
Abstract
Objective
The purpose of this study was to conduct a clinic-radiographic quantitative evaluation of three interpositional materials, Temporalis myofascial flap (TMFF), Buccal fat pad (BFP) and Abdominal dermal fat graft (ADFG) in patients undergoing TMJ ankylosis (TMJA) release surgery.
Materials and Methods
30 joints in 18 patients of TMJA were randomly assigned to three different interpositional material groups for clinical and radiological evaluation. Maximum mouth opening (MMO) and volumetric assessment of the graft using CT scan were recorded and followed up for one year.
Results
No statistically significant difference was noted in MMO between the three interpositional materials after 1 year (p >.05). However, statistically significant difference was noted in the volume of the graft between the three. Average graft volume at 1week in TMFF was 368.15 ± 39.57mm3 and at 1 year was 250.61 ± 37.72mm3; in BFP, at 1 week was 287.69 ± 20.37 mm3 and at 1 year was 267.11 ± 19.24 mm3; in ADFG, at 1 week was 284.18 ± 30.28 mm3and at 1 year was 280.7 ± 14.28mm3. ADFG showed the least volume reduction and TMFF showed the most. Minimal complications in terms of transient facial palsy and local infection were noted and treated conservatively.
Conclusion
At present the only study in the literature radiologically quantitatively assessing and comparing three interpositional grafts, ADFG is highly satisfactory; thereby may be hailed as arguably the best interpositional material in TMJA surgery.
Keywords
Introduction
The management of Temporomandibular Joint Ankylosis (TMJA) aims to restore mouth opening, prevent re-ankylosis and improve aesthetics and quality of life. 1 A space of 10-15 mm should be created to permit mouth opening along with placement of a soft tissue interpositional material to help to prevent reankylosis. 2 The interpositional tissue inhibits osteoblastic growth between the abraded bone surface and should completely fill the gap created by resection of ankylotic mass thereby preventing hematoma formation and its subsequent organization and calcification leading to reankylosis. 3
No interpositional material mentioned in the literature—alloplasts, articular disc, temporalis muscle/fascia, fascia lata, skin graft, conchal cartilage, and fat—has been considered ideal. Muscle may fibrose, cartilage may calcify, fascia is not bulky enough and alloplastic implants may cause foreign body reactions. 4
Temporalis myofascial flap (TMFF) and buccal fat pad (BFP) have been employed as interpositional materials in TMJA.5–6 As they are both pedicled flaps, it has been traditionally thought that the chances of their volumetric shrinkage and therefore reankylosis are less. Abdominal dermal fat graft (ADFG) though non pedicled, can be harvested in larger volumes. 7
However, very few studies have quantified the volume of interpositional materials.8, 9 Also, to the best of our knowledge, there is no study comparing the degree of resorption of TMFF, BFP and ADFG, and that retained. Therefore, in this study, the authors have quantitatively evaluated these three interpositional materials in terms of mouth opening and Volumetric assessment.
Materials and Methods
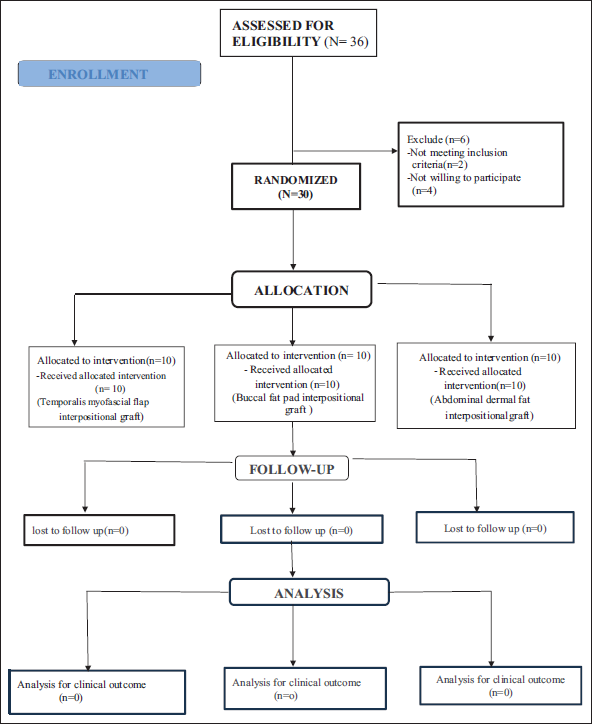
The single centre prospective interventional study comprised of 30 joints in 18 patients (5-39 years) of bony TMJA in a three-year span. A 1-1.5cm gap was created using a piezoelectrical unit achieving 30-35mm mouth opening using a preauricular approach.10, 11 This was followed by Interpositional Arthroplasty and Ramus condyle unit (RCU) reconstruction with coronoid graft which was harvested from same surgical site. Fibrous, fibro-osseous, reankylosis cases and those with intact articular discs were excluded. Among the 36 eligible joints (22 patients), 2 were not meeting the inclusion criteria and 4 refused to consent to the study because of concerns taking long-term follow-up and socio-economic reason (Figure 1). Patients were randomly selected irrespective of age and sex for participation and divided into Group A (TMFF), Group B (BFP), and Group C (ADFG) according to the computed assisted random sequence generation. Ethical clearance from the Institute and informed consent from patients were obtained. Before enrolment, the aim and objectives, implications and possible complications of the clinical trial were explained to all the patients and informed consent was obtained. Patient did not receive any financial compensation for participating in study.
Consort Diagram.
Interpositional Materials
Temporalis Myofascial Flap (Figure 2): A 5 × 2cm inferiorly pedicled, finger-shaped, posteriorly placed, composite TMFF was harvested and sutured to soft tissue into dead (gap arthroplasty) space. 1
Harvesting TMFF.
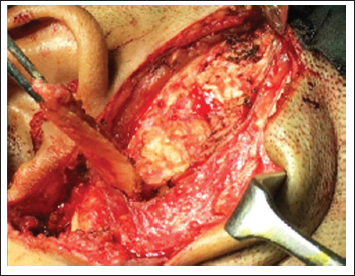
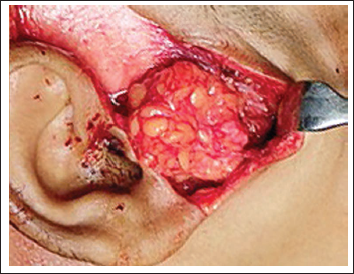
Buccal Fat Pad (Figure 3): Dissection was carried out subperiosteally in the region of the coronoidectomy along the anterior border of the ramus. Then a stab incision was placed through the periosteum followed by blunt dissection to reveal the BFP. It was then teased into the defect, while milking the maxillary buccal sulcus near the second molar region and sutured to soft tissue around gap arthroplasty space/dead space. 2
Harvesting and Interpositiong BFP in Gap Arthroplasty.

Abdominal dermal fat graft (Figure 4): A 4 × 1.5cm elliptical incision was placed 3-5cm below the umbilicus exposing the underlying fat. Blunt dissection through the fat was carried out to reach the abdominal fascia and the graft was harvested, following which its epidermis was excised. The graft was then folded onto itself with the dermis apposed and the fat was trimmed to fill the joint cavity. 8
Interposition of ADFG in Gap Arthroplasty.
Evaluation of Parameters
Clinical evaluation was done at 1 week, 6 months and 12 months while CT scan was taken at 1 week and 1 year.
Clinical evaluation: Maximal mouth opening (MMO) and complications were evaluated—facial nerve weakness, infection, cosmetic deformity (Conspicuousness of scar, temporal and cheek hollowing). Patients’ overall treatment satisfaction were evaluated using Patients’ global impression of change (PGIC) scale 1 to 10 was also recorded.
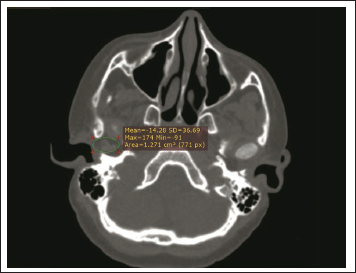
Radiographic evaluation: Volumetric assessment of the interpositional materials, based on DICOM data of axial CT scans was performed by two radiologists and one maxillofacial surgeon and averaged. All scans were performed on the same machine with the same scanning protocols in coronal, axial and sagittal planes. Volume was defined for each axial slice by the thickness of a selected area (Figure 5) measured by RadiAnt DICOM data viewer (64-bit). Johansson’s formula was used to measure the total volume of graft: Vgraft = ∑(selected areas × thickness of each section). 12
CT Scan Shows Measurement of Volume on Axial Section.
Results
This study consisted of 30 joints (12 bilateral, 6 unilateral) in 18 patients (10 females and 8 males) of the age group of 5-39 years (average 18.22 years). There were 6 patients (9 joints) below 12 years of age (Table 1). Data analysis was done with SPSS vs 25using the Paired t test and ANOVA test. P <.05 was considered statistically significant, keeping
Demographic Data, Preoperative and Postoperative Evaluation of MMO and Interpositional Graft Volume.
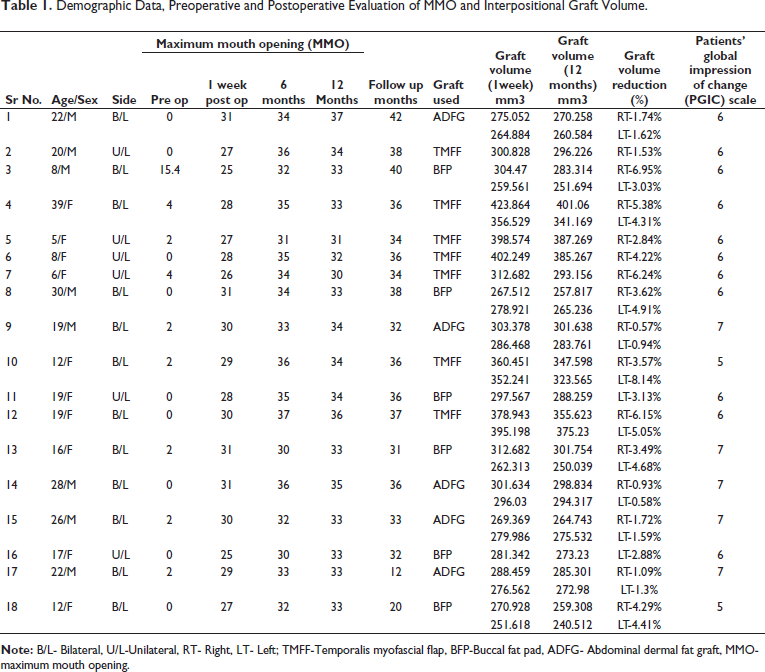
In the TMFF group, preoperative MMO was 0-4 mm (mean 1.7). It increased postoperatively to 26-30 mm (mean 27.85), 31-37 mm (mean 34.8) at 6 months and 30-35 mm (mean 32.16) at 12 months. Average graft volume at 1week was 368.15 ± 39.57mm3 and at 1 year was 250.61 ± 37.72mm3. Average volume reduction was 4.74%.
In BFP group, preoperative MMO was 0-15.4 mm (mean 2.9). It increased postoperatively to 25-31 mm (mean 27.83), 30-35 mm (mean 32.16) at 6 months and 33-34 mm (mean 33.20) at 12 months. Average graft volume at 1 week was 287.69 ± 20.37 mm3 and at 1 year was 267.11 ± 19.24 mm3. Average volume reduction was 4.14%.
In ADFG group, preoperative MMO was 0-2 mm (mean 1.2). It increased postoperatively to 29-31 mm (mean 30.2), 32-36 mm (mean 33.6) at 6 months and 33-37 mm (mean 34.4) at 12 months. Average graft volume at 1 week was 284.18 ± 30.28 mm3 and at 1 year was 280.7 ± 14.28mm3. Average volume reduction was 1.21%.
No statistically significant difference was noted in MMO between the three groups after 1 year (p >.05). However, statistically significant difference was noted in graft volume reduction, ADFG showing the least and TMFF the most.
Transient paresis of facial nerve was reported in 6 patients in TMFF, 4 in BFP and 4 in ADFG which all resolved within 3 weeks. Infection was reported at TMJ area in one ADFG group and stitch abscess was reported in one TMFF group; both were successfully treated conservatively. There were no reported cases of permanent facial nerve damage, re-ankylosis, seroma, infection, peritoneal perforation and cheek/temporal hollowing. Mean patient PGIC score was 5.8 in TMFF, 6 in BFP and 6.8 in ADFG; this difference was not statistically significant.
Discussion
This study, both clinically and radiographically, evaluated the efficiency of TMFF, BFP and ADFG in TMJA after interpositional arthroplasty with RCU reconstruction.
Balaji 13 conducted a study with costochondral graft and TMFF in TMJA with a 6 year follow up. The mean MMO in patients below 12 years was 31.8 mm and above it, was 35.5 mm. The mean MMO of 6 children in our study was 32.16 mm and in 12 adults was 34 mm, the overall mean MMO being 33.18 mm.
In a study by Vishal Bansal 9 , BFP was measured preoperatively, though not intra-operatively, using Ultrasonography. Chaudhary measured the intra operative volume of ADFG using a syringe 5 . However, in this study, neither the preoperative nor the intra operative volume assessment of any the interposition materials was performed. The reason for the same was that being pedicled flaps, TMFF and BFP are not amenable to exact intraoperative volume assessment. Therefore, maintaining uniformity, all three were assessed radiographically 1 week postoperatively and then compared at 1 year.
Temporalis Myofascial Flap
TMFF, with or without overlying fascia has been considered an ideal interpositional material due to its proximity to the surgical site and its vascularity.11, 14 However, its potential drawbacks include sloughing of fascia and its tendency for atrophy and fibrosis, aggravating trismus.
Vikas Aneja 15 evaluated TMFF in 10 patients over 3.3 years and found MMO increase from 6.8 to 34.5mm.Su-Gwan 16 studied 7 patients for 20.1 months and reported MMO increase from 15 to 36.1mm. Bulgannawar 6 evaluated temporalis fascia in 8 patients over 4.3 years with MMO increase from 2.75 to 36.5mm. In this study, mean MMO increased from 1.7 to 32.85mm at 1 year.
The mean volume reduction at 1 year in our study was 4.74%. To the best of our knowledge, no other study has radiographically measured the volume of TMMF as interpositional material in the longer term.
Complication of pain during jaw movement, trismus, alopecia, loss of interpositional material and temporal hollowing have been reported with TMFF. 14 Temporal hollowing was not observed in this study as the TMFF was harvested from the posterior part of the temporalis rather than the traditional anterior part.
Buccal Fat Pad
BFP is encapsulated, easily accessible, has a tendency to epithelize and can be harvested as a pedicled flap without the need for an additional donor site. However, the smaller size and volume of fat lobules may make them vulnerable to fragmentation during harvesting and functional loading of the TMJ.
Singh 2 used BFP in 10 patients of TMJA and after 2 years, found MMO increase from 2.8 to 35.1 mm. Adebayo 17 utilised BFP as, a free graft and a pedicled flap in 7 joints and found MMO increase from 3.5 to 36.5mm. In our study, the mean MMO after BFP increased from 2.9 to 33.2 mm at 1 year.
Gaba et al 3 studied BFP in 18 patients clinically and radiographically. On MRI he could detect BFP in 65% joints at 1 year. Roychoudhury et al 5 compared BFP and ADFG in 36 patients. After BFP, MRI showed 67.5% volumetric shrinkage at 1 year. The volume retained was 1.4cm3. In this study, the mean volume reduction was only 4.14%.
The role of vascularity alone in graft survival is questionable—BFP, though pedicled has shown more shrinkage as compared to ABDG in both, this study and that of Roychoudhury. 5 Complications like infection, bleeding and reankylosis were not encountered like Gaba et al. 3
Abdominal Dermal Fat Graft
ADFG may be considered relatively resistant to resorption as it has a large volume and size of fat lobules. Also, the greater number of stem cells in ADFG than in BFP account for a greater potential for lipogenesis and prevention of adipolysis.7, 8 The dermis helps in blood perfusion and vasoinduction for the underlying fat 18 and acts as a graft carrier, making handling easy 19 and preventing fat fragmentation during transfer. However, the dermis has a propensity to form epidermoid cysts if the epidermal layer is not completely removed at the time of harvesting.
Dimitroulis 19 studied non-vascularised fat grafts in 21 rabbits, which did not survive after transplantation, but promoted neoadipogenesis. The dermis survived while the fat necrosed and was replaced by new fat. Saunders et al 20 studied 75 mice and showed that the new fat was normal in appearance, but lesser in volume. Qi et al 21 reported early fat ischemia in 48 rats but in 6 months, the fat grafts became volumetrically normal. Roychaudhary observed that volume rather than vascularity of fat is a crucial factor in its availability in the interposed site to achieve a better clinical outcome. All fat, irrespective of vascularity and the site of harvest, undergo ischemia and resorption during early stages of transplantation. The resorption rate is 20-70%, subsequently, it is suggested that a 30% excess may be harvested. This, however, is not possible for pedicled buccal fat pad. 5
Dimitroulis 7 evaluated ADFG in 11 patients of TMJA and observed MMO increase from 15.6 to 35.7 mm after 41.5 months. In this study, the mean MMO increased from 1.2 to 34.4 mm at 1 year.
Dimitroulis 8 evaluated 15 patients of ADFG on MRI after 2 years of discectomy and reported the average volume of the fat graft in and around each joint to be 3.10 ± 1.46 cm3. In term of statistical significance, the fat did not resorb. Roychoudhury 5 further found 41.9% volumetric shrinkage of ADFG on MRI after 1 year and reported the mean volume retained was 6.3cm3. In this study, the mean volume retained was 2.8 cm3 and the volumetric reduction was1.21%.
Possible complication of ADFG include hematoma, seroma and inadvertent peritoneal perforation have been reported in the literature. Dimitroulis 7 observed 9.1% reankylosis in his study. No reankylosis was seen by Roychoudhary 5 or in the present study.
Imaging/Radiographic Evaluation
It is widely accepted that soft tissues are always better evaluated on MRI than CT scan. Following this norm, MRI was considered in our study for graft volume evaluation as performed by Dimitroulis and Roychoudhury. Starcukova 22 showed that MRI without artefacts is possible only if nearby implants are made up of material having low magnetic susceptibility and low electrical conductivity like pure titanium. However, most commercially available titanium implants do not meet this criterion of purity. On the other hand, Kocasarac 23 has showed that titanium and titanium alloy implants generate fewer artefacts on CT scan.
Gaba 3 performed MRI on 18 cases of TMJA at 6 and 12 months to assess the fate of BFP. At 6 months, artifacts hampered the visualization of BFP in 60% of cases. At 12 months, BFP was visible only in 65% of cases.
Therefore, in this study, radiographic evaluation of the volume of the graft was performed initially using MRI; but the titanium implants used for Ramus condyle unit reconstruction led to the appearance of large artefacts on MRI, due to which exact graft evaluation was not possible. The importance of RCU reconstruction in maintaining ramus height and preventing secondary occlusal problems was emphasised in a previous studies.24, 25 Therefore, CT scan was therefore considered for graft volume evaluation for that patient as well as for all future patients. This showed fewer artefacts and gave a better delineation of the graft.
Conclusion
To the best of our knowledge, this is possibly the only study in literature regarding volumetric assessment of TMFF, BFP and ADFG as interpositional materials in TMJ Ankylosis, utilising a CT scan. At one year follow up, there was no statistically significant difference between the three interpositional materials for maximum mouth opening. Although the volume of the pedicled TMFF in the immediate postoperative period was the greatest and the non-vascularised ADFG the least, the former showed the most resorption and the latter, the least. It is suggested that neither the vascularity nor the initial harvested volume of the interpositional material had any effect on final outcome in terms of residual volume of the graft. Graft shrinkage in the healing period may be due to inflammation, fat fragmentation during surgery and joint loading and failure of the graft to revascularize. The final success rate of interpositional grafts material in term of preservation of volume was ADFG>BFP>TMFF.
A limitation of our study is the relatively short duration of follow up. Since we believe that RCU reconstruction is essential. CT scan instead of MRI had to be used for volumetric assessment of graft using CT scan it is difficult to assess what the fat has transmitted but change in volume of fat can be adequately assessed. Thus, it may be concluded that based this study, the interpositional material definitely persisted and did not resorb; however, whether they continue to remain muscle and fat or transformed into other tissue may be subject to scrutiny.
Ultimately the goal of treatment of ankylosis is to prevent new heterotropic bone formation and this has been shown to occur at one year in all three groups, although with better volume preservation using abdominal dermal fat graft.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and the Declaration of Helsinki of 1975 that was revised in 2000. (IEC GDCH/OS.3/2018).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient before their inclusion in the study with the approval from ethical committee. The procedure was explained to them regarding the nature and benefit of the study.