
Abstract
Central giant cell granuloma (CGCG) is a locally aggressive and benign lesion that can cause significant destruction of the jaw. World Health Organization has defined it as “localized benign but sometimes aggressive osteolytic proliferation consisting of fibrous tissue with hemorrhage and haemosiderin deposits, presence of osteoclast-like giant cells with reactive bone formation.” Surgical resection is often necessary to manage the condition, and subsequent reconstruction is crucial for functional and aesthetic restoration. This case report presents a case of CGCG of the maxilla in a 61-year-old female patient who presented with a chief complaint of swelling on the right side of the palate for 2 months. Preoperative histological examination of the biopsy specimen concluded the lesion to be a CGCG. The report discusses the surgical approach, preoperative planning, and postoperative outcomes of the lesion.
Introduction
Central giant cell granuloma (CGCG) is a rare benign bone lesion that primarily affects the maxillofacial region predominantly affecting young adults.1–3 It is characterized by osteolytic, blood-filled cavities containing multinucleated giant cells within a fibrous stroma. 2 The etiology and pathogenesis of the lesion are still unclear; however, several authors have described various factors including, intraosseous hemorrhage, inflammation, local trauma, and genetic anomalies. 4 From a histological perspective, CGCG exhibits similarities with giant cell lesions of genetic disorders such as neurofibromatosis type I, Noonan syndrome, and cherubism.5, 6 The prevalence of CGCG in the general population is estimated to be 0.0001%. 7 Notably, 60% of cases are diagnosed before the age of 30. 8 CGCG exhibits two types of clinical behavior: aggressive and non-aggressive types. There are some prerequisites for the lesion to be called an aggressive lesion: pain, paresthesia, root resorption, cortical bone perforation, and a high rate of postoperative relapses. 9 Although benign, CGCG can cause significant damage to the jawbone, leading to functional impairment and facial deformities. Surgical removal is often the preferred treatment, but it can result in significant bone loss and aesthetic concerns, which require reconstruction techniques. Various reconstructive methods have been used, including autogenous bone grafts, allografts, and vascularized free flaps. However, these techniques have limitations, such as donor site morbidity and complex surgical procedures.
Case Report
A 61-year-old female patient came to the Department of Head & Neck (OMFS), Kalyan Singh Super Speciality Cancer Institute, Lucknow, with the chief complaint of swelling in the upper right region of the hard palate for 2 months (Figure 1). The medical history revealed hypertension for 2 years for which the patient is taking medications occasionally. The patient also gives a history of tobacco consumption for 25 years; however, the patient stopped consuming tobacco for 2 months. There was no facial asymmetry.
Preoperative Lesion.

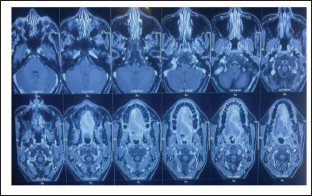
Initial clinical evaluation demonstrated a moderate swelling on the hard palate crossing the midline in the tooth region of 17–21, which was tender on palpation. The mass subsequently grew larger over 2 months. Contrast-enhanced magnetic resonance imaging (CEMRI) scan (Figure 2) revealed a 3.7 × 3.4 × 4.1 cm expansile lytic lesion without any evidence of periosteal thickening or reaction. A blood test was advised to rule out any pathology associated with bone metabolism. All parameters were normal, including alkaline phosphatase and PTH. The levels of calcium phosphorus, C-reactive protein, and erythrocyte sedimentation rate were all within normal limits. The lesion appeared well-defined and abutted the adjacent soft tissues without evidence of infiltration. CGCG was diagnosed, and a surgical resection was indicated. The tumor was exposed and removed after lifting the palatal flap under general anesthesia.
CT Scan Showing the Lesion
In addition to resection of the lesion and analyzing the various fragments anatomically and pathologically, deep curettage of the surrounding bone was performed until seemingly healthy bone tissue was observed. Surgical curettage was completed, and a palatal flap was repositioned and sutured using silk 3/0 (Figure 3). Moreover, an acrylic splint was placed following suture placement for further support of the palatal mucosa (Figure 4). The resected material, consisting of approximately 10–15 fragments with a diameter of 1.5–3 cm, was subjected to histological examination. The diagnosis of a central giant cell granuloma (CGCG) was validated by the distribution of giant perinuclear osteoclast cells, their clustering in islets around hemorrhagic suffusion foci, the cytological aspect of the mononuclear elements, the presence of neo-osteogenesis, and the tumor’s negative immunostaining with the anti-P63 antibody, (which ruled out a giant cell tumor). The postoperative course was uneventful, with no immediate complications.
Immediate Postopeartive and Closure of the Defect.

Immediate Postoperative Profile Picture With Acrylic Splint.

Discussion
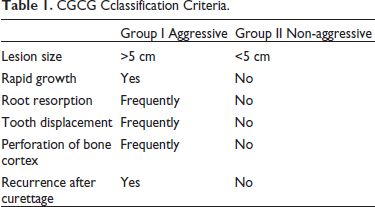
The term “reparative GCCG” was first used by Jaffe to characterize lesions that he thought were a reaction to an intraosseous traumatic hemorrhage of the jaw. 1 Though it can manifest at any age, CGCG primarily affects children and young adults, with about 75% of cases reported before the age of 30 years. 10 With an anterior predilection, more than 70% of CGCG occurs in the mandible and <30% in the maxilla. 11 While most maxillary lesions in the literature are described as occurring in the anterior region, these lesions in the mandible seem to be evenly distributed between the anterior and posterior regions. 12 Choung et al. 9 classified the lesion into two types: aggressive and non-aggressive types, which are described in Table 1.
CGCG Cclassification Criteria.
The treatment option for CGCG ranges from curettage to resection. Eisenbud et al. 13 and his associates stated that, in the event of a recurrence, a peripheral ostectomy involving bone resection and a surgical vacuum must be carried out. An en bloc resection provides the best chance of complete recovery. An en bloc surgical resection with a 5-mm margin of healthy tissue was the course of treatment for 18 patients with aggressive CGCG in a study conducted by Bataneih et al. 14 Relapses occurred only in one patient.
Unal et al. 15 suggest using a diamond cutter to create micro-perforations of the resection field in order to obtain safety margins. To promote better bone healing, curettage, osteotomy, tumor resection, and micro perforations were carried out in this study. Remarkably, only a small number of cases reported following en bloc resection had iliac crest graft bone reconstruction.
Both intralesional injections of corticosteroids and systemic calcitonin administration via nasal spray or subcutaneous injection have been used with success. Denosumab therapy could be considered a therapeutic option in large CGCGs of the jaws. The results of a study conducted by Bredell et al. 16 suggested a successful treatment option. A treatment length of not shorter than 12 months is recommended. When used in tandem with aggressive GCCG, interferon-α appears to be able to slow down the lesions’ rapid growth, reduce their size, and even help to consolidate the bone. However, surgical intervention is still required to remove the lesion. 17 Furthermore; the literature has documented several investigations and distinct experiences demonstrating the beneficial effects of antiosteoclastic and antiangiogenic molecules in the management of CGCG. These drugs, however, are poorly studied in the medium term and have extremely variable efficacy, along with severe short-term side effects. 18
There have been reports of recurrence rates ranging from 11% to 49%. This vast variation is explained by the spectrum of lesions, which ranges from the less common large painful and aggressive lesion to the more frequent smaller painless non-aggressive lesion. 19 To minimize the chance of recurrence, aggressive lesions like the one described in this report should be treated with total surgical resection. The challenge, though, is figuring out how aggressive the patient was before surgery.
Conclusion
Clinical, radiological, biological, and anatomopathological factors all play a crucial role in diagnosing CGCG. It is essential to conduct mandatory assessments of calcium and phosphorus levels to differentiate between bone metabolism disorders and hyperparathyroidism-related brown tumors. Despite the significant radiological volume of the lesion, we were able to achieve a conservative and non-mutilating approach through surgical exploration. Initially, the surgical team opted for a conservative therapeutic approach upon discovering the lesion. The synthesis of clinical and radiological findings, along with profound theoretical knowledge, guides the diagnostic hypothesis and the therapeutic approach. However, the most effective way to fully recover from the condition is through block surgery procedure resection. In every situation, routine observation is essential due to the high risk of relapse.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.