
Abstract
Midazolam is a commonly used benzodiazepine in palliative care and is considered one of the four essential drugs needed for the promotion of quality care in dying patients. Acting on the benzodiazepine receptor, it promotes the action of gamma-aminobutyric acid. Gamma-aminobutyric acid action promotes sedative, anxiolytic, and anticonvulsant properties. Midazolam has a faster onset and shorter duration of action than other benzodiazepines such as diazepam and lorazepam lending itself to greater flexibility in dosing than other benzodiazepines. The kidneys excrete midazolam and its active metabolite. Metabolism occurs in the liver by the P450 system. This article examines the pharmacology, pharmacodynamics, and clinical uses of midazolam in palliative care.
Keywords
Introduction
Since the accidental synthesis of the first benzodiazepine, chlordiazepoxide, in 1961, benzodiazepines have emerged as important agents for symptom control in palliative medicine. 1 Benzodiazepines treat a variety of symptoms in palliative care, including anxiety, delirium associated with alcohol withdrawal, seizures, and when symptoms are refractory, they are used for palliative sedation therapy.2,3 Benzodiazepines combined with haloperidol is emerging as an effective treatment for delirium. 4 Benzodiazepines if misused can lead to withdrawal symptoms and cognitive impairment. 2 The ideal benzodiazepine for use in palliative care would be one where there is rapid onset of action, yet have a short duration to minimize adverse effects. Midazolam is one benzodiazepine fitting this description. This review examines the pharmacology, pharmacodynamics, and evidence for use in palliative medicine. Midazolam is considered one of the four essential drugs that should be available in all settings caring for dying patients. 3
Structure of midazolam
Midazolam contains a benzene ring fused to a seven-membered diazepine ring (see Figure 1). 5
Structure Midazolam.
Pharmacodynamics
Midazolam binds with high affinity to the benzodiazepine receptor, which is at the interface of the α and γ subunits of the gamma-aminobutyric acid receptor (GABA). 6 GABAA receptors mediate inhibitory functions in the human brain. 7 They are protein complexes consisting of five subunits, arranged pseudo-symmetrically around an ion channel selective for chloride (Cl−). 8 The major receptor, GABAA, consists of α1, β2, and γ2 subunits. 9 Benzodiazepines bind to the α and γ interface leading to anxiolytic, sedative, muscle relaxant, and anticonvulsive actions. Benzodiazepines are considered exogenous modulators of the GABA receptor. 10 When compared with other benzodiazepines, midazolam binds to the GABA benzodiazepine binding site as avidly as clonazepam (Ki 0.85 ± 0.02 nM) and lorazepam, but more avidly than diazepam (Ki 10 ± 1 nM).
Pharmacokinetics and metabolism
Midazolam exists in a pH equilibrium between closed and open ring structures. 11 The benzodiazepine ring of midazolam opens at lower pH. At physiologic pH, the ring closes and the molecule becomes lipid soluble allowing rapid penetration across the blood–brain barrier.12–14 The pH characteristics of midazolam allow preparation of salts that are readily soluble in aqueous media. 11 Midazolam onset of action is rapid regardless of the route. Both the intravenous (IV) and subcutaneous routes manifest onset of action within minutes. 15 Following IV administration, midazolam has a distribution half-life of 6–15 min. Midazolam has an elimination half-life of 1.5–3 h. The duration of action is 60–120 min. 16 The lipophilic nature of midazolam accounts for the relatively large volume of distribution at steady state, that is, 0.8–1.7 l/kg. 17 Oxidation of the imidazole ring leads to greater clearance than other benzodiazepines such as diazepam. 18 Intramuscular midazolam is rapidly absorbed with the onset of action within 2 min of administration. 13 Peak serum concentrations occur between 23 and 40 min. Intramuscular midazolam has a bioavailability of 90%.13,19,20 Intranasal (IN) midazolam has a rapid onset of action with a Tmax of 10–14 min. Bioavailability ranges between 60% and 80%. Increases in Cmax and AUC are dose proportionate. 21 Oral bioavailability is 40–50% due to extensive first-pass metabolism.22,23 When given orally, the onset of action is approximately 15 min reflecting its rapid absorption from the gastrointestinal (GI) tract. 23 CYP3A4 and CYP3A5 hydroxylate midazolam. 24 Patients with CYP3A4 mutations can experience increased sedation. 25 Metabolism yields three metabolites, α-hydroxy midazolam, 4-hydroxy midazolam, and α,4-hydroxy midazolam, all excreted as glucuronides. 14 α-hydroxy-midazolam is pharmacologically active with sedative properties like that of midazolam. It is a formation rate-limited metabolite and closely follows midazolam concentrations. 26 When glucuronidated, the α-hydroxy metabolite loses its potency and is one-tenth as potent as midazolam. 26 α-Hydroxy-midazolam accumulates to a greater extent after oral administration because of the first-pass metabolism. The α-hydroxy-midazolam metabolite has an elimination half-life of 1 h in humans. Excretion of midazolam is primarily by the kidneys. 14 Table 1 compares the pharmacology of midazolam with other commonly used benzodiazepines.
Pharmacology of Midazolam with Other Commonly Used Benzodiazepines.

Adapted from Howard and colleagues. 27
Dosing in special populations
Liver disease
Advanced cirrhosis reduces the plasma clearance and prolongs the half-life of midazolam. MacGilchrist and coworkers showed that cirrhotic patients had a significantly (p < 0.05) prolonged elimination half-life of midazolam (3.9 versus 1.6 h) compared with a control group. 28 The cirrhotic group experienced more profound sedation for up to 6 h when compared with controls. Critically ill patients with liver failure need careful dosing of midazolam.
Renal disease
Midazolam accumulates and can cause prolonged sedation in patients with renal dysfunction. 29 Patients can experience prolonged sedation in the setting of severe renal failure. 30 The active metabolite α-hydroxymethyl midazolam accumulates and contributes to sedation. Because patients with chronic renal failure and hypoalbuminemia have a higher fraction of unbound drug at greater risk for adverse effects, careful dosing of continuous infusions is necessary. 31
Advanced illness
Terminally ill patients experience significant physiologic changes affecting drug disposition. Loss of body weight and cachexia can lead to a decrease in Vd (volume of distribution). Decreasing Vd leads to increases in drug concentration and effect for lipophilic drugs like midazolam. 32 Low albumin levels, commonly seen in advanced illness, decrease the clearance of midazolam. 33
Elderly
Midazolam clearance decreases in the elderly. Prolonged elimination of half-life occurs in the elderly. 34 Liver blood flow decreases with age, and midazolam is a drug with a low hepatic extraction (0.3), so elimination prolongs in low hepatic blood flow states.32,35
Pediatric
In healthy neonates, the half-life (t1/2) and the clearance (Cl) are 3.3-fold longer and 3.7-fold shorter, respectively, than in adults owing to low levels of CYP3A4 and CYP3A5. These enzymes do not surge until the fourth week of life. Disease affects the pharmacokinetics of midazolam in neonates; multiple organ failure reduces the clearance of midazolam, and mechanical ventilation prolongs the t1/2 of this drug. Extracorporeal membrane oxygenation (ECMO) therapy increases t1/2, Cl, and Vd of midazolam several times. 36 Large inter-individual variations in midazolam clearance values exist in critically ill neonates, infants, children, and adolescents. 37 Midazolam appears to be a safe drug to use in neonates with incidences of hypotension and respiratory depression in low percentages. 36
Drug interactions
CYP3A4 metabolizes midazolam almost exclusively to its hydroxyl metabolites. 38 Inducers and inhibitors of CYP3A4 potentially affect midazolam levels. Drugs such as glucocorticoids, antifungals, antibiotics, retrovirals, antidepressants, calcium channel blockers, and H2 blockers interact to influence the disposition of midazolam.38,39 Table 2 summarizes the effects of midazolam drug interactions.
Drug Interactions.

AUC, Area under the curve.
Specific drug interactions are noted below. In general, the combination of benzodiazepines with drugs like opioids and antihistamines increases the risk of sedation and respiratory depression.
Adverse effects
Besides somnolence, most adverse effects are of low frequency. 68 Clinical trials show that midazolam is safe to give with opioids for the treatment of dyspnea in advanced illness.69,70 Hiccups occur with an incidence of approximately 3.6%. 71 Benzodiazepines cause disinhibition reactions to occur in both adult and pediatric patients, and midazolam is no exception. 72 However, benzodiazepines in combination with antipsychotics help control delirium. 73 Vorsanger and Roberts reported two cases of athetoid movements after receiving midazolam as a premedication. 74 Physostigmine reversed the movement. Midazolam can cause prolonged anterograde amnesia.75–77
Clinical applications of midazolam in palliative care
Palliative sedation therapy
Terminally ill cancer patients near the end of life can experience refractory symptoms, which require palliative sedation. Midazolam is the most common benzodiazepine used for palliative sedation therapy.78,79 It is also considered the first-line drug because of its ability to be easily reversed, lending itself to use in respite sedation and short-term palliative sedation. 80 One report in adult palliative sedation found mean midazolam doses of 29 mg/day (median: 30 mg, range: 15–60 mg/day). 81 A recent study in an Israeli hospice found average doses of midazolam up to 79 mg/day. 82 Mercadante and coworkers found mean doses were 23–58 mg/day. 83 Midazolam is useful for palliative sedation in the home setting for pediatric patients. 84 Initial doses were in the range of 0.02–0.08 mg/kg/h. 84 Mean dose was 0.02–1.0 mg/kg/h. 84 In treating terminal restlessness and agitation, Bottomley and Hanks 15 used continuous infusion of subcutaneous midazolam in 23 advanced cancer patients in hospice. The investigators achieved symptom control in 22 of 23 patients using initial doses of 0.4–0.8 mg/h. The mean maximum dose was 2.9 mg/h. Dosing varied between patients highlighting the need to individualize dosing. Midazolam along with droperidol or olanzapine remains a treatment option for agitated patients in the emergency room. 85
Dyspnea
Opioids are useful for the treatment of terminal dyspnea and anxiolytics help manage the anxiety associated with dyspnea. One trial (single-blinded) studied subcutaneous midazolam as an adjunct therapy to morphine in treating severe dyspnea in terminally ill cancer patients (N = 101). 69 Patients received one of three treatments. The morphine group consisted of subcutaneous scheduled morphine (2.5 mg every 4 h for opioid-naïve patients or a 25% increment over the daily dose for those receiving baseline opioids) with midazolam rescue doses (5 mg) for breakthrough dyspnea. The midazolam group received scheduled midazolam (5 mg every 4 h) with morphine rescues (2.5 mg) for breakthrough dyspnea. The morphine–midazolam group received scheduled morphine (2.5 mg every 4 h for opioid-naïve patients or a 25% increment over the daily dose for those receiving baseline opioids) and midazolam (5 mg every 4 h) with morphine rescue doses (2.5 mg) for breakthrough dyspnea; 35 patients entered in the morphine group, 33 in the midazolam group, and 33 in the morphine–midazolam group. At 24 h, the frequency of dyspnea relief was 69%, 46%, and 92% in the morphine, midazolam, and combined groups, respectively (p = 0.0004 and p = 0.03 for combined versus midazolam and combined versus morphine, respectively). At 48 h, the percentage of no relief was lowest on the morphine–midazolam group (those receiving scheduled morphine and midazolam; 4%). The data show that adding midazolam to morphine enhances dyspnea control.
Another study by the same author 70 compared morphine with midazolam for symptom relief during evaluations for dyspnea in patients with advanced cancer; 63 ambulatory patients with advanced cancer and dyspnea were clinically characterized and then randomized to receive either oral morphine or oral midazolam. Titration occurred in the clinic, and starting doses were 2 mg for midazolam and 3 mg for morphine, with incremental steps of 25% of the preceding dosing every 30 min. Reduction of dyspnea by 50% was the goal. Patients continued outpatient status during diagnostic studies; 31 patients with dyspnea entered the morphine arm, and 32 patients entered the midazolam arm. During the initial in-clinic phase, alleviation of dyspnea by 50% occurred in all patients, whether they received morphine or midazolam. At 3–5 days follow-up, the dyspnea intensity was less in the midazolam arm [numeric rating scale (NRS): 0–10; p = .0001–.0002], and these significant differences extended to breakthrough dyspnea over the same time frame in the midazolam arm. Patients tolerated both treatments well with mild somnolence being the most common adverse event. Neither morphine nor midazolam use led to needing additional diagnostic and therapeutic interventions. The study showed that midazolam was better than morphine for the immediate and long-term relief of dyspnea. 70 IN midazolam showed no clinical benefit for the management of dyspnea in one randomized, double-blind controlled trial. 86 Dyspnea scores did not differ between IN midazolam and placebo. Baseline anxiety levels were low. There were concerns about drug delivery in that it was difficult for participants to use spray bottles. 86
Seizures
Midazolam, as well as diazepam and lorazepam, are drugs most widely used as initial management for status epilepticus which is defined as seizures lasting more than 5 min or more than one seizure without recovery in between.87,88 Midazolam is one of the best studied drugs in the out-of-hospital setting. The RAMPART (Rapid Anticonvulsant Medication Prior to Arrival Trial) study identified intramuscular midazolam as being non-inferior to IV lorazepam in both adults and children for seizures persisting more than 5 min.89,90 Midazolam is versatile in that it controls status epilepticus by a variety of routes, including IV and subcutaneous routes. It is effective when given buccally, intranasally, or rectally. 91 Potential drawbacks when using the IN route include seizing patients spitting or blowing out medication during administration. 90 In the hospice setting, lorazepam or midazolam can be considered for status. Lorazepam may be favored due to its longer half-life, but as seen with the RAMPART study, both drugs are efficacious. 91
Analgesic effect
Ho and Ismail analyzed 13 randomized controlled trials (RCTs) looking at the analgesic effect of intrathecal midazolam. Studies suggest a delay in need of rescue analgesia in the postoperative setting. Intrathecal midazolam did not affect motor blockade. 92
Insomnia and terminal illness
Matsuo and Morita evaluated IV midazolam for insomnia in palliative care patients and found it to be as effective as flunitrazepam, but more costly. 93 Incidences of a hangover effect, delirium, treatment withdrawal, or death did not differ. Respiratory depression, defined as apnea, respiratory arrest, and decreased respiratory rate, occurred significantly more often in those receiving flunitrazepam than midazolam. Midazolam given subcutaneously works well also for insomnia in palliative care. 94
Delirium and agitation
Goncalves and coworkers 95 found the combination of intramuscular haloperidol and midazolam to control agitation in advanced cancer in 91% of cases. Agar and coworkers used midazolam as a rescue medication for refractory delirium. In that study, there were better outcomes in the placebo–midazolam rescue arm than the other arms which used antipsychotics and rescue midazolam. 73
Ketamine emergence phenomena
Midazolam has been used to treat or prophylactically treat emergence phenomenon associated with ketamine use. 96
Hiccups
Midazolam may be useful in the management of hiccups in terminal illness. 97
Pruritis and biliary obstruction
Prieto found the use of continuous infusion of midazolam to be effective in refractory pruritis associated with biliary obstruction. The original intent was to use midazolam for sedation given the refractory nature of the pruritis. Surprisingly, the pruritis improved and there was minimal sedation. Midazolam was started subcutaneously at 1 mg per hour after a 2 mg bolus. The dose was increased 1 mg every 15 min as needed for itching. During the next 4 weeks, the patient was slowly titrated to 84 mg/h of midazolam, with total control of his itching. 98
Muscle spasm
Parenteral benzodiazepines, such as midazolam, can be used to relieve muscle spasm and spasticity in the last days of life (Table 3). 27
Schedule of Administration.
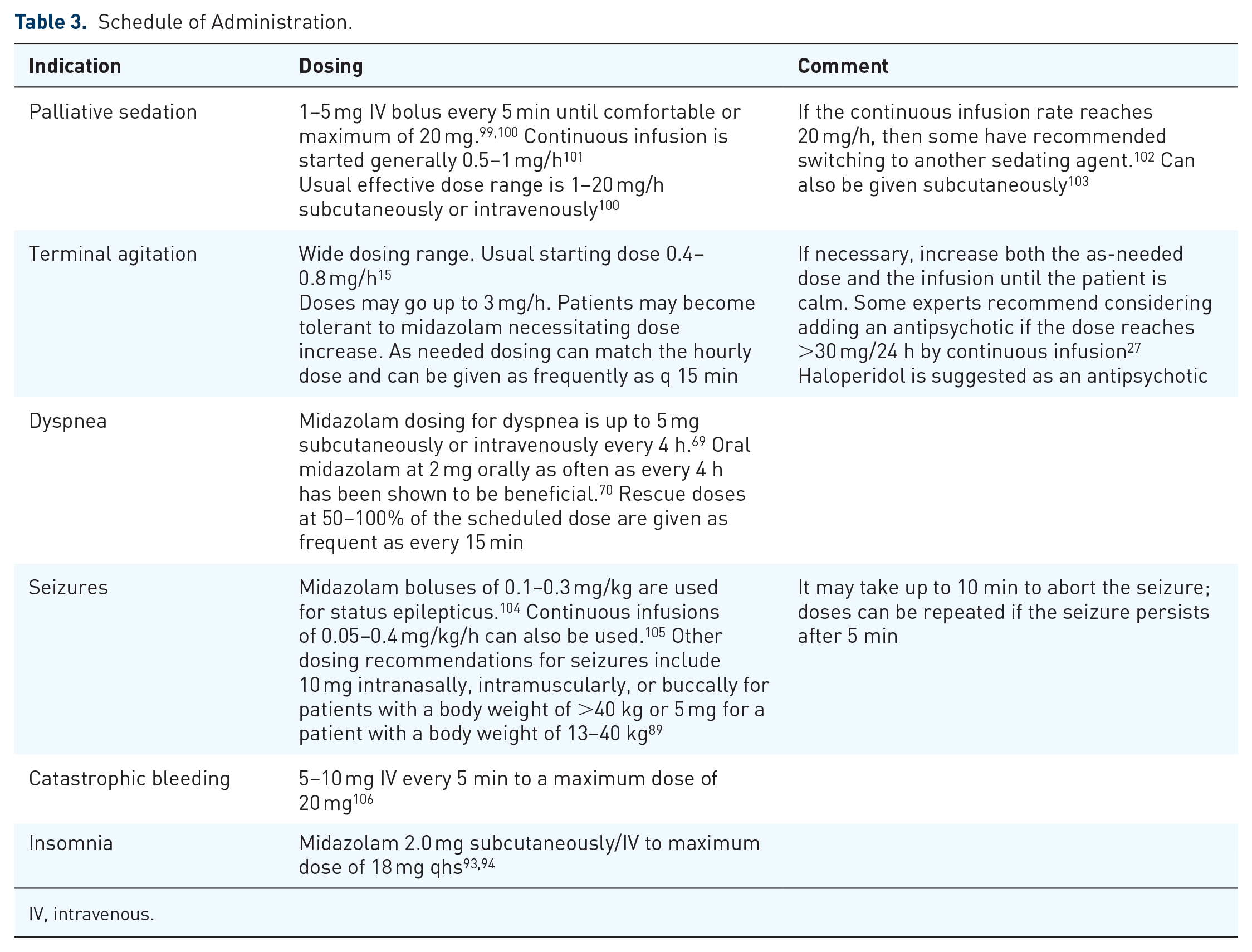
IV, intravenous.
Pediatric dosing
Dosing in children is weight based. 37 There is a fourfold variation in dosage administration (30–120 µg/kg/h) for children between the ages of 6 months and 12 years. In critically ill children, there is greater than fourfold variation in midazolam clearance. The greater variation in midazolam clearance values than the dosage schedule suggests that many children may receive too high or too low a dose of midazolam to obtain satisfactory sedation. This may explain the poor sedation achieved in clinical trials with midazolam in critically ill children. As a group, pediatric patients generally require higher dosages of midazolam hydrochloride (mg/kg) than do adults. Younger (less than 6 years) pediatric patients may require higher dosages (mg/kg) than older pediatric patients and may require close monitoring. Midazolam should not be administered by rapid injection in the neonatal population. Severe hypotension and seizures have been reported following rapid IV administration, particularly with concomitant use of fentanyl. 107 Doses given to children must be calculated on a mg/kg basis. For children 6 months to 5 years of age, a dose of 0.05–0.1 mg/kg is recommended. Dosages up to 0.6 mg/kg titrated slowly may be necessary to achieve the desired endpoint. For children 6–12 years of age, the recommended dose is 0.025–0.05 mg/kg with doses up to 0.4 mg/kg to achieve the desired endpoint. 14
Route conversions and conversions from other benzodiazepines
Converting midazolam from the oral to IV/subcutaneous route uses a 2:1 ratio.22,108 Midazolam’s potency in comparison with other benzodiazepines is shown in Table 4. 27 This may be useful when switching from one benzodiazepine to another when greater clinical efficacy is required.
Benzodiazepine Equivalents. 27

Pharmacoeconomics
The cost of giving midazolam given by IV injection/subcutaneous injection ranges from 1.75 to 8 US dollars/dose depending on concentration. This is comparable with the cost of IV Ativan. 109
Conclusion
Midazolam is a benzodiazepine with sedative, anxiolytic, muscle relaxant, and anticonvulsant properties. Its lipid soluble properties allow rapid action. Advantages also include the ability to be given by multiple routes and its short half-life. The short half-life allows for reversibility of drug effect if desired. Clinicians should consider this drug when there is a need for a short-acting, rapid-onset benzodiazepine. As a versatile drug, it is used for the management of palliative sedation, terminal restlessness, seizures, and dyspnea. It can be used to manage anxiety and symptoms of dyspnea in the setting of withdrawal of care and catastrophic bleeding. Disadvantages of the drug include propensity to be rapidly metabolized with continued use.