
Abstract
Oral submucous fibrosis (OSMF) is a potentially malignant condition of the oral cavity. Various surgical treatment modalities have been advocated in the management of OSMF with variable results. We are reporting a case of OSMF Group IVa where the post-fibrotomy defect was reconstructed using a platysma myocutaneous flap (PMF) in a young male patient. Postoperatively, patient was evaluated during a regular follow-up period for one year. The Preoperative interincisal opening of 2 mm gradually improved to 35 mm at the end of one year postoperatively with no postoperative complications. The facial aesthetic is not compromised as the incision is some way from the face and the scars are hidden underneath the collar. PMF can be considered a good reconstructive option for OSMF with aesthetically acceptable results, however, the technique is more demanding and must be mastered properly.
Introduction
Oral submucous fibrosis (OSMF) is a premalignant condition characterised by blanching and stiffness of the oral mucosa, which causes progressive limitation of mouth opening. Areca nut, commonly known as betel nut or supari, plays a crucial role in the aetiology of OSMF. 1
Majority of the treatment modalities focus on alleviating the burning sensation and releasing the vertical fibrotic bands, that is, fibrotomy to increase interincisal opening. Conservative treatment primarily consists of multiphase intralesional injections of placental extract, hydrocortisone, hyaluronidase and triamcinolone, along with supplements of micronutrients and vitamins. 2 Surgical technique for management of OSMF includes fibrotomy, myotomy, coronoidotomy/coronoidectomy followed by reconstruction of the surgical defect with the help of various flaps. Over time numerous reconstructive options have evolved such as Tongue flap, the Palatal Island mucoperiosteal flap, and the BFP (Buccal Fat Pad) and extraoral flaps such as the Nasolabial flap, Platysma myocutaneous flap (PMF), superficial temporal fascia flap and Radial artery forearm flap. Though numerous surgical modalities have been advised for the management of OSMF, each has their own merits and demerits. 3
PMF is a versatile flap that has been used for intraoral defect reconstruction since 1978. Depending on the prevailing vasculature, three types of platysma flaps are available: superiorly, posteriorly, and inferiorly based. Superiorly and posteriorly-based flaps are most commonly used for Orofacial reconstruction. It is thin, pliable, simple to harvest and also suitable for 3-D reconstruction of defects with minimal morbidity of the donor site with primary neck closure. 4
We are reporting a case of OSMF Group IVa (According to Khanna and Andrade 5 , 1995) where the post-fibrotomy defect was reconstructed using PMF in a young male.
Case Report
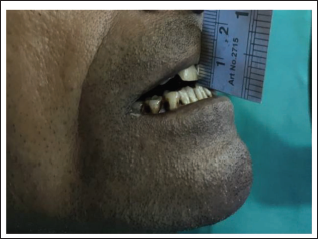
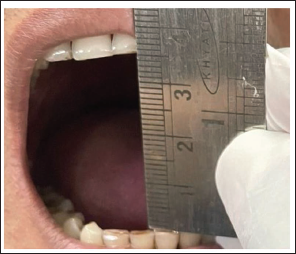
A 38-year-old male patient reported to the Department of Oral and Maxillofacial Surgery with the chief complaint of difficulty in mouth opening and burning sensation on having hot and spicy food for the past four years. Patient gave a history of tobacco consumption (Gutka chewing) of three to four packets per day for the past 10 years. On clinical examination, blanching of the buccal mucosa, soft palate and mucosa covering hard palate was seen. On palpation, vertical fibrotic bands on buccal mucosa, retromolar trigone area and perioral fibrotic bands were present with a maximum interincisal opening of 2 mm (Figure 1). Also, OPG revealed bilateral elongated coronoid process of the mandible.
Preoperative Maximum Inter Incisal Opening - 2 mm.
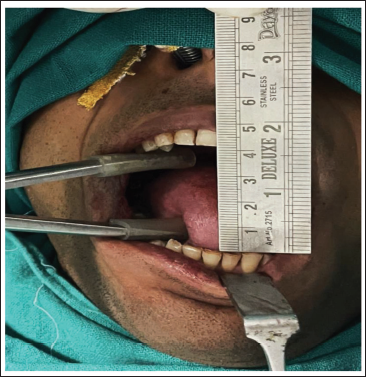
After thorough history taking and clinical examination, routine blood investigations were done. Patient was operated under general anaesthesia with nasotracheal intubation using fiberoptic bronchoscope followed by surgical part preparation and draping. 2% lignocaine with 1:80,000 adrenaline was infiltrated along the intended incision line parallel to the occlusal plane to achieve haemostasis. An incision was made extending from the anterior faucial pillar to 1.5 centimetre(cm) away from the commissure of lip, at the level of the occlusal plane avoiding injury to Stensen’s duct. The incised fibrotic bands were further disentangled manually with the use of curved haemostats. Bilateral medial pterygoid, masseter and temporalis myotomy were done using electro-cautery and an interincisal opening of 25 mm was achieved using a heister jaw opener. The coronoid process was then exposed through the same incision and bilateral coronoidotomy was done using chisel and mallet method. Now the mouth opening achieved was 42 mm (Figure 2). Prophylactic extraction of all the erupted third molars and second molars was done.
Intra-operative Maximum Inter Incisal Opening - 42 mm.
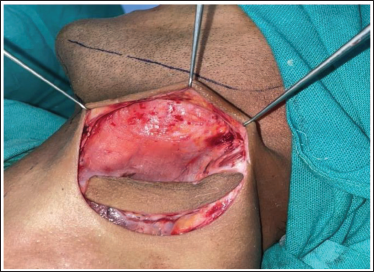
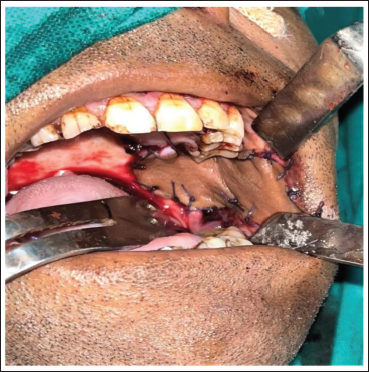
Reconstruction of the intraoral post-fibrotomy defect was done using a superiorly-based PMF. Patient was positioned with the neck hyperextended and the skin paddle was outlined on the neck, bilaterally below the inferior border of the mandible (Figure 3). First, the superior incision was made and dissection was done in a plane superficial to the platysma muscle cephalic to the inferior border of the mandible (Figure 4). A skin incision was then made at the inferior line of the skin paddle, with exposure of the platysma muscle inferiorly. Transection of the platysma muscle was done sharply at least 1 cm inferior to the edge of the skin paddle, and a subplatysmal plane of dissection was established right below the inferior border of mandible. After fully developing the plane of dissection, transection of the PMF was done vertically: anteriorly and posteriorly for full mobilisation (Figure 5). Using a soft tissue tunnel the flap was introduced into the oral defect. The harvested flap was then sutured to the intraoral defect (Figure 6). Closure of the donor site was done in layers (Figure 7) with deep layer sutured using 3-0 vicryl and superficial layer using 4-0 prolene to attain an aesthetically acceptable outcome. An intraoral pressure pack was given and an extraoral pressure dressing was applied.
Extraoral Skin Markings for Platysma Myocutaneous Flap.

Platysma Muscle with Skin Island at Lower End and the Skin Above is Being Undermined.
Mobilisation of the Harvested Flap.

Intraoral Closure of Recipient Site.
Extraoral Closure of Donor Site.

Nasogastric tube (Ryle’s tube) was secured for postoperative feeding and patient was kept under Antibiotic, Anti-inflammatory and Analgesic coverage postoperatively. The medications were administered intravenously for 3 days postoperatively and oral administration for a further five days.
Following a 10-day latent period, active physiotherapy was initiated utilising Hister’s jaw exerciser three times a day for fifteen minutes per session in order to avoid contracture and relapse. Patient was advised and motivated to maintain the physiotherapy for one year. Patient was evaluated at a regular follow-up period till one year postoperatively.
The interincisal opening was 30 mm at 1st postoperative month which gradually improved to 35 mm at the end of one year (Figure 8). No postoperative complications were recorded with complete coverage of the defect and good consolidation of the flap at the end of one year.
Postoperative Maximum Inter Incisal Opening - 35 mm at One Year Follow-up.
Discussion
Ever since Schwartz J 6 initially described OSMF in 1952, pathogenesis and management of this condition have been an issue of controversy. Chewing areca nuts, eating spicy cuisine, nutritional deficiencies, genetic predisposition, autoimmune, and collagen abnormalities are a few of the variables that have been proposed as contributing factors to the pathophysiology of this condition. Based on the observation of an Indian case-control study by Sinor PN et al., 7 it has been observed that with the increase in the duration and the frequency of the areca nut chewing the risk for the development of OSMF increases.
Futrell JW 8 was the first to reconstruct intraoral defects with a PMF in 1978. Since then, it has been extensively utilised for the reconstruction of various head and neck defects. This flap is thin, pliable, simple to harvest and facilitates three-dimensional reconstruction with low donor site morbidity.
There are three variants of the platysma flap, depending on the predominant vasculature. Transverse cervical artery supplies the inferiorly based flap, posteriorly based platysma flap gets its axial blood supply primarily from branches of an occipital artery (Collateral circulation from the superior thyroid and posterior auricular arteries may also contribute) and the submental branch of the facial artery supply the superiorly based platysma flap. External jugular and submental veins are the chief venous drainage of this flap. In the orofacial region, the superiorly based and posteriorly based flaps are commonly used. 4 The skin paddle’s dimensions range from 5 × 10 cm to 7 × 14 cm. According to Coleman JJ et al., 9 more perforators should be preserved by utilising a large enough skin paddle (at least 5 cm broad), as smaller skin paddles may limit the flap’s vascular supply.
In the present case report a superiorly based PMF was used to reconstruct the intraoral post-fibrotomy defect. There was no evidence of infection or wound dehiscence and also there was no functional restriction like neck contracture. Aesthetically acceptable results with scars hidden underneath the collars were achieved.
The PMF has the following benefits: adequate flap thickness for the majority of orofacial defects, no visible extraoral scar on the face, no incidence of intraoral hair growth, good colour match, less donor site morbidity, simple access to the intraoral recipient site and simplicity in donor site closure. Generally, the PMF can be used to repair the oral cavity to a satisfactory degree for deficits measuring between 50 and 75 cm2. One of the benefits of using this flap is that it causes little alterations to the neck’s contour and movement.
Conclusion
The PMF is a versatile flap which can be used as a potential reconstructive option in OSMF cases with aesthetically acceptable results. The patient complied well because the incision was made well away from the face, where the scar was concealed by a collar. However, the platysma flap technique is difficult and requires more time to perform during surgery and it should be mastered accurately.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethical Approval and Informed Consent
Ethical approval was not required for this article as it is a case report. Before commencing the study a written informed consent was obtained from the participant as deemed necessary.