
Abstract
Background:
Reminiscence is used in a range of different interventions in palliative care, for example, Dignity Therapy or Life Review. However, literature has focused mainly on the methodology, and little has been published on patients’ priorities and primary concerns.
Objective:
This study looks at themes emerging in a reminiscence intervention with patients confronted with a life-limiting disease. Interviews were audiotaped and transcribed verbatim. Transcripts were analysed using thematic analysis.
Setting/subjects:
Seventeen patients who were receiving palliative care at the University Hospital Bonn participated in interviews reviewing parts or phases of their lives.
Results:
Patients expressed satisfaction and a sense of well-being with the intervention. Major themes emerging in the interviews were the factors involved in the development and expression of personality, such as character-forming influences, self-image, self-awareness, and philosophy of life. Talking about personality was entangled with influences from growing up, qualification/job, partner/spouse, children, resources, twists of fate/crossroads, and coping.
Conclusion:
The topics emerging from the interviews differed from the scope of guiding questions in common reminiscence methods like Life Review or Dignity Therapy. The underlying motivation of patients seemed to be the search for identity and continuity in one’s life.
Introduction
The major tenet of palliative care is the holistic treatment of the whole person encompassing physical, psychological, emotional and spiritual needs. 1 Psychosocial needs have always been included in the scope of a multidisciplinary team. Physicians, nurses, chaplains, social workers, psychologists and volunteers support the patient in adapting to and coping with the progression of the disease by various means. Studies with interventions comprising biographical elements are efficacious in increasing spiritual well-being and decreasing depression.2–13 Reminiscing is described as having social, instrumental and integrative functions. Sharing personal memories is bonding people. Looking at challenges in the past could help cope with the present and reminiscing might help to continue or adjust one’s identity. The authors describe biographical narrations as a process providing life with a sense of purpose and unity. Life narratives create a ‘narrative identity’ which helps with psychological adaption and development in existential crisis. 14 These findings are confirmed by a study from Romanoff and Thompson 15 who state that narratives could help to find meaning at the end of life. Webster and colleagues described functions of reminiscing as preparation for death and maintenance of identity. Personal memories are indispensable in the provision of sense of coherence, meaning of life and sense of self, and they have a positive impact on mastery and self-esteem. 16 Processes such as enhancing meaning in life, preserving a sense of control and promoting acceptance and reconciliation that are discussed in these studies also contribute significantly to coping. 13 Reminiscence interventions also improved ego-integrity and reduced depression. 17 However, cultural factors seem to have a major influence on the topics patients prioritize. We conducted a systematic review 18 and found only one article about primary concerns of patients. It was a multisite study in Japan, Korea and America of Ando and colleagues 19 who found a broad range of concerns with major differences between countries. Webster and colleagues 16 suggest a high impact of ethnicity regarding the emphasis on the individual or the collective. Common reminiscence interventions such as Life Review or Dignity Therapy have a range of guiding questions, for example, on accomplishments in life, favourite roles and significant events. These questions may focus the reminiscence intervention on topics that are less relevant for the patient and thus prevent benefit from the intervention or even provide a barrier to participate. 20
There might be an impact of different cultures on the topics raised by patients. This suggests the assumption that transferability of interventions might not be given and need to be tailored. To adjust established approaches such as Dignity Therapy, we need to know about primary concerns of patients. To our knowledge, no previous studies have described German patients’ preferences and priorities expressed in a reminiscence intervention. Therefore, the purpose of the present study was to conduct a qualitative evaluation of biographical interviews with patients treated in a palliative care unit in Germany to gain deeper insight into their primary concerns when asked to reminisce about their life.
We used a qualitative evaluation of biographical interviews with patients treated in a palliative care unit in Germany to gain deeper insight in their primary concerns.
Methods
This study aimed to find priorities and primary concerns of patients with a life-limiting disease. The intervention focused on simple reminiscing as described by Webster and colleagues, 16 based on an interview and producing a legacy in the form of a letter or a story for the loved ones. The main focus was to avoid any control. Patients were free to talk about any subject they wanted. As in the study of Allen and colleagues, 10 interventionists were graduate students who received intensive training, monitored and supervised by a medical psychotherapist and a physician. Training comprised reading materials, structured role-play and teaching content (knowledge on palliative care, biography work, interview techniques, transcribing and writing).
Setting/participants
The participants were recruited from the departments of palliative medicine and radiotherapy of the University Hospital Bonn. The inclusion criteria for this study were as follows: (1) patients informed about their life-limiting disease, lack of curative treatment options and prognosis, (2) fluent in German language, (3) 18 years of age or older and (4) no psychiatric impairment such as dementia, psychosis, severe depression or diagnosed personality disorder. Patients were recruited by a social worker, a nurse or a psycho-oncologist. Patients who met the criteria for the study were asked whether they were interested in participating. One of the authors (M.H.) explained the project in detail for written informed consent. Data were collected between January and May 2017. The research ethics committee of the University Hospital Bonn reviewed and approved the study (no. 335/16).
Data collection
The interviews were unstructured with open-ended questions such as ‘What do you want to tell us about your life?’ to provide a story-telling setting. Interviewers encouraged patients by active listening, mirroring answers and reflecting emotions. We had no other prompts and decided not to use questions from Dignity Therapy or Life Review to avoid cultural biases. Lindqvist and colleagues 20 raised awareness for reflection of the interview as a social situation following social conventions. They saw ‘collisions between the norms and values of participants- on cultural, class and individual levels- and those underlying the DT protocol’. Stating Romanoff and Thompson 15 who conclude in their study, ‘The telling of the story to a willing, nonjudgmental companion acknowledges existing meanings and enables the construction of new meanings that may alleviate suffering’. Therefore we decided to use a simple reminiscence as described by Webster and colleagues. 16 Interviews were conducted in hospital or as an exception at the patients’ home following discharge from hospital. After the intervention, a researcher (M.H.) visited the patients to get feedback on the intervention. A written narrative from the audiotaped interview was constructed which was then presented to the patient as a little booklet. Health status declined very quickly for some patients who were very weak. Five patients died unexpectedly soon after the interview before the booklet could be presented to them, and the legacy document was presented to the next of kin instead. Only three patients were able to receive their legacy document themselves. Analysis is restricted to the interviews.
Analysis
The interviews were audiotaped and transcribed verbatim. We restricted our research on qualitative evaluation of patient interviews to gain deeper insight in primary concerns. Transcripts were analysed using thematic analysis 21 with the software MAXQDA-11. Thematic analysis was chosen as a method for identifying and analysing themes within the data. The main interest was to reflect the reality of the participants. Analysis followed an inductive and semantic approach as described by Braun and Clarke. 21
For generating initial codes, the entire data set was checked systematically. Relevant data were collected for each code. Two of the authors (M.H. and G.A.) assured that no new codes derived from the data. In a second step, codes were categorized into themes. M.H. and G.A. reviewed themes independently checking the entire data set and generating a thematic overview. Clear definitions and names for each theme were generated and if necessary, discussed until consensus was reached. Inter-coder reliability 22 was demonstrated twice during the coding process This took place at two time points in analysis when generating initial codes, and when defining and naming themes. M.H. and G.A. were familiar with the entire data set and discussed initial codes and themes till consensus was reached. All consolidated criteria for reporting qualitative research (COREQ) were considered. 23
Results
Twenty-three patients were asked for participation, of which two rejected because of time constraints related to their therapies and two others felt too weak. Therefore, a total of 19 patients were included. Two patients dropped out due to a declining performance status after inclusion. Hence, 17 interviews were conducted (response rate: 0.739) (Table 1).
Sample.
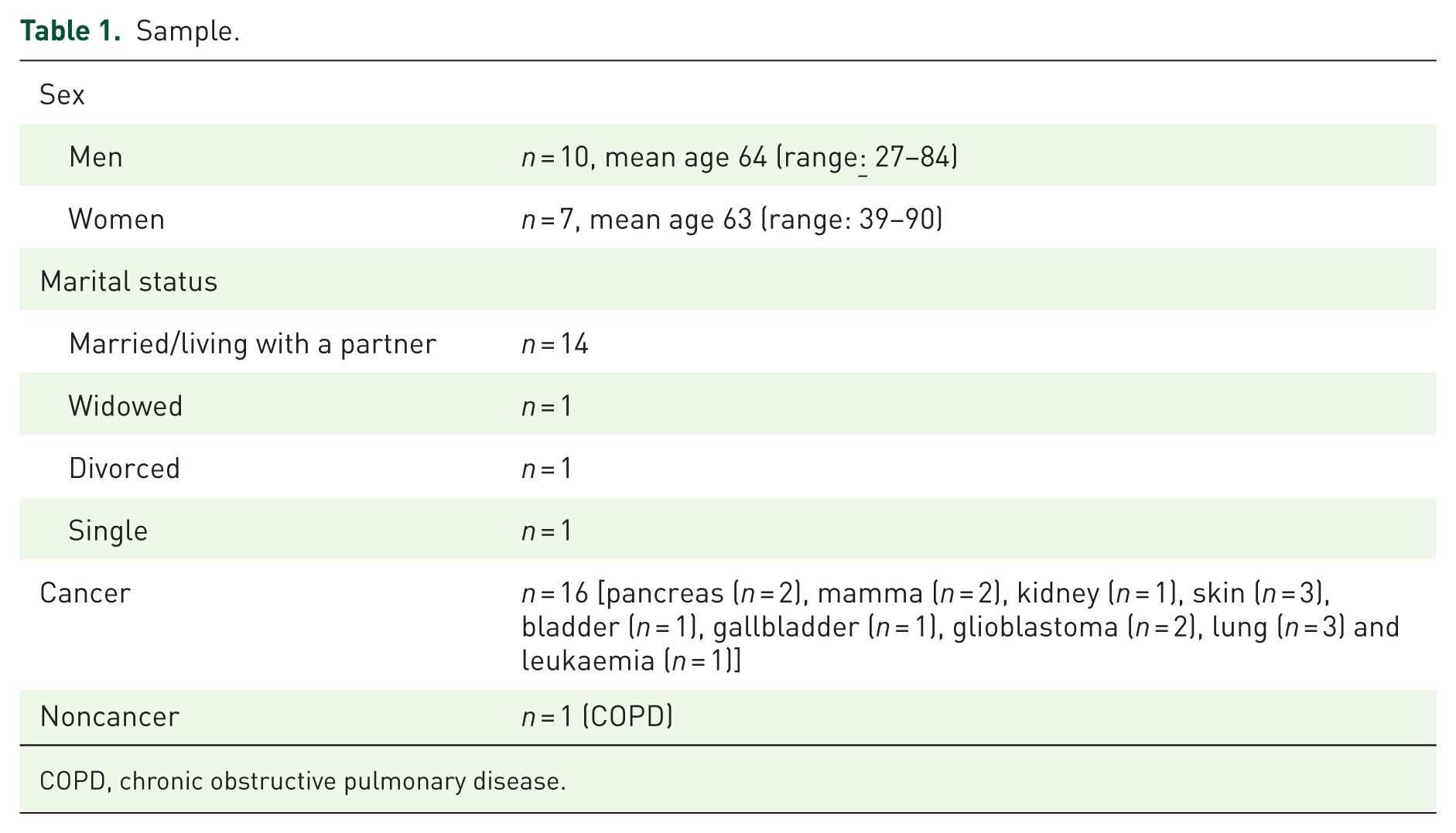
COPD, chronic obstructive pulmonary disease.
In 4 of the 17 interviews, a family member was present during the interview as requested by the patient. The duration of the interviews varied between 50 and 170 min in one or two sessions, the average interview length was 94 min.
Identified themes were personality, resources, growing up, qualification/job, spouse/partner, twists of fate/crossroads, coping and children.
Patients set these themes in context with their personality: what had influenced it, how and why they act as they do, how they became the person they are now and what they think about life. Everything was to a lesser or greater extent an explanation, and an illustration of how things influenced the course of life and their character. ‘Personality’ was the most commonly mentioned theme, highlighted by all participants in their biography: Somehow it was my mistake that I never got far in my career. I mean it is obvious that afterwards I never got a second chance. Through all the phases I was always stressed and I wonder if my way of life was at fault. Foreign languages have always been part of my life and through them I developed self-confidence. I blame myself and think a lot about my life. On reflection I did not take my chances. (PST, m, 60–70) My life had a lot of repeated challenges, including financial ones. I had to pay child support. I lost my house through my divorce. The majority of my life was work. I worked much more than others. I started at six in the morning and worked till ten at night, including Saturdays. That is why I am where I am today. My house is paid off now and I had to work hard for it. Today I say to myself, I did it right. (PSCH, m, 50–60) I do everything possible and take every chance I get. I never give up – I never have. I am not that kind of person. I will fight my way through to get what I want if necessary. On the other hand, I am a calm and good-tempered person, but if someone is lying to me or betraying me, I get very cross. I am always very honest and say what I am thinking. I expect others to be honest with me as well. Giving up doesn’t come into question, even if I have to go on all fours. (POC, f, 60–70) My daughters told me that I should have been stricter. I suppose you can never do everything right. I know that, but every mother tries her very best. I think I acted in that manner because I was never allowed to make my own decisions. I was not allowed to go to university. I had to do the apprenticeship. I always had to obey. Therefore, I wanted to make it different for my own children. I always said, my children can decide for themselves what they want to do. (PK, f, 60–70) School was crowded and full. I even had to bring my own chair. There were no books, just copied sheets of paper. At the beginning it was terrible. The war was just over, and the teachers had just been demobilised. They were not very friendly. It wasn’t great. I had to fight my way through. My father helped me with everything, he organised the chair and helped me get by, also in other things like English and French. I could always count on him. (PG, m, 80–90) My father died when he was 62 years old, but he had been bed-ridden for nine years before that and we cared for him at home. He became ill when I was 12 years old and died when I was 21. These years formed my character. I was a good boy and I always did a lot of sports. I was brought up in a village with all my family around, just as it is in a village. It was hard being without your father in adolescence. My father was really ill and suffering. He cried a lot and had a lot of pain, but he did not whine. He had a fighting spirit and I am like him in many ways. He told me, you are as strong as you want to be. This phrase has always been very important to me. (PHS, m, 50–60)
Some of the illustrative quotes reflect themes such as qualification/job, coping, children and growing up. Talking about qualification/job predominantly was seen in the meaning of facing challenges in life (‘I never got far in my career’). Coping capacities as a good character trait (‘I was a good boy’) were related to social bonds or to assure the unity (‘He had a fighting spirit and I am like him’) and coherence in own behaviour. Interestingly talking about the father was a predominant issue in ‘growing up’ narrated by men. These narrations were very emotional and vivid. The father seemed to have an outstanding importance, whereas there was no explicit narrative about the mother. Topics related to resources such as spirituality, pets, friends, hobbies and travels were seen as a function of bonding (see Table 2). Mastery could be seen when patients described how they tried to keep control using strategies and by relying on their principles (I never give up – I never have./you are as strong as you want to be).
Step 5 of Thematic Analysis: Defining and Naming Themes.

The spectrum of participants’ narratives showed how they describe the development of their own personality and how they tried to find continuity and identity of self.
Discussion
Our analysis of the data showed that the predominant theme of the patients’ narratives about their life was their personality, their sense of self and self-worth. All interviewees described how they became the person they are. Stories of patients were in most parts reflections of life rather than numeration of events. Our findings correspond with the description of the outcome of Life Review described as helping people gaining insight into their development throughout their lives. 16
Identity and meaning belong together, as stated by Weiher 24 from evaluations in spiritual care. Story-telling seems to evoke justification of how things turned up in life and to look for meaning in the things that happened. None of the patients mentioned the term ‘meaning’ explicitly. They also did not talk about their belief or lack of belief in meaning or that the world was fair or just. Nonetheless the construction of continuity in the stories told seemed to be a search for meaning. There is a great body of research regarding meaning. Park and colleagues described inconsistent research findings on the role of meaning making in psychological adjustment. They distinguished between meaning making and meaning made. Meaning making was defined as understanding of a stressor as appraised meaning and incorporation of this understanding in a global meaning system. Meaning made was defined as growth, life meaningfulness and reduced inconsistency of just-world beliefs. 25 The importance of meaning was highlighted in several studies by Breitbart and colleagues on dignity therapy. They demonstrated that quality of life is mainly influenced by patients’ sense of meaning and purpose in life.12,26
This corresponds to Seligman’s definition of a ‘full life’ described with the components: positive emotions, engagement and meaning. 27
There seemed to be a great need to gain an understanding of existential issues, such as the sense of one’s own place in the world. This finding corresponds with Frankl’s 28 theory of humans striving for meaning as the primary motivational force. Associated with meaning is the sense of coherence 29 described as a feeling of confidence that life is comprehensible, manageable and meaningful. The sense of coherence evokes resilience and coping, 16 and this might be one reason for patients’ benefit of therapies using biographical approaches.
Successful coping became obvious in the description of twists of fate or crossroads and the appraisal of life by the patients in our study. The studies by Westerhof and colleagues confirmed the instrumental and integrative functions of reminiscing by fostering coping. They concluded that reminiscing had an impact on psychological resources such as social support, mastery, coping, meaning in life and self-esteem. 14 Research in gerontology found a relation between reminiscence and mental health comprising meaning in life, mastery and positive thoughts. 16 The feeling of mastery in turn facilitates the positive effects of life review interventions in general as Korte and colleagues 30 demonstrated. Constructive reappraisal was described as an identity function of reminiscence. The identity function seemed to be the most important factor for patients in our study. Whatever topics the patients selected, the underlying tenor was their maintenance of self. Personality and identity are not in the focus of the guiding questions of reminiscence interventions but might well be worth consideration.
Dignity Therapy 31 has demonstrated to be effective for an increase of well-being and decrease of depression.5,6 The component of legacy creation is suggested to achieve higher scores in generativity and ego-integrity. 32 The idea of a legacy seemed to be helpful for patients. Interviewees in our study were asked to tell their stories to be printed in a little booklet or written as a letter. We expected that patients wanted to leave a story to their loved ones. However, it turned out that leaving a legacy was rarely a theme in the interviews though we found it more often hidden in the patients’ attitudes. Men were more often convinced than women that they lived a life that was worth to be recorded and three patients had already begun to write up episodes of their life. In contrast to the study of Hack and colleagues, 33 who looked at life reflections gleaned from Dignity Therapy, we cannot affirm that patients expressed wishes and gratitude to others. Maybe this was related to the different intervention approach. Hack and colleagues 33 described core values that were predominantly mentioned by participants such as family, pleasure, caring, sense of accomplishment, true friendship and rich experience. These topics show little congruence with our main themes. Participants in the study by Hack and colleagues were from Canada and Australia, compared with our German sample. This could indicate the cultural impact on patient priorities in palliative care settings similar to the findings of Ando and colleagues describing great differences in the prominent topics of terminally ill cancer patients from Japan, Korea and America. In that multisite evaluation of Short Life Review, Americans were interested in love, pride, will and good memories; Koreans in religious life, right behaviour for living and strong consideration for children and will; and Japanese in good human relationships, transcendence, achievements and satisfaction. 19 We did not find any of these themes in our German palliative care sample.
The analysis of data suggests differences on emerging themes related to sex. The influence of sex on the priorities of advanced cancer patients was already described by Ando and colleagues. 34 In our study, the role of the father as contributing to identity and personality was prominent in the narratives of male patients. There is a heuristic model of reminiscence in gerontology pointing out that self-narratives have different functions in which age and sex moderate memories. Reminiscence as life-span process was influenced by triggers, modes, contexts and moderators. In the research on ageing, the influence of sex on reminiscence was complex but inconsistent, whereas the influence of age was prominent in all evaluations. 16
Further research is needed to disclose the potential value of identity-related questions and cultural differences in reminiscence interventions. In addition, research should explore if interventions need to be tailored to cultural perceptions and expectations. Biographical interviews seem to foster the search for identity and ego-integrity, so further studies will be needed to investigate the influence of biography work on concepts related to identity and meaning making, such as sense of coherence, resilience and coping.
Our study confirmed that patients search for identity and found the biographical intervention helpful and beneficial. Short reminiscence interventions such as the one described here are necessary in the holistic approach of palliative care to improve patients’ well-being.
Study limitations
The unstructured interviews allowed patients to talk about any subject but made analysis difficult. However, in spite of this restriction, we found similar interview sequences and adequate comparability of the interviews. While initial codes and themes were discussed by raters until consensus was reached, no inter-rater agreement scores were calculated. The study was conducted at only one site. Patients were selected for the intervention by staff members of the palliative care team, resulting in a convenience sample and thus prone to bias. The sample showed a distribution of diseases and demographic data common in palliative care, with all except one patient suffering from cancer. Two patients dropped out after inclusion in the study, which is an anticipated number for patients receiving palliative care. The sample size was small and thus results may not be representative for palliative care patients in other clinical or cultural settings.
The cultural differences we have suggested as an explanation of the findings in our study may also have been related to differences in the methodology compared with other studies, as our data have been elicited by simple reminiscence, whereas other studies have used Life Review and Dignity Therapy. However, the impact of different cultures on topics raised by patients in a life review intervention also has been described by Ando and colleagues 34 and Webster and colleagues. 16
Conclusion
Although there are some limitations, our study provided insight in patient priorities and primary concerns when talking about their life. Patients appreciated the attention they received, and bereaved families gave positive feedback and told us how happy they were with the written booklet. Simple reminiscence seems to focus on personality in our German sample of palliative care patients and to foster looking for identity and maintaining mastery. Analysis of data suggested a cultural impact. Reminiscing interventions using guiding questions might need to be adjusted for the specific cultural and medical setting.
Footnotes
Acknowledgements
We would like to thank the patients for participation in this study. Our special thanks go to Annette Zdarsky for proofreading the transcripts.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.