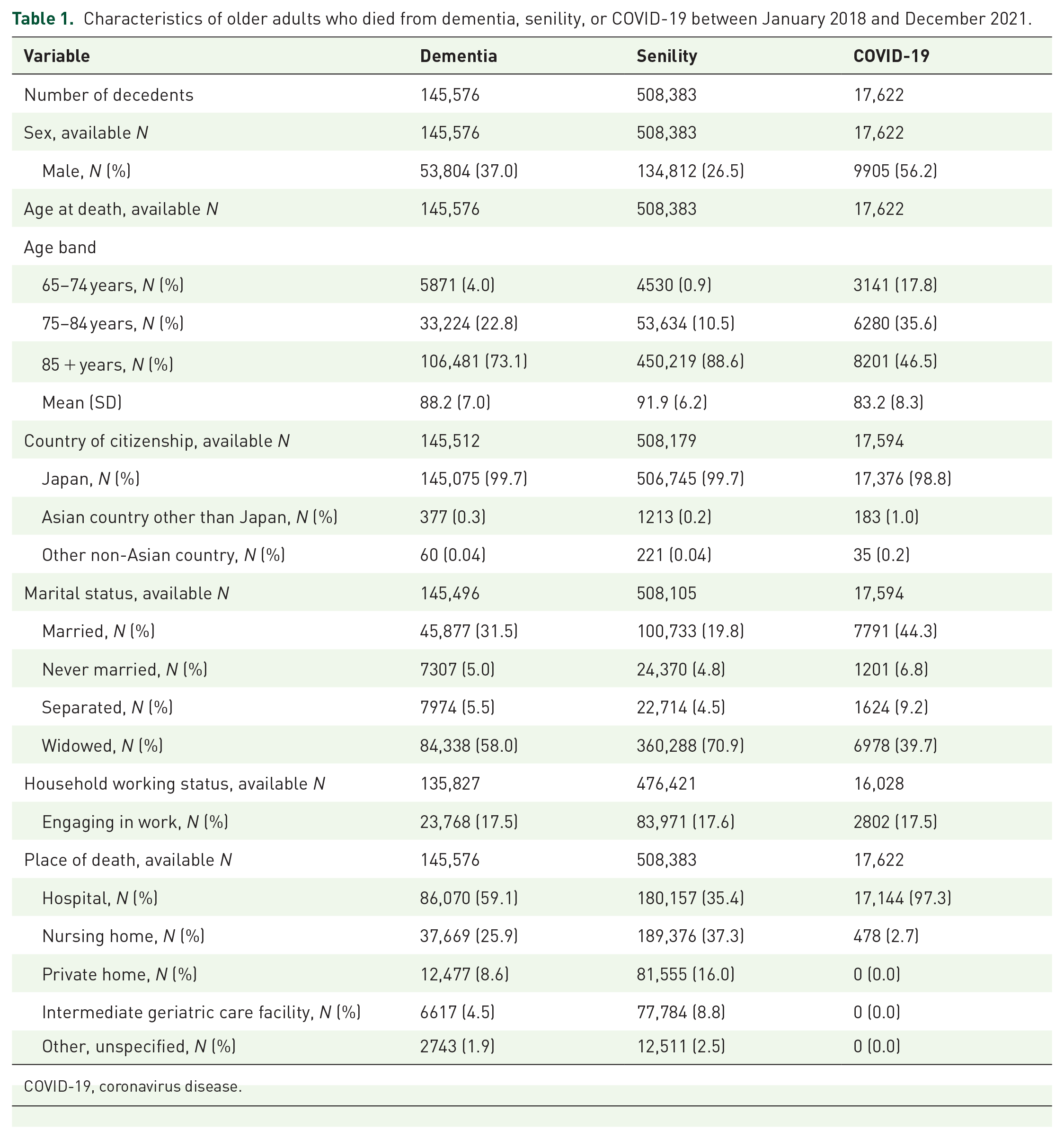
COVID-19, coronavirus disease.
Deaths from dementia occurred most frequently in hospitals (mean, 59.1%). An explicit decline in private or nursing home deaths was observed in deaths from dementia following the imposition of the second set of countermeasures against COVID-19. Senility deaths occurred mostly in nursing homes throughout the study period (mean, 37.3%) (Figure 1).

Monthly number of older adults who died from dementia, senility, or COVID-19 between 1 January 2018, and 31 December 2021: (a) Observed deaths from dementia. (b) Deaths from senility as the underlying cause. (c) Deaths from COVID-19 as the underlying cause. The observed monthly numbers of deaths are plotted per place of death that occurred between 1 January 2018 and 31 December 2021. The first countermeasures against COVID-19 are initiated on 7 April 2020. The second countermeasures were initiated on 8 January 2021.
The likelihood of hospital deaths significantly increased in patients with dementia during the pandemic since 7 April 2020 [adjusted odds ratio (OR) = 1.23, 95% confidence interval (CI) = 1.18 to 1.28, p < 0.001] and 8 January 2021 (adjusted OR = 1.73, 95% CI = 1.64–1.81, p < 0.001). Hospital deaths for patients with senility have declined since 7 April 2020 (adjusted OR = 0.78, 95% CI = 0.77–0.80, p < 0.001) and 8 January 2021 (adjusted OR = 0.81, 95%CI = 0.79–0.82, p < 0.001). Deaths in nursing homes, intermediate geriatric care, and other unspecified places became less likely to occur than in private homes (Figure 2).
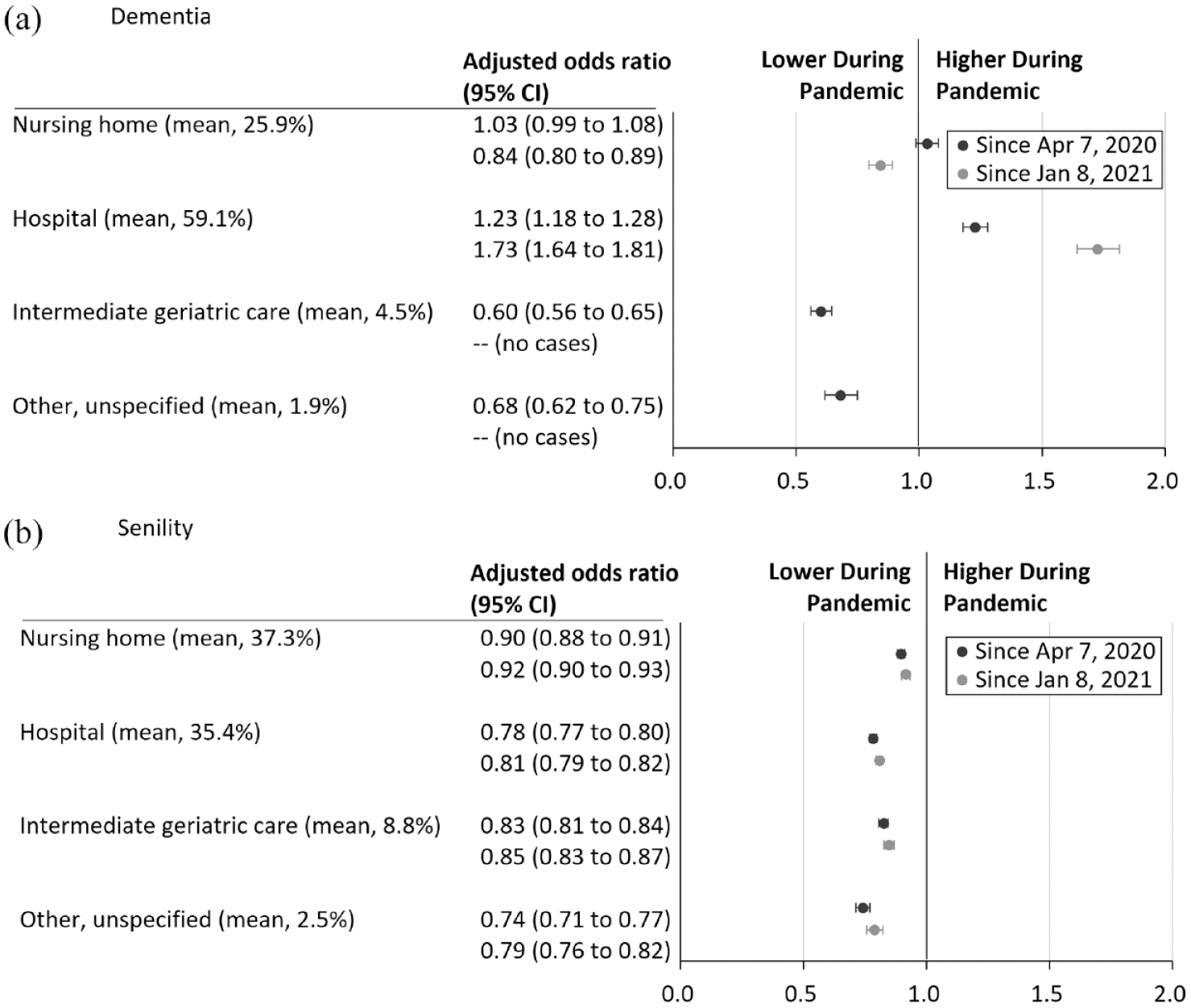
Adjusted odds ratios in place of death between before and during the COVID-19 pandemic: (a) Estimates of deaths from dementia as the underlying cause. (b) Estimates of deaths from senility as the underlying cause. Estimated odds ratios are plotted with 95% confidence intervals (CIs) for differences in the place of death between before and during the pandemic, with reference to private home deaths. A vertical line at 0 indicates no difference. Estimation of odds ratios is adjusted for decedent characteristics, including sex, age band, country of citizenship, marital status, and household working status.
Discussion
An increasing trend of hospital deaths from dementia has been seen in Japan throughout the COVID-19 pandemic. However, this shift may not be attributed to a changing underlying cause of death from dementia to death from COVID-19 infections and subsequent hospital transfer, as home deaths did not decline for patients with senility.
This pandemic-related change in place of death demonstrated the contrast between dementia and senility. It implies that the consequences of the COVID-19 pandemic-related healthcare crisis may have varied across the two populations. For senility, the healthcare shortage during the pandemic may have led to the increase in home deaths. Furthermore, healthcare staff shortages and pandemic-related restrictions such as disallowed visits to dying patients may have contributed to reduced hospital transfer of older adults dying from senility, resulting in reduced hospital deaths (Figure 2).
Despite this, the same underlying context may not apply to older adults with dementia, as hospital deaths increased during the pandemic. This appears to be a roll back against the pre-pandemic increase in nursing home deaths in Japan,6,24,25 suggesting dementia-specific challenges during the pandemic. Given the bed shortages in acute medical care settings and because psychiatric beds were less likely to be designated to treat patients with COVID-19 by the regional governments, it is likely that they were used for the care of individuals with dementia who needed specialized care. Although the data presented in the current study did not include types of hospitals in relation to hospital deaths, the observed shift in hospital deaths may have involved increased transfers from nursing and private homes to psychiatric hospitals.
Our results highlight the disproportional impact that the pandemic had on health and social care capacity for home deaths among people with dementia. The dementia-specific shift may indicate that the pandemic impeded effective palliative care including management of neuropsychiatric symptoms in private and nursing homes. The national dementia plans have included initiatives to shift end-of-life care from hospitals to communities 13 ; however, the existing framework for dementia care may not necessarily help long-term care providers to adapt to the pandemic-related changes in the lives of people with dementia. Specifically, psychiatric hospitals are considered to be privileged to use physical restraints and antipsychotic medications on people with dementia in Japan, which might have led to increased hospital transfers of patients with dementia when home care workers and nursing homes faced staff shortages and challenges to address neuropsychiatric symptoms. Japanese dementia policies before the pandemic have allowed psychiatric hospitals to use physical restraint and antipsychotic medication to manage neuropsychiatric symptoms of dementia. Contrary to the psychiatric care settings, Japanese long-term care policy prohibits in-home and residential care service providers from using mechanical and chemical restraints including psychotropics on older adults. 26
National statistics data show that as of June 2019, 8.1% of patients with dementia in psychiatric hospitals underwent at least one form of mechanical restraint or seclusion. 2 Patients with dementia in psychiatric hospitals are often prescribed with antipsychotic medications (56.2% as of September 2010). 28 However, home care workers, who are not allowed to use these measures, had limited knowledge of palliative care for people with dementia. 29 The United Nations committee alerted the Japanese government in 2022 that the national legal and healthcare systems appear to promote institutionalization of persons with dementia in psychiatric hospitals. 30 Such remaining issues regarding the lack of sufficient home-based palliative care in dementia policies combined with the pandemic-related healthcare crisis could have led to the contrasting end-of-life location allocation between older adults with dementia and those without the condition. Our findings underscore the urgent need for sufficient long-term care workforce for palliative care for people with dementia under the long-term restrictions.
Our study has some limitations. First, the death certificate data did not provide detailed information regarding changes in places of care relative to the time of death. As such, hospital deaths of long-stay inpatients could not be distinguished from those of dying residents transferred to hospitals from their private or nursing homes. Second, the data also lacked information regarding comorbidities such as pneumonia and other respiratory diseases. A long-term absence of routine care since the onset of pandemic among people with dementia was reported in Japan, 31 and this could have led to an increased risk of hospital admission. Third, coding of dementia and senility as an underlying cause of death in Japan may have had certain differences from that in other countries, 32 this should be considered in interpreting the generalizability of results.
In Japan, senility as an underlying cause of death was increasingly prioritized over pneumonia and aspiration pneumonia in alignment with the national guidelines and recommendations. 33 This could cause overestimation of senility over dementia, as there has been no recommendations for identifying dementia as an underlying cause of death in Japan. Future research including deaths from physical illness with and without comorbid dementia may be helpful to clarify the interaction between dementia and the COVID-19 pandemic in determining the distribution of the locations of death. In addition, the severity of the healthcare crisis associated with the pandemic varied across countries, which should be considered when interpreting the impact of the pandemic on the availability of hospital beds. 34 Finally, dementia might not have been recorded in the death certificates of some decedents as clinical diagnoses of dementia are underreported as the main cause of death in death certificates.35,36
Despite these limitations, our study is the first of its kind to indicate the shift to hospitals as a place of death among people with dementia since the onset of the COVID-19 pandemic. We believe that national dementia policies and initiatives should recognize the need for long-term care workforce to provide effective palliative end-of-life care to people with dementia under the long-term restrictions.