
Abstract
Here, we report a case of adenomatoid odontogenic tumor in anterior maxilla in a young girl aged 14 years. Adenomatoid odontogenic tumor is a rare, benign, and distinct slow-growing odontogenic neoplasm which results in painless expansion of jaws. It usually occurs in the anterior maxilla followed by posterior maxilla and rarely in the mandible with an age range of 3 to 82 years and a relative frequency of 2.2% to 7.1% and showing a female predilection (1.9:1).
Introduction
Of all odontogenic tumors, adenomatoid odontogenic tumor represents 3% to 7%. It exhibits duct-like structures and tubular characteristics microscopically similar to ameloblastoma which led to this lesion being designated as “adenoameloblastoma.” 1
“WHO classification of odontogenic tumours in 2005 classified adenomatoid odontogenic tumour into the first group of tumors (odontogenic epithelium without ectomesenchyme)”. 2 Stafne in 1948 first identified it as a benign lesion originating from the odontogenic epithelium and stated that it is nonaggressive and slow growing in nature. Some authors have even classified these lesions as harmatomas. 3 Its distinctive clinicopathologic profile although not pathognomonic is considerably different among other odontogenic tumors because most adenomatoid odontogenic tumors occur in association with an unerupted maxillary cuspid in teenage girls. 4 Adenomatoid odontogenic tumor appears in 3 clinical variants: follicular, extrafollicular, and peripheral type. 5 Here, a case of adenomatoid odontogenic tumor is presented highlighting the importance of accuracy of diagnosis of such lesions for its efficient management.
Case Report
A 14-year-old female patient reported with a chief complaint of painless swelling with occasional pus discharge in her anterior maxillary region for the past 6 months. The lesion was not associated with any history of trauma, pain, and lymphadenopathy. The skin over the lesion and the surrounding area appeared normal and the margins were diffuse. On palpation, there was no local rise in temperature, no tenderness, and no discharge.
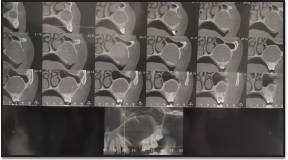
Intraoral examination revealed swelling of size approx 4 cm × 3 cm obliterating the left side labial vestibule extending from maxillary lateral incisor to the second molar mediolaterally. Superoinferiorly, it extended from middle third of labial aspect of edentulous area in relation to 24,25 to the depth of labial vestibule. The swelling was firm in consistency. On palpation, swelling was nontender, nonfluctuant, nonpulsatile, noncompressible, and nonreducible with no discharge (Figure 1). Patient gave a history of surgical dental extraction 6 years back in the same region. Cone beam computed tomography was advised which revealed a round, well-circumscribed, radiolucent lesion with well-defined distinct radiopaque margins 4 cm × 3 cm in size extending from left maxillary lateral incisor to the maxillary second molar extending into the maxillary antrum (Figure 2). Based on the history of extraction, clinical and radiographic findings, a provisional diagnosis of adenomatoid odontogenic tumor was made. Aspiration of the lesion was done, which was negative.
Clinical Photograph Showing Painless Swelling Intraorally.

CBCT Revealing Unilocular Radiolucency With Well-Defined Radiopaque Margin.
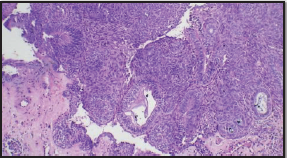
Incisional biopsy of the lesion was done under local anesthesia. The sections revealed fibrocollagenous tissue lined focally by a stratified squamous epithelium with a superficial nodular proliferation of round to polygonal cells in solid sheets and duct-like structures and rosettes suggestive of odontogenic epithelial cells. Eosinophilic fibrillar material was present between tumor cells and within duct-like structures, also focal calcification was noted. Based on these findings, a histopathologic diagnosis of adenomatoid odontogenic tumor was made (Figure 3). Enucleation of the tumor under general anesthesia was chosen as the treatment option.
Photomicrograph (H&E Stain, ×40) Showing Typical Duct-Like Structures Among Cellular Clusters and Rests of Odontogenic Epithelium.
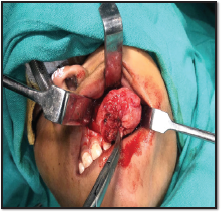
After inducing general anesthesia and intraoral site preparation, a crevicular incision was placed extending from the left maxillary lateral incisor to the left maxillary second molar and a trapezoidal flap was raised followed by subperiosteal elevation of the flap to expose the tumor mass. The labial cortex was found to be resorbed. Careful excision of the lesion along with its capsule was done in toto. Gross examination of the specimen showed a single spherical-shaped soft tissue mass measuring approximately 3 cm × 3 cm (Figure 4).
Intraoperative View Showing Lesion.
The surgical specimen (Figure 5) was sent for histopathologic examination with a confirmatory diagnosis of adenomatoid odontogenic tumor. Regular clinical follow-up of the patient was done for a period of 28 months and no signs of recurrence were observed.
Surgical Specimen: A Spherical Mass Measuring 3 cm × 3 cm (Approx).

Discussion
The first identifiable case of adenomatoid odontogenic tumor is difficult to pin down because this lesion has been given numerous names, the earliest reported case was from Norway by Harbitz in 1915. 6 Stafne reported the first series of adenomatoid odontogenic tumor in 1948 under the title “epithelial tumours associated with developmental cysts of the maxilla.” 7 Bernier and Tiecke were the first to publish a case using the name “adeno-ameloblastoma.” In an attempt to “remove unjust stigma from this lesion” and to eliminate the risk of unnecessarily mutilating surgery for patients who had the tumor that seemed to be occurring because of use of the term “adenoameloblastoma,” in 1961, Gordon 4 introduced the term “ameloblastic adenomatoid tumour.” Philipsen and Birn proposed the name “adenomatoid odontogenic tumour” in 1969. Shortly thereafter, the term was adopted in the initial edition of the World Health Organization’s Histological Typing of Odontogenic Tumors, Jaw Cysts and Allied Lesions in 1971 and was retained in the second edition in 1992. 4
Adenomatoid odontogenic tumor has been reported in patients from 3 to 82 years of age, its predilection for young patients is established in literature, 69% cases are diagnosed between the ages of 10 and 19 years. Pericoronal (dentigerous, follicular) adenomatoid odontogenic tumors are diagnosed at an earlier age than other variants. 4
Overall, the tumor is diagnosed approximately twice as frequently in women. In the third decade, adenomatoid odontogenic tumor is nearly 4 times more frequently seen in females in patients who are older than 30 years, it is diagnosed nearly twice as commonly in males. 4
Adenomatoid odontogenic tumor may occur anywhere within the jawbones or the gingiva. Before the age 30, nearly twice as many lesions are diagnosed in the maxilla, while after age 30, almost twice as many lesions are diagnosed in the mandible. Adenomatoid odontogenic tumors have been reported to be mostly asymptomatic; delayed eruption of permanent tooth especially in anterior maxilla, or slow-growing bony expansion commonly lead to the discovery of adenomatoid odontogenic tumor. Peripheral lesions present as a gingival-colored mass that ranges from 1 to 1.5 mm in diameter and 10 times more prevalent in the maxillary gingiva than in the mandibular gingiva. Nasal obstruction was reported in conjunction with rarely encountered large maxillary lesions. Gingival lesions are most often painless.4, 8, 9
Clinically, gingival lesions cannot be distinguished from gingival fibromas, peripheral giant cell lesions, peripheral cemento-ossifying fibromas, or from other peripheral odontogenic tumors, such as ameloblastoma, odontogenic fibroma, calcifying odontogenic cyst, and calcifying epithelial odontogenic tumor. 4
The lesion is usually unilocular and radiolucent, containing fine calcifications (a feature that differentiates it from other lesions) which is well demarcated with smooth cortical border. Displacement of neighboring teeth is a more common finding compared to root resorptions. Approximately, 78% of adenomatoid odontogenic tumors show calcified deposits and are associated with the crown of an unerupted permanent tooth in 71% of cases.1, 4, 10
Gross examination of majority of tumors reveals a soft, roughly spherical mass with a veritable fibrous capsule. Upon sectioning, the tumor may exhibit white to tan, solid to crumbly tissue, or one or more cystic spaces of varying size; minimal yellow brown fluid to semisolid material; fine, hard “gritty” granular material; and one to several larger calcified masses. Additionally, intact dentigerous specimens demonstrate the crown of a tooth embedded in the solid tumor mass or projecting into a cystic cavity. 4
The tumor is made up of a cellular multinodular proliferation of spindle, cuboidal, and columnar cells in a variety of patterns; usually scattered duct-like structures, eosinophilic material, and calcifications in several forms and a fibrous capsule of variable thickness.3, 4
Due to uniformly benign biologic behavior of nearly all typical adenomatoid odontogenic tumors and consistent presence of a well-developed fibrous capsule, complete surgical excision—usually accomplished by enucleation and curettage—is the treatment of choice (excision in toto). 4
Adenomatoid odontogenic tumor is referred to as “slow” or “very-slowly growing” but no report of measurements of growth rate over a course of time could be located. The large size of a few of the reported cases in young children from underdeveloped countries indicate that some cases have shown at least a moderate rate of growth. Recurrence is exceptionally rare of these lesions.6, 7, 10
Conclusion
Adenomatoid odontogenic tumor is an uncommon odontogenic lesion, but it can be usually identified from its clinical and radiographic appearance. The clinicoradiographic profile of adenomatoid odontogenic tumor observed in this study agrees with that commonly reported in literature. It is important to correctly distinguish and diagnose this lesion to eliminate the risk of unnecessarily mutilating surgery for patients. Conservative surgical enucleation is the treatment of choice as the lesion is well encapsulated and can be separated from the bone easily. Also, its recurrence is very rare.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.