
Abstract
Background:
Sex and gender are determinants of health and well-being. A person’s sex is assigned at birth while gender identity is culturally determined and influences many aspects of life. Little evidence exists regarding differences in the use or experience of palliative care services between people of different sex and genders in the United Kingdom.
Aims:
To explore differences by sex and gender in (1) time from service referral to death, (2) reason for referral, (3) preference for place of death and (4) place of death in UK hospice and community services. In addition, palliative care staff’s views of the impact of sex and gender on end-of-life experiences are explored.
Design:
Sequential multiple methods design including a service evaluation of routinely collected data from hospices and community nursing services across the United Kingdom (January 2019 to December 2022) and a qualitative study. Quantitative data were extracted from a central database, which collated all data from SystmOne, PatientConnect and EMIS and were summarised using descriptive statistics. Focus groups were conducted with palliative care staff from Wales and Scotland and analysed using reflexive thematic analysis.
Setting:
Hospice inpatient services, community nursing teams.
Results:
Ninety thousand six hundred and fourteen data points were analysed. High levels of missing data were noted around gender identity, alongside other demographic characteristics. A roughly even split between male (50%) and female (47%) patients was observed. Gender identity was not reported for 25% of the sample. The majority of patients were White British (82%). No differences were noted in other variables explored. In the qualitative study, differences by gender were percieved by palliative care staff in relation to patient and carer experiences.
Conclusion:
Quantitative data suggest limited differences in access to care or service use while qualitative data suggest differences in experiences of palliative care between sexes and genders. To enable explorations of intersectionality, sensitive data collection is needed to support future research and service delivery.
Plain language summary
A person’s sex is assigned at birth, while gender identity is culturally determined. There is evidence that people of different sexes and genders experience and access health care in different ways. This study looked at two different types of data to find out whether there were any differences in how people of different sexes or genders accessed or experienced specialist palliative care. The first part of the study looked at data that was collected by hospices and community nursing services across the UK. We compared different outcomes between people that were identified as being either male or female sex. We noticed that very little data about people’ gender identity was collected. Very few differences were noted across the variables we looked at.
In the second part of the study, we spoke to staff who worked in hospice and community nursing services in Wales and Scotland. We asked them to tell us whether, in their experience, they noticed any differences in how males and females experienced or accessed care. We were interested in the experiences of both patients accessing services, and the people close to them. Unlike in the routinely collected data, we heard in our conversations with staff that there may be some differences in how and when males and females access care. We also asked staff about how they collected data about patients, including things like gender identity. We heard that staff were sometimes worried about saying the wrong thing and offending people. They also felt that they had limited experience of supporting people who were trans or gender diverse. This study highlights the importance of making space for and supporting all aspects of an individual. Sensitive data collection is one step in the path to achieving this.
Introduction
A person’s sex (male or female) is assigned to them at birth according to their primary sex characteristics (genitalia). Gender identity is culturally determined, can be fluid and can be expressed on a scale of masculinity, femininity and/or gender neutrality. 1 In this paper, the term “male” refers to cis male and “female” refers to cis female, unless stated otherwise. The term cisgender describes a person whose gender identity corresponds to their sex assigned at birth. The terms transgender and gender diverse are used when referring to people who do not identify as their assigned sex as birth.
Internationally, research exploring sex differences in health care suggests females have a longer life expectancy than males but may live a greater number of years with a disability. 2 Females are also more likely to be widowed and live alone, with loneliness linked to poorer experiences at the end of life. 3 However, the underrepresentation of females in health research has been well documented.4,5 In a trial looking at palliative care for people living with heart failure, females experienced greater symptom burden and poorer quality of life than males, suggesting that sex-specific approaches to palliative care may be needed. 10 Sex differences in pain, 11 nausea 12 and fatigue 13 have also been reported at the end of life. Males have been shown to opt for more aggressive and life-sustaining treatment, while females have been found to be more likely to opt for palliative care14,15 and have an advance care plan16,17 in some studies. Evidence regarding the impact of gender on access to hospice care is mixed 18 with some studies indicating women are more likely to access hospice care than men, others suggesting the reverse and others indicating no differences.
Trans and non-binary people often face multiple barriers in accessing health care generally. 6 Cis normative ideologies mean that the trans and gender-diverse populations are often not represented in research, education or healthcare design. There is a growing body of research calling for greater exploration of gender and sex differences in palliative and end-of-life care.7–9 Specific barriers to accessing palliative and end-of-life care for trans and non-binary people have also been described in the literature.19,20
Differences in experiences towards the end of life have been linked in part to social constructs and expectations around gender roles, 8 as well as previous, mostly negative experiences of accessing health care for people who are trans or non-binary. 21 Whilst the sex or gender of the patient is thought to influence experiences at the end of life, so too does the sex or gender of the informal caregivers surrounding them. Gender disparities in both receiving end-of-life care and supporting others have been shown to disadvantage both males and females but in different ways. 8 Females are more likely to be caregivers than males 22 and female caregivers experience greater financial strain, 23 poorer psychological well-being, and less support than males. 24 However there are inconsistencies in the evidence around gender differences in care giving, suggesting that gender may only explain a proportion of the variance in outcomes. 22 One lens through which to consider these differences is that of intersectionality. As a theory, intersectionality provides insight into how multiple systems of oppression mutually intersect to impact on health and well-being. 25 Two recent systematic reviews26,27 highlighted the potential for intersectionality theory to inform future research and practice in this field, but both pointed to a lack of consideration of the impact of intersectionality on end-of-life experiences to date. A US-based study exploring middle-aged and older adult heterosexual and lesbian women’s views of hospice and palliative care found that no differences among people with different sexual orientation but notes that older women held more positive beliefs about hospice care and reported more comfort discussing pain management than middle-aged women. 28
The current study aims to encourage and inform discussions regarding gender-sensitive policies and practices within palliative and end-of-life care by reviewing sex and/or gender differences in specialist palliative care use and the views of palliative care staff.
Research questions
Are there any differences between sexes with regards to reason for referral, time from referral to death and preferred and actual place of death?
Do clinical staff from hospices and community nursing services in Scotland and Wales consider sex and/or gender identity to be influential in experiences towards the end-of-life?
Methodology
Theoretical underpinning
This study incorporates intersectionality theory 25 with critical realism as its philosophical framework. 29 This epistemological position enabled both individual meaning-making and wider social context to be considered in the interpretation of data generated. Additionally, what is commonly defined as reality was maintained, placing the narratives in a socially constructed framework.
Researcher characteristics and reflexivity
The authors of this paper are researchers and policy managers who all identify as female, whose interests centre around equity in palliative care and who are directly or indirectly affiliated with the organisation from which data were collected and have varied personal experiences of informal caregiving. E.W. and B.E. were known professionally to some participants.
To maintain objectivity, a steering group was assembled involving people with lived and professional experience of palliative and end-of-life care. This group contributed to the interview guide and interpretation of data collected. The research team also kept reflective notes and engaged in peer debrief sessions at regular intervals, via the steering group. Through these practices, the team’s preunderstanding enhanced its relevance without compromising the project’s rigour.
Design
A sequential multiple method design 30 including a service evaluation and a qualitative study.
Setting
The service evaluation included data from hospices and community nursing teams from a palliative care provider operating across the United Kingdom. The qualitative aspect included hospice and community nursing staff from the services of the palliative care organisation that were located in Wales and Scotland.
Study population, sampling and recruitment
The service evaluation utilised routinely collected data of all referrals made to hospices and community nursing services within a large UK-based palliative and end-of-life care provider.
Purposive sampling identified staff from a range of clinical backgrounds, within hospices and community services in Wales (Cardiff and the Vale) and Scotland (Edinburgh), to take part in online focus groups. An invitation was circulated via existing email mailing lists. The email contained a participant information sheet and a link to an online consent form (REDcap), which was completed ahead of data collection.
Patient and public involvement
Four members of the public; three bereaved caregivers, and one person living with a terminal illness were part of the project team. They contributed to the development of the application for funding, reviewed study documents and shared their reflections on emerging findings in the context of their own experiences during steering committee meetings.
Ethical considerations
Ethical approval for the qualitative study was obtained from the UCL research ethics committee (8675/004) on 21 September 2022. Research governance and data protection approvals were sought for the service evaluation. Electronic informed consent was obtained from all focus group participants.
Data generation
Service evaluation
Data were collected retrospectively for all patients referred to a hospice or community nursing services from a large UK palliative and end-of-life care provider between January 2019 and January 2022. Data were extracted from a central database which collated all data collected by staff in SystmOne, PatientConnect and EMIS. This was provided in an anonymous Microsoft Excel sheet to the research team including demographic variables (sex, gender identity, age, ethnicity, sexuality, religion), primary diagnosis, reason for referral, reason for admission, length of stay and preferred and actual place of death. The level of missing data relating to gender identity prevented a quantitative analysis of gender, the analysis was therefore based upon recorded sex.
Qualitative study
A topic guide for the focus groups was produced by the research team, including PPI representatives, and was developed based on existing international evidence around gender inequity combined with the aims of the study (Appendix 1).
Four online focus groups were conducted in December 2022 on Microsoft Teams, two with staff in Scotland (Edinburgh) and two with staff in Wales (Cardiff and the Vale). Focus groups lasted up to 60 min (range 45–60 min) and were audio recorded and transcribed verbatim. The authors made use of reflexive notes and peer debriefing following each focus group. The Sex and Gender Equity in Research (SAGER guidelines) 31 and The Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement 32 informed the conduct and write up of this research (Supplemental Material).
Data management and analysis
Quantitative data were collected and analysed first, with a view to exploring any observed differences between sexes through the qualitative work.
Service evaluation
Data were checked for consistency and accuracy. Seven observations were deleted for the variable “age” as the inputted value was greater than 150. For the survival length data, some of the values were negative, suggesting a patient died before being referred to the service. After discussing with the steering committee, these data points (n = 1006) were deleted from the analysis. The “reason for admission” was the first reason recorded for that data point, often patients had multiple reasons. This variable was not a pre-defined list of responses. Therefore, individual responses were categorised through discussion with a palliative care research nurse, to ensure clinical validity. Data regarding preferred and actual place of death were cross-tabulated to generate a new variable of whether the patient died in their preferred place.
Univariate analysis was conducted on all data. Frequency counts were generated for nominal and ordinal variables (n, %). For interval-ratio variables, descriptive statistics were presented as median, range and interquartile range. Data were analysed in STATA 17 (StataCorp. 2021).
Qualitative study
Reflexive thematic analysis was utilised for this analysis as it “emphasises the importance of the researcher’s subjectivity as an analytic resource, and their reflexive engagement with theory, data and interpretation.” 33 This was pertinent as the study aimed to generate evidence with the potential for policy impact, and the research team and steering committee were comprised of both researchers, policy managers and people with lived and professional experience of palliative care, all of whom contributed to the analysis.
Qualitative data generated in this study included the transcripts of focus groups, notes from the peer debriefs held between the research team following each focus group, as well as reflexive notes from each member of the research team. All qualitative data were analysed as a single dataset using the six phases of Braun and Clarke’s reflexive thematic analysis. 34 Initial line by line coding of the data was undertaken in NVivo 1.2 (Lumivero) by B.H. to explore accounts of experiences and observations regarding the impact of gender, whilst also considering the impact of the systems and contexts in which participants worked. 35
Initial themes were refined through discussion with the steering group. During these initial discussions, initial themes were presented, along with supporting quotes. Steering group members when then invited to reflect on and discuss these themes and contribute their own lived and professional experiences. These conversations shaped and named final themes, which were presented back to the steering group and are presented in this paper.
Results
Quantitative data
In total, 90,614 data points were received from participating hospices and community nursing teams from England, Scotland, Wales and Northern Ireland. Table 1 describes the characteristics of the patients referred to services. Overall, there was an even balance between the sexes across all four nations. In terms of gender identity, 25% of data were missing. The data that were reported were either female/feminine gender (36%) or male/masculine (30%). There was a substantial amount of missing data reported across all variables. For 95% of data points regarding sexuality, there were missing data. For ethnicity, 35% of the data were either missing or not known.
Patient characteristics.

Are there differences in sex between the reasons for referral?
Given the amount of missing data regarding gender identity, the results were explored for differences between people of different sexes. Admission avoidance was the primary reason for first referrals to the services (30%). In 44% of data points, the reason for referral was missing. Table 2 describes the reasons for referral by sex. Overall, the proportions were evenly matched across the sexes.
Reason for referrals by sex.
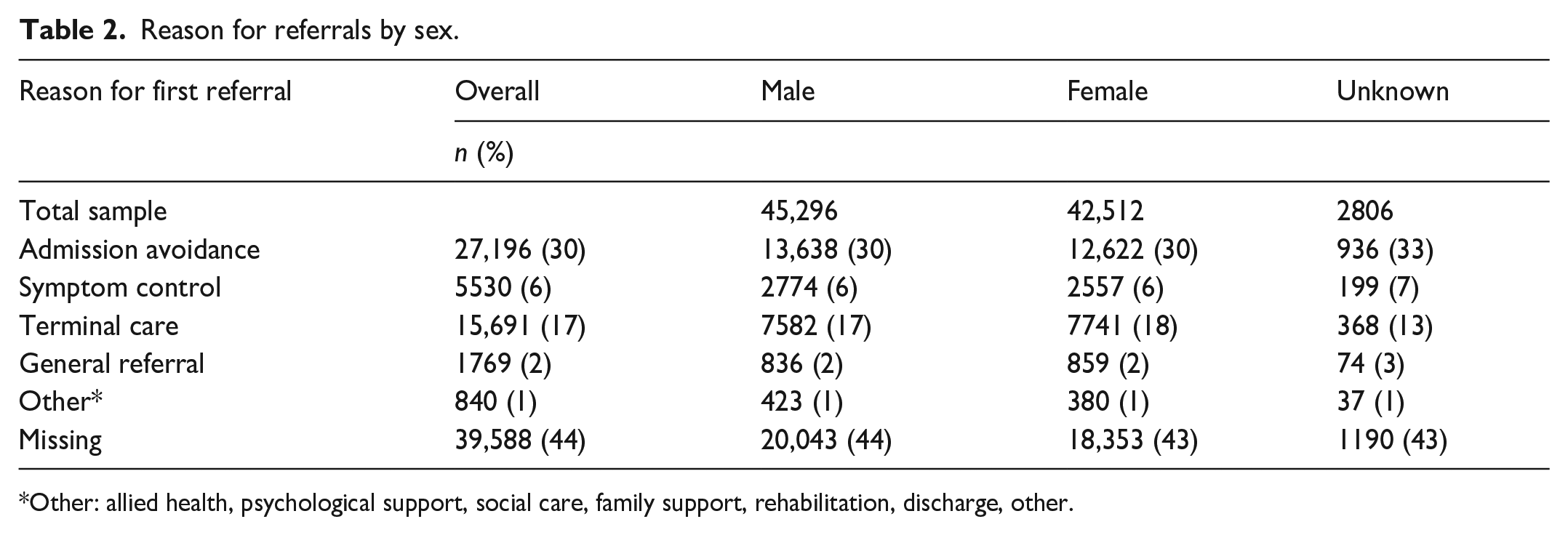
Other: allied health, psychological support, social care, family support, rehabilitation, discharge, other.
Is there a difference in the time from referral to death between sexes?
Table 3 displays the average time a patient lived for after being referred. There was strong evidence that females had a survival length of 2 days more compared to males (95% CI: 1.18–2.87, p < 0.001). Furthermore, there was strong evidence that those whose sex was not recorded had a survival length of 7 days less compared to males (95% CI: −9.66 to −4.78, p < 0.001).
Length from referral to death.

Denominator changed now as 1006 observations deleted (now = 89,608).
IQR, interquartile range.
Is there a difference between preferred and actual place of death between sexes?
Table 4 describes the proportion of preferences of place of death and actual place of death by the sex of the patient. For males and females, the preferred place to die was at home. The actual place of death for males and females was predominately home, 66% and 65%, respectively. When it came to achieving the preferred place of death, 62% of males and females died in their preferred location. For those where the sex was not recorded, 56% achieved their preferred place of death.
Preferred, actual and achieved place of death by sex.

Qualitative study results
Given the high level of missing data observed in relation to gender identity, the focus groups asked participants to reflect on how data relating to these variables is collected and stored in existing systems. Focus group participants were also asked to reflect on whether the quantitative data reflected what they observed in practice, in relation to the spilt between males and females accessing their services, and observations regarding differences in experiences of people of different genders who access their services, either as patients of informal caregivers.
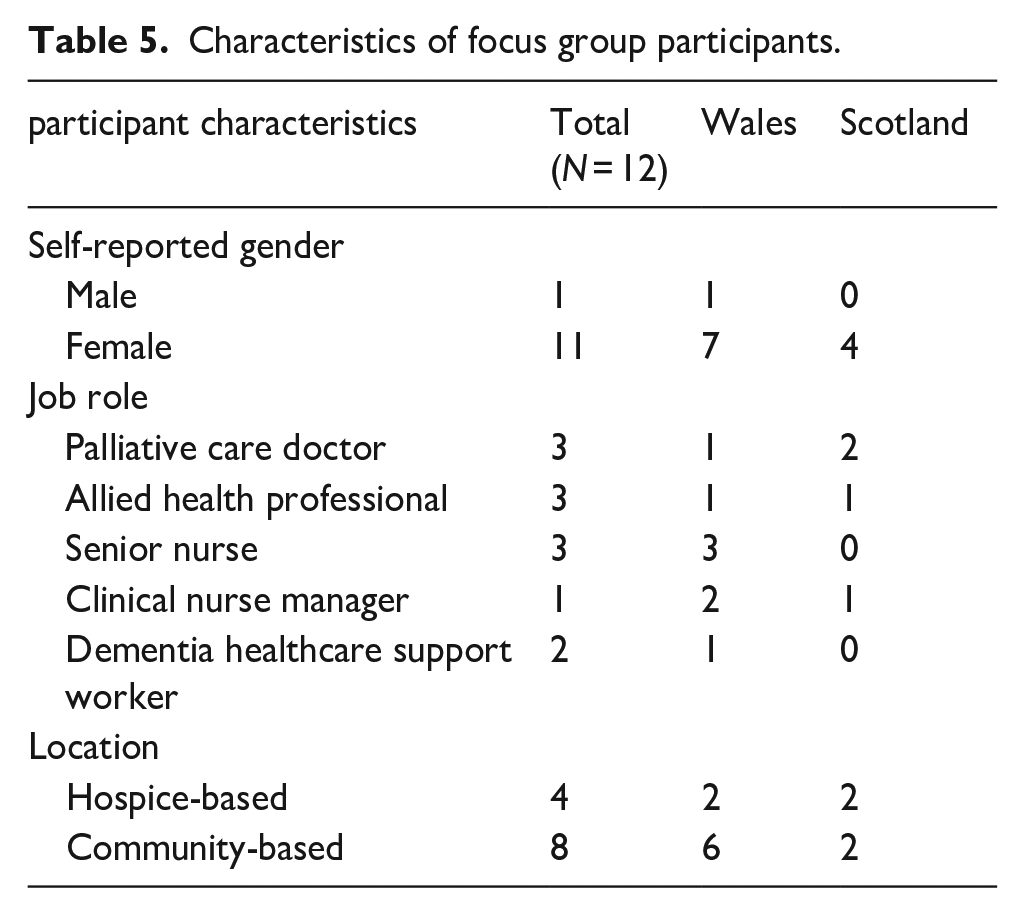
Twelve clinical palliative care staff from Scotland (n = 8) and Wales (n = 4) were recruited in total (Table 5).
Characteristics of focus group participants.
Four overarching themes were identified (Table 6). These themes describe participants views regarding how gender of either the person living with a serious life-limiting illness, or of the friend of family member who is providing care for them. They also explore how gender is one of many factors that may influence experiences for both patients and family members/friends and the impact of inequities in access to palliative care which shape the experiences and views of staff with regards to supporting a diverse population in terms of gender identity. Participants described observations of cisgendered people, unless otherwise stated.
Themes identified in qualitative analysis.

Influence of sex and gender on patterns of referral for patients with palliative care needs
Varying views were expressed regarding patterns of referral for males and females to palliative care services. Some participants felt males tended to receive higher levels of support in the community (mainly from females, although not necessarily spouses or current partners) which enabled them to stay at home for longer and therefore be referred later than females.
The male patients. . . tend to be further down the palliative route because generally speaking. . .their wives or partners are better at looking after them than the men are at looking after women, they [women] manage for longer.—Allied health professional
In contrast, others felt males tended to be referred earlier than females, as females would be more proactive in seeking and more open to receiving help from services than males.
I feel a male partner or a husband is referred to our services earlier. . .compared to a female. And a wife is a lot more accepting of allowing that care into the home.”—clinical nurse manager
Males were also thought to be more likely to be socially isolated than females, necessitating earlier support from services.
You get your men who live alone and don’t have much support, so we get an early referral for them because. . . they live alone and . . . don’t have family around. –Palliative care doctor
Conversely, others felt that isolation may lead to later access to support for males who historically have coped alone.
Men on their own. . . a lot more men come in far beyond when they could have been supported, . . . because they have just struggled on and struggled on. They’ve not allowed district nurses in, they’ve not been washing, they’ve not been shaving, not been able to get to the toilet. . . and they could have been supported a long time previous to that but refused. And you don’t often find that with women. – Clinical nurse specialist
Influence of gender on informal carers of people with palliative care needs
From participants’ observations, females were thought to be more likely to, and were more often expected to take on a caring role, than males.
In the main it’s always . . .the daughters. It’s a bit of a joke when you’re sat there with the daughter. “I’ve got three brothers, they all live next door. I live ten miles away.” The brothers don’t engage in the caring role and certainly not in the practical dealings of personal care. . . It’s always the girls.—Senior nurse
This is seen to be related to traditional gender norms, whereby females were considered caregivers. Similarly, in line with traditional views, males were thought to be less likely to take time off work to support a family member than females, as they were considered the “breadwinners.” Males were expected to take responsibility for the financial security of the family unit, while females were expected to take on the emotional and practical work of caring.
There is an expectation that men will just keep going to work, whereas. . . women. . . are more readily willing to take time off or seek help with that.—Palliative care doctor
Acceptance of support from services from male and female carers
Some participants felt male people in informal careering roles were less likely to seek or accept support for themselves and/or their unwell friends and family members than females.
The male carer is less likely to raise flags and say, “Hey, I need some help with this.” Whereas females are more inclined to ask for help, to recognise they need some extra support.—Palliative care doctor
Female caregivers were seen as more accepting of help, despite feeling pressure and sense of responsibility to fulfil the caring role. For males, pride, shame, a desire to “cope” and avoidance of therapeutic interventions were thought to make them less likely to accept help.
For some [men] it’s pride. . . they think they’re going to be asked to speak about their feelings.—Allied health professional
Impact of intersectionality
Participants agreed that while gender should be considered in relation to palliative and end-of-life experiences, other factors were likely to intersect with and perhaps exert greater influence on experience. An intersection between age and gender was noted with younger people, particularly male carers, being more likely to request and access support than older males.
Men . . . are more likely to seek help if they have young children and it’s their partner that’s end-of-life. – Clinical nurse manager
Furthermore, other factors linked to ethnicity, class, geography, financial security, culture, personality and sexuality were thought to be more influential in experience towards the end of life than gender. All participants recognised the holistic nature of palliative care and expressed a desire to provide care that aligned with the needs of individuals and those close to them.
You have to understand the patient in front of you, to try and work out what’s going to be most acceptable and useful for them. . .. I’m not sure gender is the main driver in that. It’s a lot more to do with past experiences and beliefs than . . .what sex they were born.—Palliative care doctor
Inequities in access to specialist palliative care relating to ethnicity were highlighted as a particular concern.
I think the inequality in accessing specialist palliative care is . . . far greater on ethnicity than it is on gender.. . . lots of patients from minority ethnic groups are offered less specialist services and have reduced access to services.—Palliative care doctor
Limited diversity in people accessing palliative care
Participants noted a lack of diversity among the patients and families they support, describing the vast majority of people they see as white, heterosexual and cisgendered. Relating to gender identity, some participants described feeling worried about inadvertently causing offence through incorrect use of language or limited understanding of the individual and what was important to them. This was especially true when supporting transgender people, and around the use of pronouns.
We had one patient, who prefer[red] “them/they” pronouns . . . it didn’t really affect care in any way, shape or form. . .. It was just the difficulty with the language at times.—Allied health professional
Linked to this, and despite a willingness to do so, some participants described hesitancy around collecting personal demographic data from patients, such as gender identity, ethnicity, sexuality and marital status, feeling that these were particularly sensitive topics to discuss.
Its about the disclosure. . .and not forcing any disclosure. It’s difficult in palliative care because we ask far more personal questions than other medical services. It helps us understand how someone wants to be cared for. . . But I can see that could feel incredibly threatening, if keeping that private has been the way you’ve protected yourself. . ..—Palliative care doctor
Participants suggested additional support for patient-facing staff around how to sensitively collect personal data would be beneficial. This could include discussion of how conversations around pronouns and gender identity could be conducted, as well as guidance around collecting other types of personal information, such as marital status, sexuality or religion.
Discussion
The first aim of this study was to explore sex and gender differences in referrals to palliative care services, time from referral to death, preferences for and actual place of death. Minimal differences were observed between people of different sexes with regards to these variables. The average time between referral and death was approximately 7 days. This short window could suggest that issues such as the timing of referrals or the capacity of services may be as, or more influential than factors such as gender.
The second aim of this study was to explore palliative care staff’s perceptions of the role of gender in the experiences of both patients and those close to them. Despite evolving expectations of gender roles, consistent with previous research 36 , the pressures and responsibility for unpaid caring were thought to fall disproportionately on females. Research from Canada reminds us that future research and service delivery must acknowledge diversity among caregivers, and consider multiple aspects of needs and exclusion. 37
Sexual orientation and gender identity are important aspects of an individual, consideration of which are essential for the person-centred care that palliative care aims to deliver. 38 Inconsistencies and missingness among data relating to sexuality, gender identity20,39,40 and limited confidence regarding the use of pronouns 41 in health settings and records have been recognised as an issue in the international literature and were also evident in this study.
Avoidance of asking about gender identity or sexual orientation could be related to a fear of causing offence, lack of experience or knowledge on the part of the provider, difficulties documenting identities of pronouns in existing data systems20,41 or failure to perceive its relevance. 38 Addressing biases, whether these are individual, social or systematic and increasing knowledge about sexual and gender minority communities have been suggested as routes to increase the confidence and competency of professionals providing palliative care to people from sexual or gender minorities.20,42
Whilst gender was felt to influence experiences towards the end of life, the influence of factors other than gender was recognised, and inequity in palliative care is well documented.18,43 Intersectionality acknowledges that multiple variables shape experiences. 44 In this study, participants highlighted an intersection between age and gender. While a recent systematic review examined age and gender-based social inequities in palliative care for patients with cancer, 45 few studies have looked at the intersection between age and gender in relation to palliative care. 28
Strengths and limitations
In this study, routinely collected data from a UK specialist palliative care provider were analysed to explore differences in outcomes for people of different sexes. During the project, the organisation in which the data were collected was undergoing a transformation in their digital systems, which may have impacted on the completeness of the data reviewed. The dates within the service evaluation included the COVID-19 pandemic (January 2019 and January 2022), which may also have influenced findings.
Missing data is a challenge across healthcare services, and palliative care is no exception.46,47 Robust data are key to informing service development and delivery, monitoring the reach of services and crucially, delivering care aligned with the needs, values and preferences of individuals and those close to them. 46 There is likely to be variation in whether the categorisations in the data were determined by staff, patients or those close to them across the data collected. The levels of missing data observed in this study around gender identity may reflect discomfort around asking this question.
Within the focus groups, there was often no explicit acknowledgement that cisgendered people were being referred to, but this was the assumption made. Therefore, within the results section, the terms “male” and “female” have been used when describing themes, while quotes reference “men” and “women.” This suggests that the heteronormative and cisnormative views described in relation to healthcare access elsewhere 48 could persist towards the end of life. In the United Kingdom, the vast majority (91%) of the clinical workforce in hospices is estimated to be female. 49 This over-representation of females is reflected among focus group participants. While a range of professional backgrounds were represented, we acknowledge that the limited sample size and positionality of both participants and researchers may have influenced findings.
Implications for future research and practice
This multiple methods study aligns with calls for research and practice to normalise the inclusion of all gender identities and gender-neutral language, 6 to support palliative care to deliver the person-centred care that is at its core. In addition to increasing the representation of trans of gender diverse people within research, the adoption of an intersectional lens could facilitate consideration of the complex interplay between the different elements of a person.
Specific recommendations for palliative care providers regarding how best to approach inclusive discussions about identities and relationships have been provided in the literature. From the United Kingdom, Braybrook et al. offer 10 recommendations which cover verbal and non-verbal communication, the creation of safe environments and suggestions for visible and consistent LGBT+ inclusiveness in care systems. 9 Recommendations from Canada centre on standardising the collection of sexual orientation and gender identity data and addressing biases (on individual, systemic and societal levels) through listening to sexual and gender minority patients and caregivers’ testimonials regarding specific needs, and the impact that meeting these needs can have on experiences towards the end of life. 20
Conclusion
Minimal quantitative evidence of sex differences in reasons for referrals, timing of referrals or preferred and actual place of death were observed, yet conclusions were challenged by the lack of data relating to gender identity. Sensitive and appropriate collection of patient data is needed to create and sustain inclusive and equitable services to improve palliative and end-of-life care for all. Perceived differences in experience of accessing palliative and end-of-life care and of being a caregiver were reported, highlighting the importance of person-centred, gender-sensitive palliative and end-of-life care.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251344310 – Supplemental material for Sex and gender in palliative and end-of-life care: A service evaluation and qualitative analysis
Supplemental material, sj-docx-1-pcr-10.1177_26323524251344310 for Sex and gender in palliative and end-of-life care: A service evaluation and qualitative analysis by Briony F Hudson, Bethan Edwards, Ellie Wagstaff and Nicola White in Palliative Care and Social Practice
Footnotes
Appendix 1
Acknowledgements
Thank you to our project and steering committee members and all participants who gave up their time to support the project.
Ethical considerations
Ethical approval for the qualitative study was obtained from the UCL research ethics committee (8675/004) on 21 September 2022. Research governance and data protection approvals were sought for the service evaluation.
Consent to participate
Electronic informed consent was obtained from all focus group participants.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a small grant from Marie Curie MCSGS-21-606. The funding for the Open Access publication of this article (CC BY-NC 4.0) was funded by Marie Curie as part of this grant.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Anonymised transcripts from the focus groups are available on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.