
Abstract
A home is a preferred place of death by most people. Nurses play a key role in supporting end-of-life home care, yet less is known about the factors that determine home as a place of death. This scoping review describes the percentage of actual places of death and determines social factors related to home as the place of death among noncancer patients with end-stage chronic health conditions. Inclusion criteria included (1) noncancer chronic illness conditions, (2) outcomes of place of death, and (3) factors that determine home as a place of death. Sources of evidence included PubMed, CINAHL, and Web of Science databases, which were searched in May 2022, and additional searches from May 2022 to November 2023.The JBI scoping review guide (2020) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Scoping Review extension were used. Twenty-eight studies were included in this analysis. The range of percentages is varied within the same place of death among the sample. Two major constructs that determine a home as a place of death were identified: preceding factors and social capital. The results suggest that the place of death among noncancer patients with end-stage chronic health conditions should be continued to be understood. Two constructs determined home as a place of death and are considered as a fundamental to increasing equal accessibility in the initiation of palliative care services to promote home death and meet end-of-life care goals.
Keywords
Background
Aging in place and dying at home are increasingly preferred options for people worldwide, including in the United States. 1 This trend has been evident since 2017, when dying at home surpassed dying in the hospital for the first time among Americans, 2 and it has continued to gain momentum, especially during and after COVID-19. 3 However, despite this growing preference, a significant disparity remains between the preferred and actual place of death. 4
The remaining varied locations of death, including nursing homes and healthcare facilities, suggest social inequity influences.5,6 Despite advantages, predicting disease trajectories in noncancer patients poses challenges, causing delays in palliative care, increased home care needs, and postponed hospice services. This results in a lower quality of life, higher likelihood of hospitalization for uncontrolled symptoms, and increased caregiver burden. 7
Understanding factors influencing end-of-life outcomes in chronic noncancer patients is vital amid the rising trend of home deaths. A comprehensive understanding of individual and systemic factors is crucial for aligning preferred and actual places of death. 8 Considering evolving factors such as personal values, healthcare policies, resources, social support, and family and professionals’ attitudes is essential. Analyzing these influences helps comprehend end-of-life care choices, ensuring alignment with patient preferences.
The objective of this scoping review is twofold: first, to determine the distribution of places of death among individuals with noncancer terminal illnesses, and second, to identify the factors influencing home death in those with noncancer chronic health conditions. By addressing these objectives, this scoping review aims to provide a comprehensive understanding of the factors associated with home death in noncancer patients, shedding light on gaps in the current literature and informing future research and practice in end-of-life care for this patient population.
Methods
This scoping review was conducted following the Joanna Briggs Institute (JBI) methodology for scoping reviews, 9 which aligned with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist 10 (see Supplemental Material 1 for the PRISMA-ScR checklist). The scoping review process, including search strategy, inclusion and exclusion criteria, data screening, data extraction, and synthesis, was conducted and is briefly described below.
Search strategy
The search strategy aimed to find published articles in English in databases, including PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, and Google Scholar. An article search was performed using these databases for the first search in May 2022 and an additional search from May 2022 to November 2023 offering the most up-to-date research included here. The initial search started by using the keywords consisting of the terms ‘determinants of health’ and ‘place of death’ in the CINAHL database. After that, looking at the keywords in the retrieved articles, synonyms of the place of death, such as the ‘site of death’ and ‘location of death’, were added and utilized in other databases. Each synonym search term was joined with the Boolean connector ‘OR’, and the Boolean connector ‘AND’ was used to combine different terms such as ‘determinants of health’ AND ‘place of death’. In addition, a bibliography search was performed on the included articles to identify additional relevant articles. The article publications were limited to English, and there was no publication time-limitation period (see Supplemental Material 2 for sample terms used for the initial CINAHL Search).
Inclusion and exclusion criteria
Studies were included if place of death was the outcome variable. The participants were descendants aged 18 years or older. They had chronic health conditions such as heart failure or cardiovascular diseases, dementia, or other noncancer chronic illness. The results of these studies also included factors associated with the place of death. Articles were excluded if there were no factors correlating with death at home or if the sample did not include noncancer patients.
Selection of studies
The retrieved articles were independently screened for eligibility based on the titles and abstracts. Duplicate articles were removed. The entire text was then reviewed in detail to verify that the articles met the inclusion criteria. Subsequently, articles were selected for data extraction. Any disagreements between reviewers (SG and RGL) at each stage of the selection process were resolved through discussion. The search results and study inclusion process are reported and presented in the PRISMA-ScR flow diagram (see Figure 1).
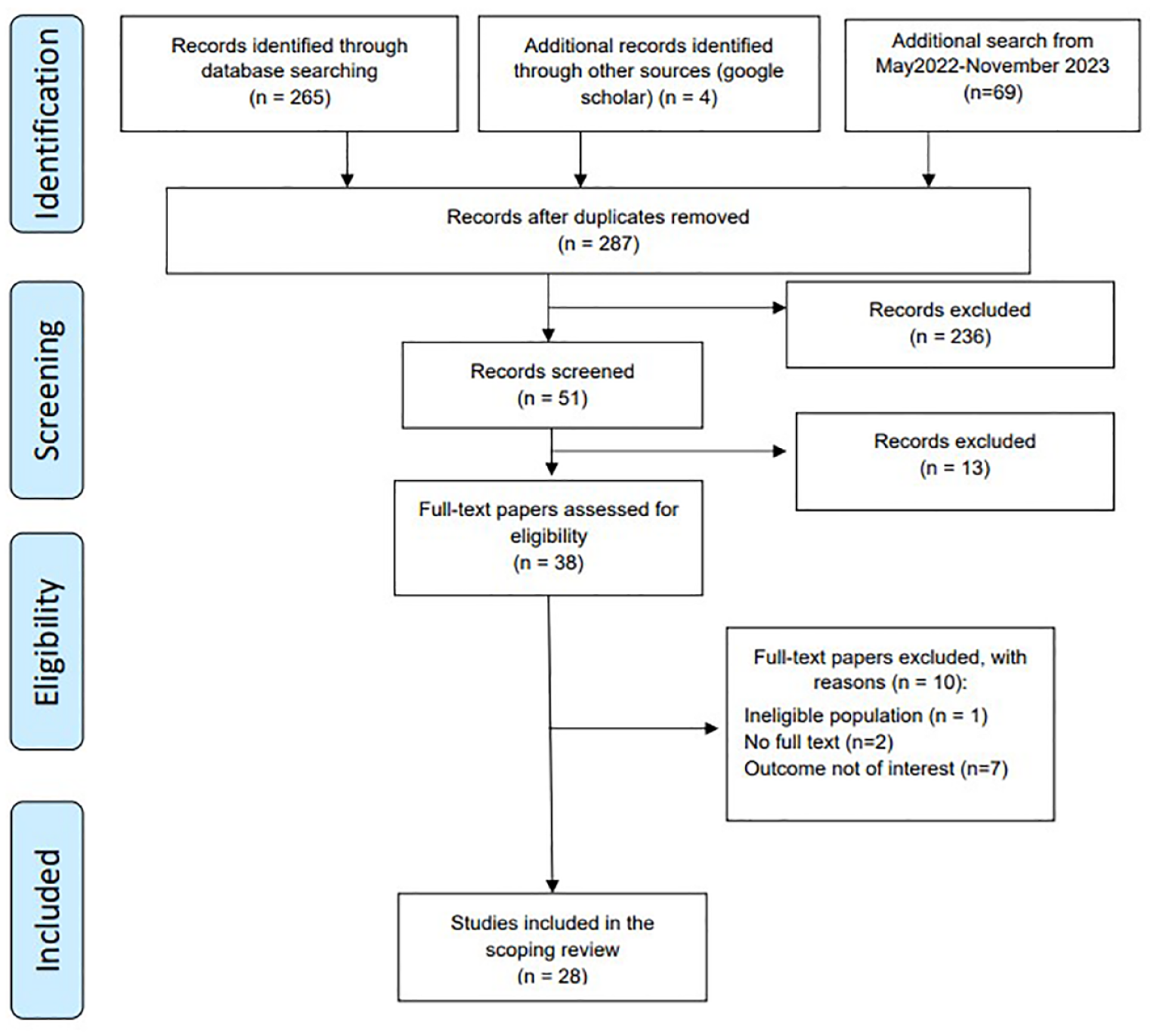
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Data extraction
Data were extracted from articles included in this scoping review by two independent reviewers using a data extraction tool developed by the reviewers, as shown in Table 1. The extracted data included specific details about the author/s, year of publication, characteristics of the participants, main factors associated with home death, and percentage of the place of death, which are vital findings relevant to the review objectives.
Data extraction (n = 28).

PC, palliative care; COPD, chronic, obstructive, pulmonary, disease; ADL, activities of daily living; GPs, general practitioners; PCU, Palliative care unit; PWD, people with dementia.
Results
The initial database searches retrieved 265 studies and added 4 articles from another source, and the additional search retrieved 69 studies, accounting for duplicates. Subsequently, the titles and abstracts of these 287 articles were reviewed, leading to the selection of 51 articles for a full-text examination. Ultimately, 38 of these articles met the eligibility criteria. After a comprehensive review, 28 articles were included in this analysis. The reasons for excluding articles are outlined in Figure 1 (PRISMA flow diagram).
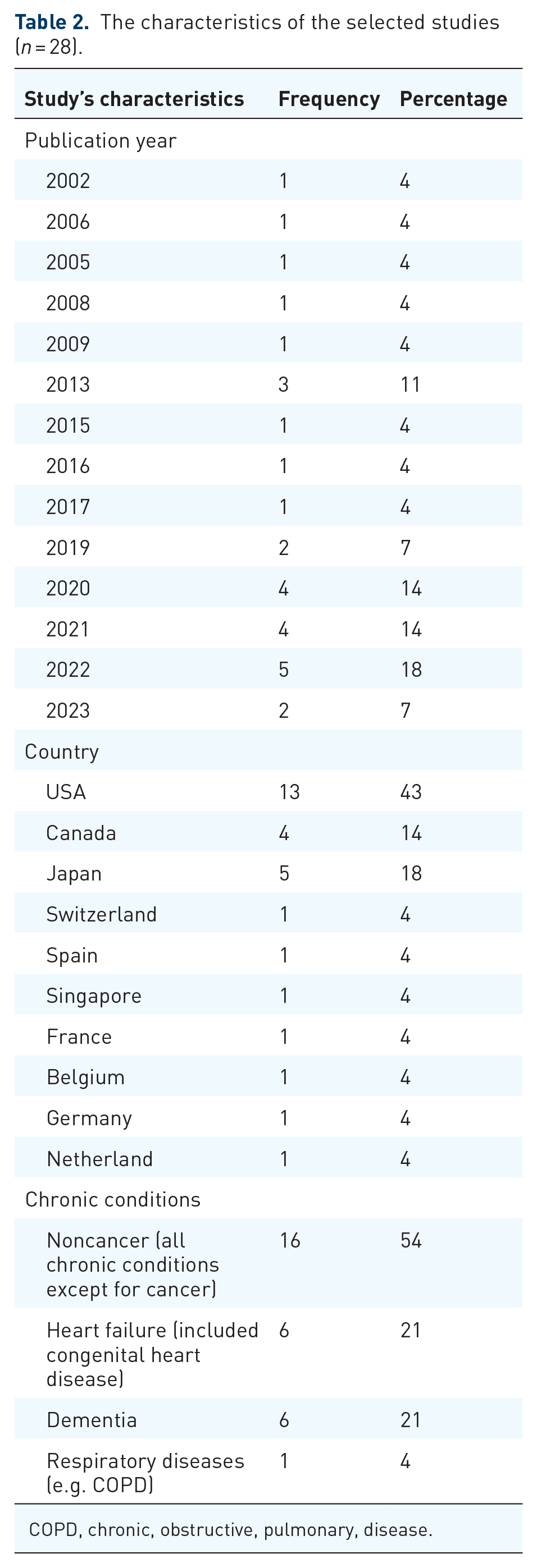
Publications were also categorized by the year of publication, country of origin, and noncancer chronic condition foci. In this review, there are more robust publications on this topic between 2020 and 2022, from the United States and Japan, with the highest number of publications and the primary chronic condition being noncancer (54%) (n = 15), heart failure (21%) (n = 6), dementia (21%) (n = 6), and respiratory disease (4%) (n = 1) (see Table 2).
The characteristics of the selected studies (n = 28).
COPD, chronic, obstructive, pulmonary, disease.
As data provided in Table 1 demonstrate, the percentage of actual place of death for noncancer terminally ill conditions varies across different settings. The highest proportion of deaths occurred in hospitals, accounting for approximately 13.2–80.94% of cases, followed by nursing homes around 1.5–37.3% and residential care around 1.7–28.8%. Home deaths accounted for around 11.1–72.10% of cases, while hospice facilities saw a lower percentage, around 0.2–9.67%. Overall, hospitals and nursing homes were the most common places of death among people with noncancer terminally ill conditions. Yet, a significant but more variable percentage occurred at home. Hospice facilities had the lowest proportion of deaths among the reported settings.
We compiled this list of factors investigated in the study, all of which held significance in some aspect of the research. Our primary focus was to explore a wide array of factors associated with home deaths, with a priority on examining correlations rather than making predictions. For example, in certain studies, the main objective was to predict outcomes such as home deaths. Even if the final model did not yield statistical significance, we considered preliminary models that revealed meaningful relationships between specific factors and home deaths.
Based on this scoping review, several factors are associated with the home as a place of death. These factors can be categorized into two groups: individual factors, including demographics, socioeconomic status, and clinical data, and social factors, which encompass resources available within the family, community, and healthcare services. The review of the literature identified the top five individual factors linked to home death (n = 28). These factors include comorbidity (43%), sex (29%), age (25%), race (18%), and marital status (14%).
As for social factors, the top five contributors to home death were found to be the utilization of palliative care or hospice care at the end of life (21%), census division (14%), geographical areas (14%), and the presence of both informal and formal caregivers (e.g., family caregivers, healthcare providers) at 7%. For a comprehensive list, refer to Table 3.
Factors associated with a home death (n = 28).

One study may result in more than one significant factor. ADL, activities of daily living; GPs, general practitioners.
Discussion
The scoping review uncovered variations in the actual place of death for individuals with non-cancer-related chronic conditions. These variations are influenced by individual characteristics, existing social inequities, 5 and disease trajectories. 11 For instance, conditions like heart failure and respiratory disease exhibit intermittent declines in psychosocial well-being due to long-term physical conditions, with disease exacerbation potentially leading to sudden death in hospitals.12,13 In contrast, dementia often presents a gradual decline in physical and social well-being due to the progressive nature of the disease, often resulting in a hospital or nursing home death. 14 Importantly, the COVID-19 pandemic is noted as a factor that widens the range of variation in the place of death. 15 This identified phenomenon emphasizes a gap in palliative care services, suggesting that appropriate palliative care has the potential to reduce unplanned readmissions and allow patients to experience more comfortable deaths in their preferred locations.
We have identified various factors that determine home as an actual place of death. We propose that the desire to die at home is influenced not only by individual factors but also by social factors. These factors are likely to explain the possibility of dying at home, as patients and caregivers require social resources to support them. In other words, they rely on extensive resources and support, including family members, relatives, community, and neighborhood resources as well as resources as the result of health policies and the healthcare system. These resources play a crucial role in assisting patients and caregivers in navigating the complexities of end-of-life care, particularly as death approaches. As identified social factors, we then categorize these into themes, including preceding factors, social capital (resources/support), and the outcome (home death).
The preceding factors
The understanding of home death involves considering a range of factors that can either support or hinder this outcome. These factors encompass individual and clinical aspects, with chronic conditions and comorbidity (e.g. dementia, heart failure) being significant contributors.7,14,16–25,26,27 These conditions can lead to suffering and pose challenges for informal caregivers who may lack training in managing these complex problems. Despite these challenges, some patients and caregivers still prefer home death and seek external support for care at home to align with the patient’s preferences.22,28
Demographic and socioeconomic factors also play a role in end-of-life care decisions. 29 For example, inconsistency is still found around the reported demographics of sex and age in this review; however, it appears more likely that males are likely to die at home than females. Older age is associated with a higher likelihood of home death.7,17,19,22–24,30–33 However, demographic factors of race, and single marital status can act as barriers to home death, leading to a higher likelihood of hospital deaths due to limited support.19,20,22–24,31,34,35 Similar findings show that socioeconomic factors of lower educational attainment and lower income are associated with a lower likelihood of a home death. This is consistent with other findings6,36 that suggest significant health disparities and social inequity influence place of death outcomes.
Social capital in the palliative care context is defined as the resources and support received by patients and caregivers from their social relationships at micro, meso, and macro levels. 37
Micro (individual) level
Related individual demographic, socioeconomic, and clinical factors play a significant role in patients’ possibility to die at home. Notably, patients who have strong support from family members, live with them, and express a preference for home death are more likely to die at home.21,38 This scoping review highlights the importance of obtaining resources and support from family members in achieving home death. By comprehending and addressing these factors, we can enhance patients’ prospects of receiving quality care at home and realizing their end-of-life preferences.
Importantly, the preferences of both the patient and the caregiver are significant. A study revealed that when caregivers expressed a preference for the patient to die at home, it positively influenced the likelihood of home death. 21 Taking into account the preferences of both parties is vital in facilitating end-of-life care decisions and providing the necessary support.
Community level (meso level)
Community and neighborhood cohesion play a crucial role as resources and support for patients and their caregivers. 39 The process of dying at home demands considerable effort from both patients and their families. As a result, social support from community resources, encompassing emotional, tangible, and informational assistance, is considered imperative. 40 While a community of formal care circles with trained and private staff for specific palliative/hospice care may be available, 41 its universal feasibility is not assured. Persistent challenges significantly affect the viability of home-based end-of-life care, hindering patients from receiving the necessary assistance and support in the comfort of their homes.41,42 This scoping review underscores the necessity for future research to explore community resources within the care circle for this patient population, with a particular focus on informal social networks, community cohesion, and their functions.
Macro (system/society) level
The underutilization of palliative care, a palliative care training shortage, and delays in initiating these services present significant obstacles, hindering patients and their families from obtaining optimal end-of-life care and realizing their preference for the location of death.7,22,24,43,44 These challenges underscore the pivotal role of health policy and medical legislation related to end-of-life care services and related support systems. 45 Studies indicate that only specific regions have health policies supporting home or community palliative care.19,24,32,44 Adding to the complexity, census division and geographical differences, as revealed in this scoping review, contribute to disparities in access to palliative care services, with notable distinctions between rural and urban areas.17,23,33,42
In response to these complexities, urgent steps are required to advance the implementation of early palliative and hospice care services for all. This proactive approach addresses the identified challenges and ensures equitable access to high-quality end-of-life care across diverse regions and circumstances.
The outcome, home death, is the outcome of emphasis in this scoping review and refers to both the place of care and the place where patients ultimately die. Preceding factors come into play to achieve home death, initiating individual resources at the micro, macro, and meso levels.
Therefore, based on the multiple factors identified in this scoping review, we categorized them into two constructs and one outcome aligned with the framework of social capital for palliative care by Lewis et al. 37 , as depicted in Figure 2, which presents the model of home death. This review summarizes two significant constructs associated with home as the preferred place of death for individuals with noncancer end-stage chronic health conditions. These constructs include preceding factors and social factors, with home death the outcome.

The model of home death: preceding factors and social capital influence on home death in noncancer patients with end-stage chronic health conditions.
It is important to consider the variations in healthcare systems and cultural caregiving practices across world regions. 24 Western countries often have nursing homes and residential care facilities as options for older adults where they can receive end-of-life care. In contrast, some Asian countries like Singapore and Japan prioritize aging in place and supporting home-based care for ill individuals. 22 These differences impact the availability and utilization of home-based care services, affecting the opportunities and preferences for home death in noncancer patients with end-stage chronic health conditions.
Limitations
Our scoping review had certain limitations in the search process. Although we conducted searches across multiple databases, the keywords used were broad in nature. Additionally, we did not include gray literature in our search, which could have resulted in the omission of relevant studies. Another limitation pertains to the analysis of data concerning the place of death in relation to specific chronic conditions. We observed a wide range of percentages within the same place of death, which restricts the generalizability of these findings when collectively considered. These results should be interpreted with caution given the wide range of percentage results associated with various conditions. Furthermore, our review did not establish definitive cause-and-effect relationships between the factors, further limiting our ability to draw conclusive conclusions about their relationships. It is important to acknowledge these limitations as they may impact the comprehensiveness and applicability of our review’s conclusions while calling for additional research that is needed in this area of inquiry.
Conclusion
The place of death in patients with noncancer chronic health conditions is wide-ranging and influenced by various factors. While the distribution of places of death may not provide universal insights, it is a valuable starting point for understanding the patterns in different regions. It can provide insights into the effectiveness of certain policies or practices and inform best practices for end-of-life care. In addition, this will help tailoring end-of-life care strategies to the specific context of the study area. Our review did not establish clear cause-and-effect relationships between these factors, limiting our ability to draw definitive conclusions. However, it can be summarized that noncancer chronic conditions were more likely to die in healthcare facilities such as hospitals, nursing homes, and long-term care settings. When considering factors associated with home death, preceding factors (demographics and socioeconomics) and social factors emerged as significant.
These findings highlight the importance of initiating community-based palliative care early in the course of chronic health conditions. By providing timely symptom management and mobilizing palliative care and social care resources and support across the three levels (individual, community, and system), patients can be better prepared for a dignified death in their preferred setting.
It is crucial to recognize that there are still many social aspects to explore, such as examining additional resources and support, addressing specific preceding factors to ensure equitable access within the healthcare system, and promoting home death as a feasible outcome. These findings have implications for further research and practice, particularly for understanding the factors that determine the place of death in terminally ill patients with chronic conditions, with a specific focus on social factors at the meso (community) level. By delving deeper into these areas, we can enhance our understanding of how social factors influence end-of-life care decisions and develop strategies with a palliative care framework to promote home death while ensuring equal accessibility and support for all patients.
A compassionate and patient-centered approach to end-of-life care involves understanding individual clinical conditions, patient preferences, and socioeconomic and demographic variables. By tailoring interventions based on these factors and examining available resources and support, healthcare providers can enhance the quality of care and ensure that patients receive treatment in their preferred setting.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524241236964 – Supplemental material for The determinants of actual place of death among noncancer patients with end-stage chronic health conditions: a scoping review
Supplemental material, sj-docx-1-pcr-10.1177_26323524241236964 for The determinants of actual place of death among noncancer patients with end-stage chronic health conditions: a scoping review by Sangduan Ginggeaw and Raeann LeBlanc in Palliative Care and Social Practice
Supplemental Material
sj-docx-2-pcr-10.1177_26323524241236964 – Supplemental material for The determinants of actual place of death among noncancer patients with end-stage chronic health conditions: a scoping review
Supplemental material, sj-docx-2-pcr-10.1177_26323524241236964 for The determinants of actual place of death among noncancer patients with end-stage chronic health conditions: a scoping review by Sangduan Ginggeaw and Raeann LeBlanc in Palliative Care and Social Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.