
Abstract
Methods:
A 10-year retrospective analysis of eight patients with temporomandibular joint (TMJ) ankylosis. The age, gender distribution, etiology, affected side (unilateral or bilateral), mouth opening (MO), and occlusion were evaluated pre-operatively and after gap arthroplasty (GA) with follow-up two years.
Results:
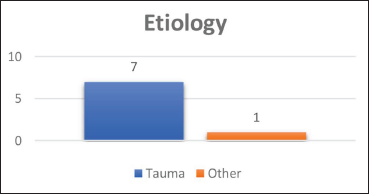
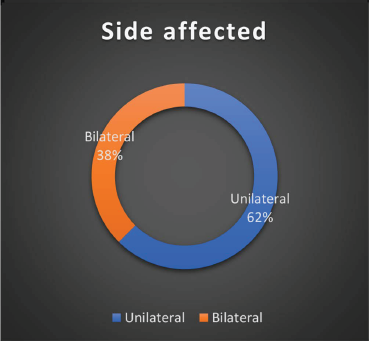
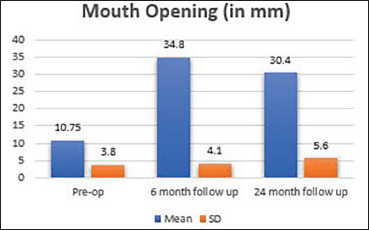
In this study, there were eight participants, with an average age of 24.75 ± 3.8 years, gender distribution was 62% men and 38% females with seven individuals having etiology of trauma and 1 pathology. TMJ ankylosis was found to be bilateral in 38% of patients and unilateral in 62%. Pre-op and two-year follow-up MO showed a mean of 10.75 ± 3.8 mm and 30.4 ± 5.6 mm, respectively. Re-ankylosis was not reported in any cases.
Conclusion:
The most effective care for TMJ ankylosis begins with a correct and timely diagnosis, followed by the development of a proper/comprehensive treatment plan thus improving the patient’s quality of life. We conclude that all of our GA patients had appropriate MO at follow-up of 24 months. Long-term functional outcomes of GA are satisfactory as it justifies adequate MO with minimal complications. After GA jaw physiotherapy is also critical for long-term success.
Introduction
Temporomandibular ankylosis characterizes, bony or fibrous adherence of joint followed with reduced mouth opening (MO). In circumstances where the patient is still growing, this may also impair the symmetry of the face skeleton. 1
It has an impact on the patient’s psychological growth and jeopardizes their life due to the incapability to open mouth. 2
A number of conditions, including arthritis, infections, trauma, temporomandibular joint (TMJ) surgery, tumors, hereditary flaws, cryptogenic and induced causes, leads to TMJ ankylosis. Infection is the primary cause of TMJ ankylosis, however, trauma ranks second. 1
These people have restricted mandibular mobility, which can result in malocclusion and asymmetry of face. As a result, the mandible’s vertical, sagittal, and transverse orientations may alter on the afflicted side, with altered craniofacial growth and development. 3
A detailed pre-operative examination and severity of the deformity is crucial for effectively treating ankylosis. 4
TMJ ankylosis treatment options are condylectomy, gap arthroplasty (GA), interpositional (IGA), coronoidectomy, and complete restoration or replacement. 2
GA is a commonly used procedure, technically easier and less time-consuming compared to IGA. Regarding the relative merits of GA and IGA, literature has two schools of thought. According to some authors, both GA and IGA could significantly increase MO, but one could totally avoid re-ankylosis whereas according to some authors, GA alone can produce acceptable results. An adequate gap between two bony segments and aggressive jaw physiotherapy are very important factors in the management of TMJ ankylosis and avoid re-ankylosis. 5
Kaban’s protocol is very well known for managing ankylosis. 6
Aesthetics becomes a secondary goal after achieving adequate MO and providing the patient with proper nutritional care through a balanced diet and lifestyle. 7
Materials and Method
Retrospective research was conducted. After getting consent (SVIEC/ON/DENT/RP/NOV/22/17) from the Ethics Committee, data from the medical records of patients treated with arthroplasty at our center between the months of January 2011 and December 2021 were retrieved.
The parameters studied were:
Age and gender distribution Etiology Affected side (unilateral or bilateral) Mouth opening (MO) Occlusion
Through the use of panoramic radiographs and 3-D computed tomograms, radiographic examinations were used to identify anatomical borders and type of ankylosis. Patients underwent the GA procedure, which involved exposing the ankylosed mass, with a gap of at least 1.5 cm, followed by the insertion of a drain and closure. After surgery, the patient received prophylactic antibiotics and followed by aggressive jaw physiotherapy from first post-operative day itself.
Methodology
The medical records of TMJ ankylosis patients treated with GA at our Hospital between January 2011 and December 2021 provided the data for this study.
Compilation of data, regarding ankylosis of the affected side, etiology, age, gender, pre- and post-operative MO was done. The clinical history, symptoms, correctly interpreted radiographs all contributed to the diagnosis.
The data obtained were statistically analyzed and interpreted.
Results
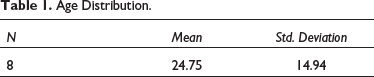
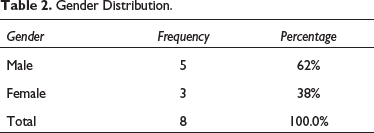
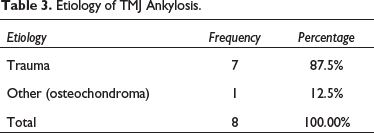
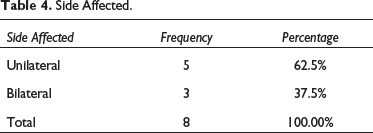
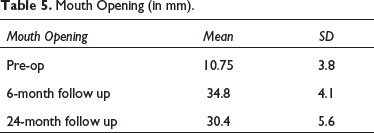
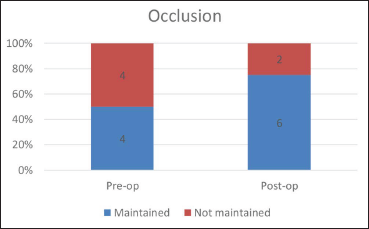
During 10 years of a retrospective study from January 2011 to December 2021, eight patients with temporo-mandibular ankylosis were given treatment with a mean age of 24.75 ± 3.8 years (Figure 1, Table 1) and with a gender distribution of 62% males and 38% females (38%) (Figure 2, Table 2). In the population studied, trauma was found to be the commonest etiology of the ankylosis counting 87.5% of the cases, followed by pathology (osteochondroma) representing 12.5% of the cases (Figure 3, Table 3). The study showed that side affected, from a total samples of 8, 62.5% had unilateral and 37.5% had bilateral involvement TMJ ankylosis (Table 4, Figure 4). In all patient’s MO was measured pre-operatively, at six-month and at two-year follow-up. It showed a mean of 10.75 ± 3.8 mm, 34.8 ± 4.1 mm, and 30.4 ± 5.6 mm, respectively (Table 5, Figure 5). Status of preoperative occlusion was ideal in 50% of case and was not in other 50%. Post-operative occlusion was improved in 25% and maintained in 75% of total cases (Table 6, Figure 6). During the period of postoperative follow-up, temporary facial paresis occurred which lasted for three to five weeks, which was estimated to happen due to excessive flap retraction. No permanent facial nerve damage was reported in any case. Infection and a foreign body reaction can contribute to re-ankylosis.
Age Distribution.
Gender Distribution.
Etiology of TMJ Ankylosis.
Side Affected.
Mouth Opening (in mm).
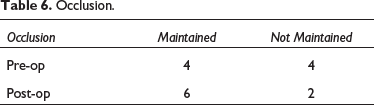
Occlusion.
Age Distribution.
Gender Distribution.
Etiology of TMJ Ankylosis.
Side Affected.
Mouth opening.
Occlusion.
Discussion
Ankylosis is a severely disabling disorder that affects speech and eating patterns as well as the patient’s facial appearance, worsening stress, inhibiting appropriate hygiene, having a negative impact on the oral health of patient’s. The literature lists a variety of ankylosis therapy options. Discussing about the best course of treatment in 1851 Esmarch, was given credence for undertaking the first osteotomy for ankylosis. Abbe (1880) and Risdon (1934), introduced of GA and interpositional arthroplasty, as efficient treating options. To prevent any further recurrence, restoring MO to at least 35 mm is the ultimate objective. 2
The oldest treatment, GA involves total removal of the ankylosed mass without interpositional material. Its simplicity and low operation time are advantages. However, when the condition is unilateral, the mandible grows normally on the unaffected side while the affected side experiences reduced growth. Despite the unaffected side developing normally, this may restrict the ipsilateral extension of the maxilla in growing individuals. In some instances, the maxilla on the affected side may grow normally, whereas it may grow excessively on the unaffected side due to the normal side’s unrestricted growth. A maxillary cant is the outcome of both of these events. In bilateral cases, the patient has an obtuse cervicomental angle, a mandible that is prominently retruded, and no chin. Slightly shorter posterior maxillary height results in steep occlusal planes. It is often referred to as a bird face deformity or Andy gump appearance because of the convex facial profile. 3
In the present study, we used the procedure of gap arthroplasty paired with active aggressive jaw physiotherapy as a therapeutic modality and discovered that it has a high success rate.
In the study by Xia et al. of 71 instances, out of the 71 patients, 42 (59%) were men and 29 (41%) were women. 8 In the current study, there were eight total participants, with a mean patient age of 24.75 (interquartile range: 16–55) years. Five of the participants were men (62%) and three were women (38%).
According to a study conducted by Roychoudhury et al., 76% had unilateral involvement and 24% had bilateral involvement. 2 In the present study, patients with unilateral involvement of TMJ ankylosis were 62% and 38% had bilateral involvement.
Trauma is the most frequently reported etiology of the disease in our study (87.5%), virtually identical to the 91.7% reported in the study by Anchlia et al. 9
Ankylosis occurs in the first and second decades of life with trauma (13%–100%), local or systemic infection (0%–53%), and surgery are all common causes. In addition to these, other etiological variables include radiation, systemic lupus erythematosus, myositis ossificans, osteochondroma, ankylosing spondylitis (Bechterew disease), and psoriatic arthritis. According to the study conducted by do Egito Vasconcelos et al., eight patients were submitted to TMJ surgery in which etiology included trauma at 75%, and others at 25%. 10 In the present study, 87.5% of patients had etiology of trauma and 12.5% with pathology (osteochondroma). To summarize, ankylosis has trauma as its principal etiology, which happens at an early adolescence age, more in men, unilaterally.
GA includes condylectomy which is a simple procedure with a fast recovery period. There are a number of disadvantages, such as the development of a pseudo-articulation, short ramus, the failure to eradicate all bone diseases, a raised risk of re-ankylosis, and the absence of functional joint restoration. There occurs anterior open bite in cases of bilateral ankylosis cases. While in cases of unilateral ankylosis posterior teeth do not occlude properly or may remain in cross-bite on unaffected side with inadequate range of motion. 11
According to Rajan et al., in five instances, the average pre-op MO was 8.6 mm, while the average post-operative MO was 37.9 mm. 12 In the present study pre-op MO with a mean of 10.75 ± 3.8 mm and post-op MO of 34.1 ± 4.1, respectively.
According to knowledge in the literature, occlusion as a factor in pre-op and post-op has not been considered in many studies. In the analysis by Roychoudhury et al., 13 patients had unstable occlusions after surgery; improvement was seen at the next visit. 2 In the present study, post-operatively occlusion was maintained in six participants and unsteady in two.
Various complications can arise during gap arthroplasty procedure. When there is excessive retraction of the soft tissues intraoperatively, transient may arise, and can be managed by steroid medication. Osteotomy cut should be directed 45 inward and downward manner, cautiously taking into account glenoid fossa. Also one can gently tease out the ankylotic mass from glenoid fossa without disturbing the local anatomy. 13 Other complications can be permanent facial palsy, parotid sialocele and deafness.
In our study, no major complications were reported in any case.
Re-ankylosis can have a variety of causes, however, it is generally believed that insufficient resection and patient adherence with postoperative MO exercises or physiotherapy are the main culprits. Wound infection and a foreign material response brought on by interposition substitutes are two reasons that might cause re-ankylosis. 14
Conclusions
Suitable treatment plan was established after prompt and accurate diagnosis of TMJ ankylosis. At the 24-month follow-up, we deduced the conclusion that all patient treated with gap arthroplasty had sufficient MO. Long-term functional outcomes of GA are satisfactory as it justifies adequate MO with minimal complications. Here we believe in initiating rigorous physiotherapy on the first postoperative day itself. As far as stable occlusion and sufficient range of motion and mouth opening are achieved other disadvantages of gap arthroplasty can be overlooked. Constant follow-up of 24 months is adequate to exclude chances of re-ankylosis.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Is Gap Arthroplasty Sufficient in TMJ Ankylosis: Our Experience by Amit Mahajan, Dharang Soni, Pratesh Dholabhai, Sharvari Daithankar, Aditya Shah and Chaitya Adalja, in The Traumaxilla
Footnotes
Acknowledgement
We appreciate Dr Gulam Naviwala’s for remarks, wise suggestions, and careful reading of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical Committee approval with completion no. SVIEC/ON/DENT/RP/MARCH/23/39.