
Abstract
Objective
To investigate postoperative risk factors for transient urinary incontinence (TUI) after different en bloc holmium laser enucleation of the prostate (HoLEP) techniques.
Methods
We retrospectively analyzed 169 consecutive patients who underwent HoLEP using the original en bloc technique (n = 41), en bloc with early mucosal strip detachment technique (n = 72), and three horseshoe-shaped incisions technique (n = 56) to treat bladder outlet obstruction from January 2017 to October 2019. Preoperative variables and surgical quality indexes were compared between the groups. TUI was defined as any hygienic or social problem caused by involuntary loss of urine at 2 weeks postoperatively. The postvoid residual urine volume, maximum urinary flow rate, and International Prostate Symptom Score (IPSS) were assessed.
Results
Among all three techniques, the three horseshoe-shaped incisions technique was significantly associated with the lowest incidence of TUI and the lowest IPSS. Although not statistically significant, the three horseshoe-shaped incisions group also showed a trend toward a faster enucleation time. No life-threatening intraoperative complications occurred in any group.
Conclusion
Use of three horseshoe-shaped incisions in en bloc HoLEP prevented urethral sphincter damage with a low rate of postoperative TUI. Further long-term, multicenter comparative assessment is required.
Research Registry number: 6848
Keywords
Introduction
Holmium laser enucleation of the prostate (HoLEP), originally reported in clinical practice by Gilling et al. 1 in the 1990s, has shown promising results, and its use has become widespread as a standard treatment option for benign prostatic hyperplasia (BPH). Many studies have demonstrated significant advantages of HoLEP, including a low complication rate and shorter catheterization times than those of transurethral resection of the prostate. 2 , 3 More recent descriptions of various approaches to en bloc procedures have been published, mainly to address the goals of improving the effectiveness of enucleation, better visualization on the surgical plane, and optimal safety compared with the traditional three-lobe method.4–6 However, many studies have indicated a significant initial rate of transient urinary incontinence (TUI) as a complication after HoLEP. 7 , 8
Although most patients who develop TUI after HoLEP experience spontaneous recovery within 3 months, 9 TUI reduces patients’ general quality of life and is a significant concern for clinicians. Many authors have proposed that TUI after HoLEP may be caused by excessive damage to the external sphincter and bladder neck during resection of adenoma tissue. 10 , 11 Various modified techniques have been proposed with a focus on reducing the rates of postoperative TUI. Miernik and Schoeb 12 recently presented promising results in their report of a “three horseshoe-like incisions” approach to HoLEP as a time-efficient and simple-to-learn technique; however, the prevalence of postoperative incontinence was not reported.
In our institution, we initially used a holmium laser to reproduce the original en bloc technique reported by Scoffone and Cracco 4 in 2016. Because of frequent postoperative TUI, we began using the en bloc approach with early mucosal strip detachment and then deliberately modified the approach to use three horseshoe-shaped incisions for better postoperative outcomes. In the present study, we reviewed the overall performance of three different en bloc HoLEP techniques—the original en bloc technique, the en bloc with early mucosal strip detachment technique, and the three horseshoe-shaped incisions technique—in 169 patients with the goal of reducing the rate of postoperative TUI.
Materials and methods
Patient selection and parameters measured
This retrospective study was performed to investigate TUI after different HoLEP techniques. The study was approved by the Kaohsiung Medical University Hospital Institutional Review Board (KMUHIRB-E(I)-20180313). All procedures were performed in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The requirement for informed consent was waived.
From January 2017 to October 2019, 169 consecutive patients who underwent HoLEP by the same experienced surgeon (SCW, who had performed >100 HoLEP procedures with the traditional three-lobe technique prior to this study) were admitted to the Department of Urology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan. The inclusion criteria were an International Prostate Symptom Score (IPSS) of >8, postvoid residual urine volume (PVR) of >50 mL, maximum urinary flow rate (Q max) of <15 mL/s, and (in men) BPH causing acute urinary retention. The exclusion criteria were voiding disorders not associated with BPH and a history of prostate surgery. Preoperative urodynamic studies were routinely performed according to the standard protocol in our department. Suspected prostate carcinoma was confirmed or ruled out by prostate biopsy if the prostate-specific antigen (PSA) concentration or digital rectal examination results were abnormal. From January 2017 to February 2018, the first 41 patients underwent the original en bloc HoLEP procedure performed as previously described by Scoffone and Cracco. 4 From February 2018 to December 2018, 72 patients underwent en bloc HoLEP with early mucosal strip detachment. From December 2018 to October 2019, 56 patients underwent the modified three horseshoe-shaped incisions technique with early apical release.
The following patient data were recorded: age, preoperative PSA concentration, prostate volume measured by transrectal ultrasound of the prostate, history of 5-α-reductase inhibitor use, history of use of antiplatelet agents with aspirin that were not discontinued prior to surgery, history of recurrent urinary tract infections occurring more than three times in the past 3 months, IPSS, PVR, and Q max. The following perioperative outcomes were also recorded: overall operative time, enucleation time, morcellation time, decrease in hemoglobin concentration, and final prostate specimen weight. The follow-up protocol included documentation of the IPSS, PVR, Q max, postoperative PSA concentration, and incidence of TUI 2 weeks postoperatively. TUI was defined as any hygienic or social problem caused by involuntary loss of urine according to the guidelines of the International Continence Society and quantified by the complaint of any involuntary leakage of urine. 13 All complications were recorded within 30 days after surgery.
This study was registered at the Research Registry (https://www.researchregistry.com/, registration number 6848). The reporting of this study conforms to the STROBE guidelines. 14
Laser and operative equipment
A 100-W holmium-YAG laser (Lumenis, Yokneam, Israel) equipped with a 550-μm end-firing fiber at a maximum energy of 1.6 J and frequency of 50 Hz was used. A 26-Fr continuous-flow laser resectoscope (Olympus, Tokyo, Japan) with a 30° down lens and a mechanical tissue morcellator (VersaCut; Lumenis) were also used. These devices and settings were used for all procedures performed in this study. A 20-Fr three-way Foley catheter using normal saline for continuous bladder irrigation was inserted at the end of the surgery. Generally, the flow of the irrigation fluid was tapered overnight and terminated the morning of postoperative day 1. The catheter was removed on postoperative day 2 after confirming cessation of hematuria. All patients received both prophylactic antibiotic treatment using cefazolin 30 minutes before the operation and postoperative antibiotic treatment using cefazolin until discharge.
Surgical procedures
Original en bloc HoLEP (performed as described by Scoffone and Cracco 4 )
Step 1. An inverted U-shaped laser incision was made around the verumontanum. This step allowed blockage of vessels caudal to the prostate adenoma and identification of the surgical capsule.
Step 2. A mucosal incision was made between the median and left lobes, lateral to the verumontanum. Enucleation of the left lobe was then begun from the 5- to 3-o’clock position. The bladder neck was retrogradely incised at the 5-o’clock position. The lateral lobe was gradually dissected to the anterior commissure by laser incision and mechanical sweeping. The anterior bladder neck fiber was visualized before dividing.
Step 3. The median lobe and the rest of the bilateral lobes were dissected with a retrograde approach, and the whole adenoma was lifted. The posterior bladder neck was then divided entirely.
Step 4. The only remaining connection between the adenoma and prostate capsule was the mucosal strip, which was contralateral to the verumontanum. The mucosal strip was divided by laser incision.
Step 5. Hemostasis was completed by laser in most cases. Adjuvant hemostasis by electrocoagulation was required in very few cases.
En bloc HoLEP with early mucosal strip detachment
Steps 1 and 2. The first two steps were similar to the original en bloc HoLEP technique described above.
Step 3 (early mucosal strip detachment). Once the surgical plane of the bilateral lobes was created, the mucosal strip was found contralateral to the verumontanum and divided by laser. The prostate adenoma was then dissected along the ventral capsule, and the anterior bladder neck fiber was identified and divided by laser.
Step 4. The median lobe and the rest of the bilateral lobes were resected with a retrograde approach. The whole adenoma was lifted, and the posterior bladder neck was divided. The whole prostate adenoma was then pushed into the bladder.
Step 5. Hemostasis and morcellation were performed similarly to the original en bloc HoLEP.
Modified three horseshoe-shaped incisions technique with early apical release
Step 1 (ventral scoring). The ventral mucosa contralateral to the verumontanum was scored from the 11- to 1-o’clock position and expanded bilaterally and dorsally (Figure 1(a)).

(a) The en bloc process is started by scoring the ventral mucosa opposite the verumontanum from the 11- to 1-o’clock position with expansion bilaterally and dorsally. (b) The urethral crest is cut around the seminal colliculus using an inverted U-shaped cut; it is then extended circumferentially, joining the previous ventral scoring demarcation to create a circle of “white line” to release the apex from the external sphincter. (c) The mucosal strip is located between the anterior capsular plane and bilateral adenoma and divided by laser incision, and another inverted U-shaped cut is made. (d) After continuous dissection between the anterior capsular plane and the ventral prostate, the spoke-like fiber of the anterior bladder neck is divided by laser, and another inverted U-shaped cut is created. (e) The bladder lumen is entered anteriorly between the capsular plane and the adenoma. (f) The median lobe and the rest of the bilateral lobes are dissected in a retrograde fashion along with the surgical capsule. This process gradually moves toward the posterior bladder neck and gently divides the remaining attached fiber.
Step 2: First incision. The urethral crest was cut around the seminal colliculus in an inverted U-shape. After reaching the surgical plane, the bilateral lobes were gradually dissected to the anterior commissure, and the median lobe was partly lifted by laser incision and mechanical sweeping.
Step 3. The enucleation process was carried out circumferentially until it joined the previous ventral scoring demarcation, leading to a “white line” circle to release the apex from the external sphincter (Figure 1(b)).
Step 4: Second incision—early mucosal strip detachment. Once the mucosal strip was visualized between the anterior capsular plane and bilateral adenoma, it was divided by laser incision. Another inverted U-shaped cut was then made, which allowed the external sphincter to be completely freed from the prostate adenoma (Figure 1(c)).
Step 5: Third incision. After continually dissecting along the anterior capsular plane and the ventral prostate, the spoke-like fiber of the anterior bladder neck was divided by laser, and another inverted U-shaped cut was created (Figure 1(d)). The bladder lumen was entered anteriorly, between the capsular plane and the adenoma (Figure 1(e)).
Step 6. The median lobe and the rest of the bilateral lobes were dissected with a retrograde approach along with the surgical capsule. This process was advanced toward the posterior bladder neck, and the remaining attached fiber was gently divided (Figure 1(f)).
Step 7. The whole prostate adenoma was mobilized and pushed into the bladder. Hemostasis and morcellation were performed similarly to the original en bloc HoLEP.
Statistical analysis
General data were analyzed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA), and differences were deemed statistically significant at p < 0.05. Analysis of variance was performed for the three groups to identify significant differences if the data were normally distributed. If the data were not normally distributed, the Wilcoxon rank sum test was used to evaluate any differences. Parameters were compared with Fisher’s exact test or the chi-square test. A sample size calculation revealed that 150 patients were needed to show statistical significance in our study.
Results
As shown in Table 1, no statistically significant differences in any of the baseline characteristics were found among the three groups. There were no significant preoperative differences in the history of 5-α-reductase inhibitor use, incidence of recurrent urinary tract infections, or use of antiplatelet agents with aspirin. The intraoperative parameters of the three groups are shown in Table 2. Although not statistically significant, the three horseshoe-shaped incisions group showed a trend toward a faster enucleation time (95% confidence interval, 30.06–37.51). No significant differences were found in the overall operation time or operation efficiency. Use of a monopolar instrument for hemostasis was not needed in any patient.
Characteristics of patients undergoing HoLEP
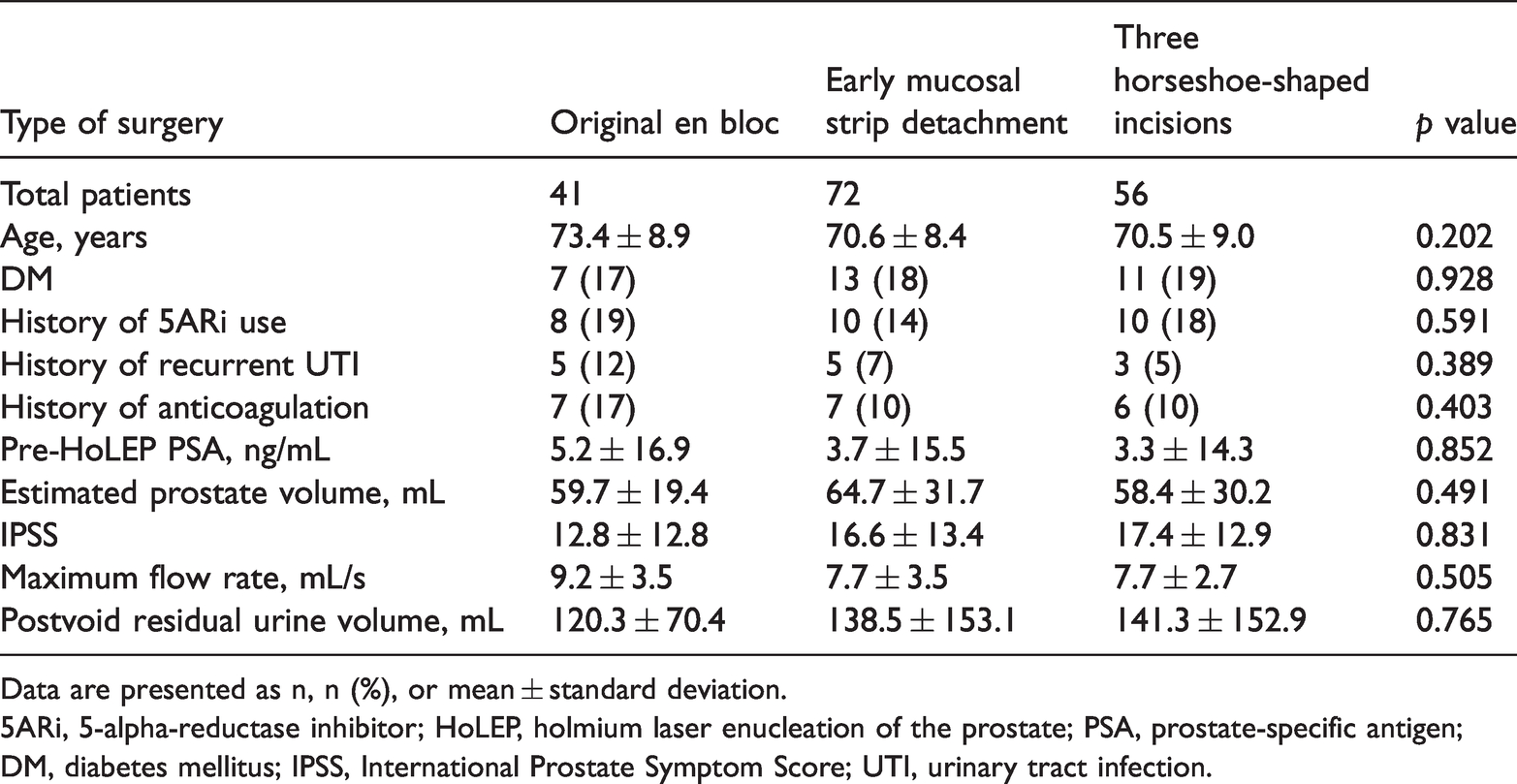
Data are presented as n, n (%), or mean ± standard deviation.
5ARi, 5-alpha-reductase inhibitor; HoLEP, holmium laser enucleation of the prostate; PSA, prostate-specific antigen; DM, diabetes mellitus; IPSS, International Prostate Symptom Score; UTI, urinary tract infection.
Intraoperative parameters

Data are presented as n, n (%), or mean ± standard deviation.
CI, confidence interval.
Table 3 shows a significant difference in the incidence of TUI at 2 weeks postoperatively, with 14.0% in the original en bloc group, 9.7% in the early mucosal strip detachment group, and 3.5% in the modified three horseshoe-shaped incisions with early apical release group (p = 0.001). A significant difference was also seen in the incidence of late postoperative urinary incontinence in the third month (p = 0.004), but there was no significant difference in the incidence of late postoperative urinary incontinence in the 6th and 12th months (see Appendix Table). The mean IPSS was also significantly different among the groups (95% confidence interval, 2.04–7.335; p = 0.031): 6.0 ± 4.5 in the original en bloc group, 3.5 ± 3.1 in the early mucosal strip detachment group, and 2.8 ± 2.5 in the three horseshoe-shaped incisions group. The postoperative mean Q max was 16.5, 19.3, and 17.9 mL/s in the three groups, respectively, showing an obvious improvement but without statistical significance. At 2 weeks postoperatively, the differences in the PVR were clearly lower, but they did not reach statistical significance.
Two-week postoperative parameters

Data are presented as n (%) or mean ± standard deviation.
TUI, transient urinary incontinence; HoLEP, holmium laser enucleation of the prostate; PSA, prostate-specific antigen; IPSS, International Prostate Symptom Score; CI, confidence interval.
No major life-threatening intraoperative complications occurred in any of the three groups. Overall, few postoperative complications occurred: one (2.4%) patient in the original en bloc HoLEP group required a blood transfusion, and five (12.1%) patients in the original en bloc HoLEP group and two (2.7%) patients in the early mucosal strip detachment group developed acute urinary retention after catheter removal. In addition, one (2.4%) patient in the original en bloc group developed a Clavien–Dindo grade 3 complication (prolonged bleeding that required bipolar electrocoagulation).
Discussion
TUI is one of the most frequently occurring complications after HoLEP and a concern for both patients and clinicians.15–17 Moreover, many studies have shown a significant initial rate of stress urinary incontinence after the enucleation maneuver based on the surgical plane, regardless of the wavelength used. Although several modified en bloc techniques have been described, only a few studies have compared the rate of postoperative TUI among different methods. Miernik and Schoeb 12 reported a time-efficient en bloc HoLEP technique using three horseshoe-like incisions but did not report the prevalence of postoperative incontinence. To the best of our knowledge, their report is the first to describe the postoperative effect of the three horseshoe-shaped incisions technique on TUI compared with other en bloc HoLEP techniques for treatment of prostatic adenoma.
Several studies have shown a postoperative incidence of TUI ranging from 1.7% to 10.0%. 16 , 18 , 19 Shigemura et al. 7 found that the prevalence of TUI was >10% for 497 patients treated by dozens of different surgeons. The current study showed a TUI rate of 3.5% in the three horseshoe-shaped incisions group. The main reason for the wide variation in the occurrence of TUI after HoLEP across studies may be the different definitions of postoperative TUI. Many studies have defined TUI solely on the basis of patient reports of transient stress urinary incontinence. However, the current study defined TUI as any involuntary loss of urine, including postvoid dribbling and urge or stress urinary incontinence. We believe that this specific definition of TUI is more suitable for diagnosis because any kind of involuntary urine leakage plays an important role in reduced quality of life.
Since the introduction of the en bloc HoLEP technique in 2016 by Scoffone and Cracco, 4 en bloc techniques have proven advantageous for optimal visualization of the correct plane and superior resection efficacy. We previously performed surgeries that reproduced the original en bloc method used by Scoffone and Cracco. 4 In this method, however, the mucosa of the sphincter (or “mucosal strip”) is often fixed anterior to the 10- to 2-o’clock position and incised at the end of the procedure. It is reasonable to consider that the sphincter might tear and become distended when the scope is moving, thus causing postoperative TUI. In 2018, we deliberately modified their approach by performing en bloc HoLEP with early mucosal strip detachment to avoid the frequent occurrence of postoperative TUI. The mucosa strip was released from the apex of the adenoma before dividing the prostate adenoma from the bladder neck, which should be done to reduce excessive sphincter damage. However, a review of the procedure videos showed that the mucosa of the urethral apex was easily distended by the scope when dissecting both lateral lobes because the external sphincter was still fixed. Our modification of the three horseshoe-shaped incisions technique is designed to address this problem. First, the demarcation of the “ventral scoring” is used to begin the procedure, leading to very early release of the external sphincter from the prostate adenoma. This may lower the probability of postoperative TUI because it decreases the possibility that the external sphincter around the apical gland will be distended and damaged by the scope movement. Second, the residual connecting mucosa strip is removed by “early detachment” (which is accomplished by the second horseshoe-shaped incision), thereby completely freeing the external sphincter from the prostate adenoma. We believe that using the three horseshoe-shaped incisions technique combined with ventral scoring and early detachment of the mucosa strip can eliminate the vital and challenging step of dissecting the apical gland from the capsule by aiming to preserve the external sphincter.
Saitta et al. 20 presented a detailed description of the modified en bloc technique with a focus on early apical release. They aimed to preserve the sphincter’s mucosa by early apical incision and considered early apical release to be fundamental for avoiding sphincter distension and tearing. However, they did not record the overall performance of different en bloc HoLEP techniques by the same study group. Our concept of ventral scoring plus early detachment closely resembles the technique described by Saitta et al. 20 We structured our surgical steps accordingly and considered the combination of step 1 (ventral scoring) and step 3 (early mucosal strip detachment) to be early apical release. We believe that we have provided sufficient evidence to show that the modified three horseshoe-shaped incisions technique provides a low incidence of postoperative TUI among different en bloc techniques.
The present experience with the three horseshoe-shaped incisions technique also revealed other advantages. First, this technique provides a potential benefit in decreased enucleation time, although this factor did not reach statistical significance in the present study. A longer enucleation time is correlated with an increased risk of urethral sphincter injury due to distention and stretching by manipulation of the resectoscope during the operation, leading to the occurrence of TUI. This study showed that the overall operation time was not significantly associated with postoperative TUI. However, too many confounding factors were involved in determining exactly how much time was spent in the overall operation, including anesthesia delay, equipment setup, and procedure demonstration, for example. Lerner et al. 21 found that the operative time was not significantly correlated with postoperative TUI and that the analysis was complicated by many confounding issues. Second, based on guidance provided by natural anatomical landmarks, the use of three horseshoe-shaped incisions may allow complete dissection of the adenoma, thus ensuring the quality of the enucleation without residual adenoma. Additionally, because the approach allows the surgeon to follow the natural anatomical structure with easy recognition of the dissection plane, the operation efficiency (average of 0.5 g/min) was superior to that in previous reports of the retrieval efficiency. 22 , 23 The overall efficiency of the three horseshoe-shaped incisions technique in the present study (0.5 g/min) was not inferior to that of earlier reported methods described by Miernik and Schoeb 12 (average of 0.47 g/min).
This study showed no increase in the postoperative complication rate in the three horseshoe-shaped incisions group. We believe that the low complication rate resulted from optimal visualization of the enucleated adenoma edges because of efficient irrigation. In the classic three-lobe method, it is in fact difficult to coagulate the edges of the dissection plane, which increases blood loss because of poor visibility as a result of the chaotic irrigation compared with laminar irrigation between the capsule and enucleated adenoma. In the current study, no patients in the three horseshoe-shaped incisions group needed postoperative transfusion or reoperation.
Several modified techniques focusing on prevention of incontinence have been presented. Gong et al. 24 detailed the steps of a modified HoLEP technique that resulted in only 3 cases of postoperative transient stress incontinence in 189 patients, all of whom recovered spontaneously within 3 months postoperatively. Minagawa et al. 25 reported a novel en bloc method with anteroposterior dissection, in which the incidence of postoperative incontinence at 2 weeks was 2.7%. Another study using a modified en bloc HoLEP technique with early apical release showed a low rate of stress urinary incontinence (5.8%) at 1 month postoperatively. 20 Compared with other studies of en bloc HoLEP, the current study revealed similar outcomes for the incidence of TUI.
This study has several limitations. Postoperative urinary incontinence caused by detrusor hyperactivity or sphincter hypoactivity was not excluded by urodynamic studies. However, considering the risk of adverse effects and the invasive nature of urodynamic studies and that postoperative urine leakage is a short-term condition in most cases, the necessity of such examinations is controversial. In addition, all operations in this study were performed by a single surgeon, and the sample size was small. No large studies to date have compared the effects of different en bloc HoLEP techniques performed by other experienced surgeons on the incidence of postoperative TUI. In this study, we primarily focused on “transient” incontinence (occurring for only 2 weeks) after different en bloc HoLEP techniques; however, a long-term follow-up study including late complications is ongoing, and its data will be reported. Finally, this study was not randomized and was conducted at a single health center. Moreover, there were no records regarding an increase in the learning curves throughout the study. We recommend that further studies be conducted by multiple surgeons with different levels of experience and in multiple centers.
Conclusion
Use of the three horseshoe-shaped incisions technique is an efficient and reliable procedure for patients with obstructive symptoms of BPH. 12 In the present study, modification of this technique prevented urethral sphincter damage and had a low rate of postoperative TUI. Further comparative assessment of long-term data and reports of different surgeons’ experiences are required.
Footnotes
Acknowledgements
The authors would like to thank all individuals who participated in this research and all medical professionals who cared for the patients.
Authors’ contributions
Chun-Hsuan Lin wrote the original draft. Wen-Jeng Wu and Hung-Lung Ke performed the data curation. Ching-Chia Li and Jhen-Hao Jhan were involved in creation of the figures. Sheng-Chen Wen was responsible for project administration.
Declaration of conflicting interest
The authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Availability of data and material
Data will be available by contacting the corresponding author. All strains and reagents used in the studies are available upon request.