
Abstract
Schwannoma (neurilemmoma or neurinoma), is a benign tumor arising from Schwann cells that comprise the myelin sheaths surrounding peripheral nerve. They are encapsulated, usually solitary and slow-growing. Approximately 25%-45% of schwannoma occurs in the head and neck region. Intraoral incidence of schwannoma is 1%-12%. The most common intraoral site is tongue (1%) followed by palate, floor of the mouth, buccal mucosa, gingiva, lips and vestibular mucosa, retromolar region is the least common site. We describe a rare case of lingual schwannoma involving the left lateral part of tongue in a young male presented with a slow-growing, asymptomatic, painless mass on the left lateral part of tongue for several years. Magnetic resonance images demonstrated a well-defined almost oval-shaped isolated mass with uniform intensity on T2 weighted images relative to surrounding muscles. Patient was managed with complete surgical excision of the tumor and has not shown any recurrence in the follow-up period of 1 year. Schwannoma of tongue is a rare tumor of head and neck region. The diagnosis should be based on histopathological examination and in some cases after immunohistochemistry findings. Complete transoral resection allows removal of tumor to avoid recurrence and also avoids causing morbidity of tongue function.
Introduction
Schwannoma also known as neurilemmoma or neurinoma, is a benign tumor arising from Schwann cells that comprise the myelin sheaths surrounding peripheral nerve. They are encapsulated usually solitary and slow-growing.1, 2
Approximately 25%-45% of schwannoma occurs in head and neck region. 3 Intra oral incidence of schwannoma is 1%-12%.4, 5 The most common intraoral site is tongue (1%) followed by palate, floor of the mouth, the buccal mucosa, the gingiva, the lips and the vestibular mucosa, retromolar region is the least common site.5, 6, 7 In the central tumors, the mandible is more frequently affected than the maxilla. In the head and neck region, it is usually associated with large cranial nerve, especially the trigeminal nerve. The sensory nerves are more commonly affected.
Schwannoma may arise at any age of life but the peak incidence is in the third and sixth decade of life. There is no sex predilection. 7 Schwannoma almost never undergo malignant transformation 8 when compared to neurofibromatosis. These tumors are symptomatic when large enough to be noticed by the patient. When completely excised schwannoma does not show recurrence. 9 The treatment of choice is complete surgical excision of the tumor.
We describe a case of schwannoma involving the left lateral part of tongue in a young male.
Case Report
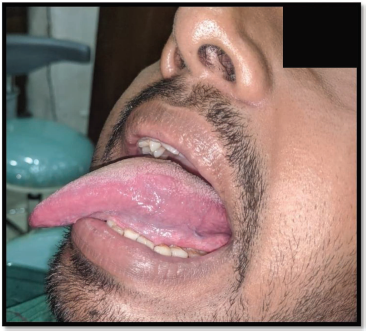
A 28-year-old male patient presented with a slow-growing, asymptomatic, painless mass on the left lateral part of tongue for several years. Clinically a palpable, nodular mass measuring 3.5 × 2.5 cm, which was well-circumscribed, involving posterolateral part of the tongue, non-ulcerated, non-tender, non-fluctuant, non-reducible, non-compressible, non-pulsatile and fixed to overlying tongue mucosa was detected (Figure 1). No cervical lymphadenopathy was evident on head and neck examination. His past medical history was non-contributory. Patient’s family history including any salivary gland tumor was not significant. No other significant findings were observed during an oral examination.
Clinical Aspect of Painless Mass on Left Lateral Border of Tongue.

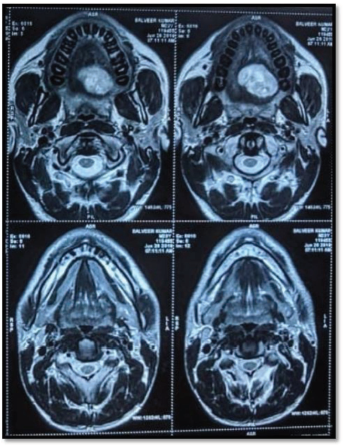
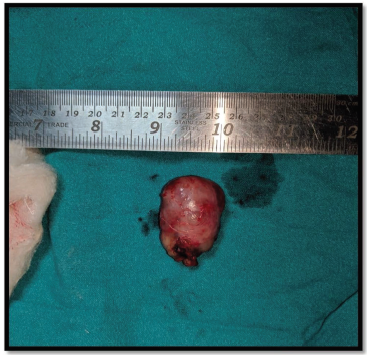
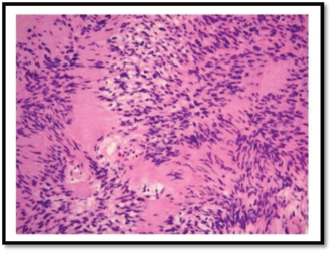
Magnetic resonance (MR) images demonstrated a well-defined almost oval-shaped isolated mass with uniform intensity on T2 weighted images relative to surrounding muscles (Figures 2 and 3). An excisional biopsy was done under general anesthesia (Figure 4). Grossly the mass was well encapsulated, measuring 3.5 × 2.5 cm in diameter, and had a firm gray-white cut surface (Figure 5). A complete excised mass was sent for histopathological examination. Histological section characterized by palisading of the spindle-shaped schwannoma cell (Figure 6) also known as Verocay Bodies (hematoxylin and eosin 100×). The diagnosis was schwannoma of the tongue. There was no associated nerve identified. The patient has not shown any recurrence in the follow-up period of 1 year (Figure 7).
MR Imaging Demonstrated a Well-circumscribed Single Intensity Mass on T2 Weighted Images (Sagittal View).

MR Imaging Demonstrated a Well-circumscribed Single Intensity Mass on T2 Weighted Images (Axial View).
Surgical Excision of Lesion.

Well-encapsulated Mass Measuring 3.5 × 2.5 cm.
Follow-up Period of One Year Without Recurrence.
Antoni A Areas Composed of Palisading Spindle Cell also Known as Verocay Bodies Hematoxylin and Eosin 100×.
Discussion
Schwannoma is a very rare condition and benign neoplasm that may arise from any peripheral nerve, cranial nerve or autonomic nerve. Schwannoma were first described by Verocay in 1908 10 and Stout described their schwanian derivation. 9 Most of the schwannoma present as a painless mass. They produce symptoms such as voice changes, dysphagia, throat discomfort when they approach more than 3 cm in dimension.
For the presented case report the final diagnosis was made by histopathological analysis of the specimen that revealed a well-circumscribed lesion composed of spindle-shaped cells with elongated or wavy nuclei known as Verocay Bodies arranged in a palisading pattern (Antoni type A). The diagnosis was made as a schwannoma of tongue with no evidence of an associated nerve.
Schwannoma usually occurs as a solitary lesion when multiple they can be associated with neurofibromatosis 11 Approximately 15% of neurofibromatosis patients will have malignant transformation which is in marked contrast to the typical behavior of a schwannoma. 12
To confirm the diagnosis, choice of imaging modality is MR imaging. MR imaging is superior to computed tomography (CT) because in MR imaging schwannoma of tongue appears as an isointense to muscle on T1, hyperintense to muscle on T2 weighted images. These tumors are well-demarcated and do not invade the surrounding musculature. 13
There are two histological variants of schwannoma identified. The first pattern is Antoni type A, consisting of closely packed Schwann cells arranged in a palisading pattern with elongated nuclei known as Verocay Bodies. The second pattern known as Antoni type B consists of loosely arranged Schwann cells in the form of meshwork of reticulum fibers and microcytes. 14
Differential diagnoses of schwannoma may be lipoma, traumatic fibroma, neurofibromas, leiomyoma, granular cell tumor, rhabdomyomas, hemangiomas, lymphangiomas, and adenoma which is based on clinical appearance of neoplasm and speed of growth. 15
The treatment of choice for schwannoma of tongue is the surgical excision of the lesion. The most common route of excision is transoral route due to easy accessibility. Several other approaches have been reported including submandibular, 16 suprahyoid pharyngotomy, 17 and transhyoid approach. 18 All these approaches were for schwannoma of the base of the tongue. Currently, the use of a CO2 laser has been reported for excision of base of the tongue. The goal of surgical therapy is achieving complete resection which makes recurrence a rare occurrence. 18
Conclusion
Schwannoma of tongue is a rare tumor of head and neck region. The diagnosis should be based on histopathological examination and in some cases after immunohistochemistry findings. Complete transoral resection allows removal of tumor to avoid recurrence and also avoids causing morbidity of tongue function.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethical Approval and Informed Consent
Ethical approval was not required for this article as it is a case report. Before commencing the study a written informed consent was obtained from the participant as deemed necessary.