
Abstract
Schwannoma, which is also known as neurilemmoma, is a type of tumor that arises from the peripheral nerve sheaths. Cases of schwannomas located in different regions have been reported. Some schwannomas present as asymptomatic masses, while others cause discomfort, such as pain and numbness. Magnetic resonance imaging (MRI) is a valuable diagnostic tool. A 23-year-old woman presented to our hospital with a mass in the left axilla that was misdiagnosed as mammae erraticae. The patient also considered the condition to be mammae erraticae for approximately 14 months because of a lack of symptoms. MRI was recommended by a surgeon from the galactophore department. A giant schwannoma was found. The mass was surgically excised, while preserving the continuity of the long thoracic nerve. Routine histopathological analysis confirmed the presence of a benign schwannoma. Schwannomas located in the axilla are rare and may be easily misdiagnosed as mammae erraticae or enlarged lymph nodes. Early investigation is necessary to make the diagnosis, and surgical excision is usually curative.
Keywords
Introduction
Schwannomas are preliminarily benign tumors that are derived from the peripheral nerve sheaths. They can be encountered at all ages, but they are particularly observed within the second and fifth decades of life. They may arise in any region of the body.1–3 The mass may be misdiagnosed as another type of tumor because of certain features. 4 Schwannomas are often asymptomatic but they sometimes cause symptoms, such as pain, numbness, or paraesthesia, because of the mass effect. Surgical excision is generally a curative choice. This report documents the case of a patient with surgically treated schwannoma in the axilla, which originated from the long thoracic nerve.
Case report
A 23-year-old woman presented to our hospital with a mass in her left axilla. The mass had increased in size over the preceding 14 months. The patient was counselled for the first time by her family doctor to undergo investigation, such as ultrasound or magnetic resonance imaging (MRI), to obtain a differential diagnosis, but she refused because she thought it was not necessary. Six months later, the mass was slightly larger compared with the initial size. She still believed that it was a mammae erraticae and did not undergo any examinations. Two months before visiting our hospital, she realized that the situation was worse than what she thought because the contour of the mass could be seen on the skin surface. She was then referred to the galactophore department and underwent MRI examination.
There was no pain or paraesthesia in the involved area. Moreover, no associated family history or clinical features were recorded. Physical findings on the initial examination indicated a solid ovoid movable mass in the left axilla, measuring 12 cm in length and 8 cm in width. The mass was partly covered by the pectoralis major muscle. Regular preoperative blood tests showed normal results. MRI revealed that the mass was subcutaneous and homogeneous (Figure 1). With a clinical diagnosis of a nerve tumor and a preoperative anaesthetist assessment, the patient underwent surgical excision of the tumor. We explained to the patient that nerve grafting might be performed if the involved nerve could not be preserved. The tumor arose from a nerve in the left axilla. It was well encapsulated and located eccentrically to the nerve trunk (Figure 2). The involved nerve was identified as the long thoracic nerve based on the electrical stimulation response. Because it was not possible to use a tourniquet, enucleation was performed under loupe magnification to protect the nerve during the dissection procedure. A longitudinal incision was made parallel to the direction of the nerve fascicles. The content in the capsule was carefully and gradually excised to ensure that the nerve fascicles remained undisturbed as much as possible. The fascicles entering or running over the tumor were dissected carefully. For the region without a clear margin between the tumor and the nerve, the adhering tissue between the capsule and epineurium was left intact to reduce the risk of nerve injury. Any observed bleeding was thoroughly assessed and managed via bipolar coagulation and local compression. Vascular pedicles for the tumor blood supply were identified and ligated gently. The specimen was sent for histopathological examination. Subsequent histological examination confirmed the diagnosis of schwannoma. In this case, the typical presence of Antoni A and Antoni B areas was observed (Figure 3). The patient was discharged from the hospital 1 week after surgery. Because the histology was benign, she did not undergo any further treatment. At the 3- and 6-month follow-up appointments, she reported no discomfort or dysfunction. No nerve deficit was observed at the 9-month follow-up.
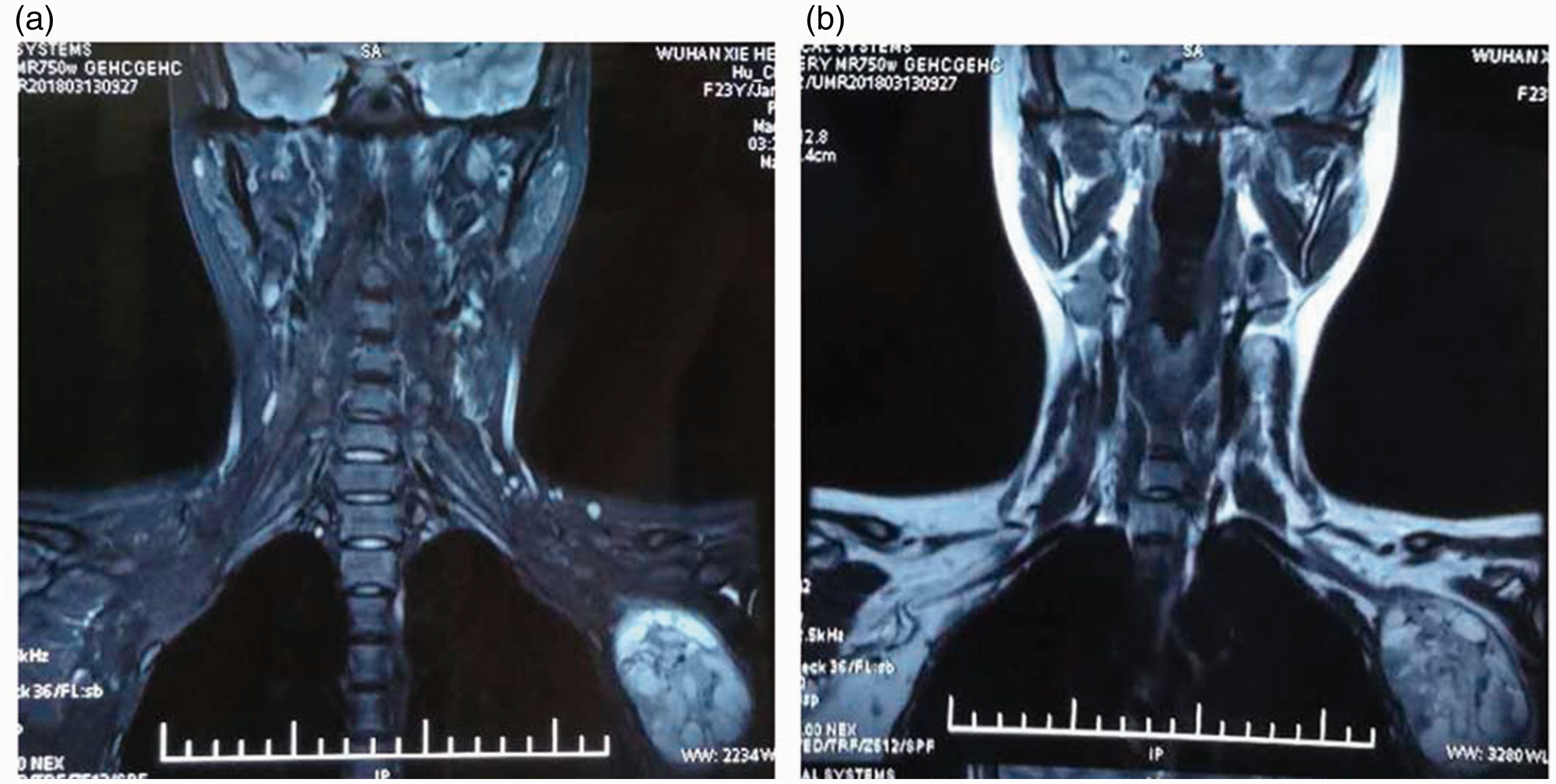
Neck and upper trunk MRI. T2-weighted sagittal image (a) and T1-weighted sagittal image (b).

Intraoperative image. The tumor was excised while the nerve trunk was identified and preserved (black arrow).

Histopathological examination. Antoni A type tissue and Antoni B type tissue were observed (hematoxylin and eosin staining), which are typical characteristics in schwannomas.
Written informed consent was obtained from the patient to publish this case report and any accompanying images. The study was approved by the Ethics Committee of Union Hospital of Huazhong University of Science and Technology.
Discussion
Schwannomas are a type of benign tumor that commonly arises from the Schwann cells in the nerve sheath. There is no associated predilection for race or sex. 5 Schwannomas commonly occur in the head and neck region or in the extremities.6,7 They are often slow growing and asymptomatic, and therefore, they are often misdiagnosed as a lipoma or fibroma, or as enlarged lymph nodes. 8 Although extremely rare, multiple schwannomas and malignant peripheral nerve sheath tumors have been reported. 9
The slow growth of schwannomas make early diagnosis difficult. MRI can be useful in determining a diagnosis because it can provide important information on the tumor extent, tumor size, and anatomical relationship with surrounding tissues, which are useful for preoperative diagnosis and appropriate planning of surgical management. 10 However, it cannot provide dynamic information. Additionally, imaging studies do not allow for an unequivocal diagnosis, and histopathological examination is conclusive. 11 In the literature, only 6% of schwannomas were preoperatively diagnosed by clinical, radiological, and fine needle cytology results. 12 Therefore, biopsy is a more reliable diagnostic method. Both Antoni A type tissue with interwoven bundles of long bipolar spindle cells and Antoni B type tissue with its loose texture can typically be observed in schwannomas. Nuclear palisading and Verocay bodies may also be observed in certain areas. 13
Extra-capsular and intra-capsular enucleation are two main techniques for surgical treatment of schwannoma. It is possible to remove the mass using enucleation without nerve fascicle injury. These techniques have been shown to be effective and safe in different studies.14–18 Postoperative nerve deficit complications, such as sensory disturbance or motor weakness, have also been reported at follow-up15,19,20 and have been considered to be associated with a large tumor size and a long history.21–23 However, the degree of nerve deficit usually ranges from grade I to grade II and it is usually reversible. 18 However, it was also reported that enucleation cannot be performed in some special schwannoma cases. 24 In our experience, careful microsurgical dissection in a bloodless field is important to avoid damaging the involved nerve during the enucleation procedure. Complete exposure of the tumor with a proximal and distal margin can facilitate the operation. Concomitant intraoperative neurostimulation is useful to confirm the involved nerve. 25 Some studies recommend that only symptomatic tumors or those demonstrating enlargement during follow-up will be excised surgically. 25 In this case, we performed surgical excision of the tumor although it was asymptomatic. Schwannomas that are located in the axilla are easy to misdiagnose as mammae erraticae or enlarged lymph nodes. We recommend early surgical excision because an increase in tumor size can increase the risk of neurological deficit after surgery. Loupe magnification and microsurgical dissection are advocated during dissection to protect the involved nerve fascicles. As reported in our patient, enucleation of the tumor was performed without producing a neurological deficit at the 9-month follow-up. Awareness of this entity may reduce the risk of misdiagnosis. Early intervention can then be initiated.