
Abstract
The origin of ameloblastic fibrosarcoma (AFS) or ameloblastic dentinosarcoma in the background of ameloblastic fibroma has been widely reported in literature. To the best of our knowledge, the malignant transformation of a benign ameloblastoma to an aggressive variety of AFS has never been reported. Here, we report a rare case of follicular ameloblastoma of mandible in a 16-year-old female, who initially presented with a painless slow growing swelling, gradually transformed into a painful, aggressive variety of AFS requiring extensive surgery and chemoradiation therapy.
Introduction
Ameloblastomas are the most common odontogenic tumors, excluding odontomas. They are benign lesions with locally invasive behavior with a high tendency to recur after inadequate excision. Several morphologic variants have been described including follicular, plexiform, acanthomatous, granular cell, basaloid, and desmoplastic. Follicular, desmoplastic, and plexiform variants have been most commonly reported to undergo malignant transformation, respectively. We report a case of transformation of ameloblastoma to ameloblastic fibrosarcoma (AFS) along with brief review of literature. AFS was first described by Health in 1887. 1 As reported in most literatures, AFS or ameloblastomic fibro-odontosarcomas are usually seen to be malignant counterparts of a benign ameloblastic fibroma. 2 But in this rare case, we see a gradual change of a follicular variant, initially treated by conservative surgery into an aggressive AFS requiring radical resection and adjuvant chemoradiation.
Case Presentation
A 16-year-old female reported to Department of Oral and Maxillofacial Surgery with the complaint of ulcerated swelling on the floor of mouth (Figure 1).
Proliferative Lesion Over Anterior Region of the Mandible.

Extraoral examination revealed a smooth swelling measuring about 4 × 3 cm extending from one angle of mandible to another.
Intraoral examination revealed an ulcerated swelling measuring about 6 × 4 cm extending from second premolar on one side to first molar on the contralateral side including the floor of the oral cavity. The swelling was firm in consistency and nontender, causing difficulty in speech and deglutition.
History revealed that she was apparently asymptomatic until when she started noticing a swelling over the right side of her jaw and numbness over her lower lip and chin region. The swelling was painless and did not produce any gross facial asymmetry. She visited numerous local doctors where she was prescribed medications for pain. She visited a community health center from where she was referred to our center. The patient was examined, evaluated, investigated, and biopsy was done. She was diagnosed to be a case of ameloblastoma of mandible (follicular variant).
Orthopantomogram revealed a unilocular lesion with cortical expansion. Curettage of the lesion was done (Figure 2) considering the size of the lesion, her age, and as the patient was unwilling for any kind of resective procedure. After 8 months of surgery, locoregional recurrence was seen. Thorough curettage of the lesion was done again. After 10 months, recurrence was seen again, and unilateral resection of the mandible was done this time followed by reconstruction with a reconstruction plate on the affected side from symphysis to angle. After a year following surgery, there was recurrence of the lesion and breakage of the reconstruction plate. The plate was removed with aggressive resection of soft tissue recurrence. After 9 months, bilateral recurrence was seen, and bilateral mandibular resection was done along with reconstruction from angle to angle.
Orthopantomogram Revealing a Mixed Radio-Opaque Radiolucent Multilocular Lesion Over the Body-Ramus Region of the Mandible on the Right Side.

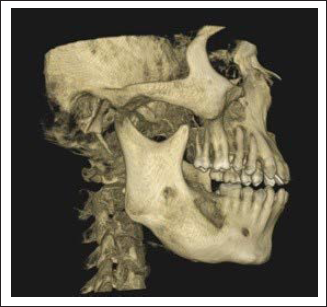
The histopathological and immune-histochemical diagnosis confirmed it to be AFS of mandible. She then underwent 30 fractions of adjuvant postoperative radiotherapy (60 Gy) followed by 1 cycle of concurrent chemotherapy after having been diagnosed with sarcoma. Then, the patient absconded, and complete cycle could not be finished. After 2 years, the lesion recurred, this time over the left side of jaw, fungating intraorally. The cone beam computed tomogram (CBCT) revealed a destructive osteoexpansile lesion involving right body-ramus region of the mandible having mixed radiolucent and radiopaque pattern (Figure 3). Then, she again visited oral and maxillofacial surgery department at King George’s Medical University, a year later. The computed tomogram revealed a 2 × 2.5 cm, ill-defined heterogeneously enhancing hard tissue lesion. The lesion infiltrated the skin, soft tissue, and the gingivobuccal sulcus. Another heterogeneously enhancing lesion was noted in the left buccal mucosa and gingivobuccal sulcus. The lesion was causing erosion/destruction of the underlying anterior border of ramus with intraosseous extension. It was seen infiltrating the overlying masseter muscle as well.
Cone Beam Computed Tomogram (CBCT) Showing Involvement of the Right Side of Mandible by the Lesion.
Investigations
Orthopantomogram showed an osteoexpansile multilocular mixed radiolucent radiopaque lesion on the right side of the mandible with thick cortical rimming.
CBCT of face showed (Figure 3) mixed radiopaque-radiolucent lesion with expansion of both the cortices initially on the right side of the mandible, and later on bilaterally.
Contrast enhanced computed tomogram of face and neck revealed heterogeneously enhancing soft tissue lesion suggesting recurrent lesion of the mandible. Multiple lymph nodes (measuring ∼1 cm in short axis diameter) noted with perinodal fat stranding in the axial sections.
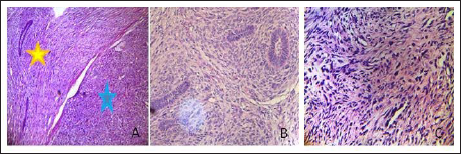
On incisional biopsy, histopathological examination and report (Figures 4 and 5) of initial biopsy showed benign odontogenic epithelium arranged in an island and net pattern (yellow star) (A) and other malignant hypercellular mesenchymal tissue comprised of spindle and stellate cells, exhibiting nuclear pleomorphism and hyperchromasia (blue star) (B,C) (hematoxylin and eosin [H&E] stain, ×10, ×40, ×40).
A Benign Odontogenic Epithelium Arranged in an Island and Net Pattern (Yellow Star) (A). Malignant Hypercellular Mesenchymal Tissue Comprised of Spindle and Stellate Cells, Exhibiting Nuclear Pleomorphism and Hyperchromasia (Blue Star) (B,C) (H&E stain, ×10, ×40, ×40).
Immunohistochemical Findings Revealed That the Tumor Cells Were Positive for Cytokeratin (A), Vimentin (B), and Ki-67 (C) (IHC Stain, ×10, ×40, ×40).
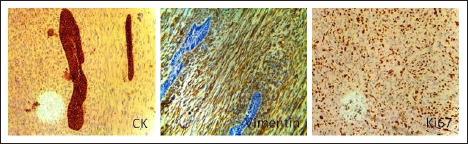
Histopathological examination revealed malignant neoplasm displaying mesenchymal and epithelial differentiation. The epithelial component was composed of ameloblastic islands made up of columnar cells arranged in a palisaded pattern with a central area of stellate reticulum while the mesenchymal component displayed storiform pattern in a fibromyxoid stroma (Figure 4). Focal area showed fibroma also. Immunohistochemical findings revealed that the tumor cells were positive for Cytokeratin, Vimentin, and Ki67 and negative for S100. Final diagnosis was malignant transformation of follicular ameloblastoma to AFS of mandible. Immunohistochemistry (IHC) revealed that the tumor cells were positive for Cytokeratin (A), Vimentin (B), Ki-67 (C) (IHC stain, ×10, ×40, ×40) (Figure 5).
Differential Diagnosis
Ameloblastic fibroma
Ameloblastic fibro-odontoma
Desmoplastic ameloblastoma
Cemento-ossifying fibroma
Osteosarcoma
Ewing sarcoma
Metastatic tumors to jaws
Osteoblastic metastatic carcinoma
Treatment
Enucleation and curettage of the benign lesion were followed by curettage again 8 months later due to recurrence. After 10 months from the date of second curettage, unilateral resection with wide surgical margins and reconstruction with a reconstruction plate from symphysis to angle was done. Then after 1 year 9 months, there was recurrence again and this time, bilateral resection of the lesion with 2 to 3 cm margin with continuity defect of the mandible and reconstruction from angle to angle with a reconstruction plate was done. Adjuvant radiotherapy up to 50 Gy dosage followed by 1 cycle of chemotherapy of regimen composed of cyclophosphamide, actinomycin, and vincristine were given. After one and half year, because of recurrence, the same regimen of chemotherapy was again administered.
Outcome and Follow-Up
Recurrent disease which was managed by repetitive surgeries with wide margins and adjuvant chemoradiation, prolonged the life span of the patient by approximately 4 years and 6 months. Ultimately, the patient succumbed to the disease.
Discussion
Most of the cases of AFS are located in the posterior part of the mandible. 3 Malignant odontogenic tumors (MOTs) comprise of a small percentage of the odontogenic neoplasms, with an incidence usually ranging from 0% to 6.1%. 4 The occurrence of odontogenic sarcomas is less frequent than carcinomas among the MOTs. 5
In this case, the tumor has affected the posterior part of mandible in a 16-year-old girl. The most common age predilection of AFS is usually below 20 years among the younger population. 6 The male to female ratio is 1.6:1 and it is more common in the mandible (79%) in comparison to that of maxilla (21%). 7 The initial presentation of the lesion was painless but subsequently became painful with its progression. Radiographically, the tumor appeared to be a mixed radiopaque radiolucent osteoexpansile lesion with irregular borders on 1 side at its initial presentation which ultimately became a bilateral massive destructive bony lesion with soft tissue involvement even after multiple surgeries. This report accounts for the gradual transformation of a benign follicular ameloblastoma to an aggressive variety of AFS. A conservatively managed ameloblastoma of posterior mandible transformed into an aggressive odontogenic sarcoma, required bilateral wide resection with clear margins and reconstruction followed by adjuvant chemoradiation therapy.
The origin of AFS or ameloblastic dentinosarcoma in the background of ameloblastic fibroma has been widely reported in literature. But rarely an AFS is seen to arise from a pre-existing ameloblastoma. Acanthomatous and desmoplastic variants have been reported to undergo malignant transformations. The most common malignant lesions arising from ameloblastomas are malignant ameloblastoma and ameloblastic carcinoma. There is no evidence of any histologic variant of a conventional ameloblastoma transforming into an AFS till date.
Rais and El-Mofty 8 reported a case of desmoplastic ameloblastoma transforming into squamous cell carcinoma.
In this case, AFS showed recurrence potential following initial conservative surgical treatment. Compared with the initial lesions, recurrent lesions exhibit decreased epithelial components and increased pleomorphic and mitotic mesenchymal components. AFS is usually characterized by local invasiveness rather than regional or distant metastasis.
Local recurrence rates of AFS are reported to be 37% in areas of the gingiva, floor of the mouth, and neck. 6 It is very difficult to differentially diagnose AFS because it falls in the category of a wide array of lesions having similar clinical, radiologic, and histologic findings although ameloblastic fibroma remains the chief differential diagnosis.
Generally, the treatment of choice for AFS is surgical excision with wide, tumor-free margins, and long-term follow-up. Adjuvant chemotherapy has also been used with moderate success.9, 10 In this case, multiple surgeries and adjuvant radiotherapy up to 50 Gy and 2 cycles of chemotherapy with cyclophosphamide, actinomycin, and vincristine regimen had been administered.
Nogueira Tde et al used 4,000 Gy in a case where the tumor was not completely resectable, with disease-free survival for 2 years. 11 Gatz et al reported a case where patient with multiple recurrent AFS responded to a regimen of ifosfamide and doxorubicin and remained in remission even after 14 months of therapy.
Learning Points
Malignant transformation of benign ameloblastoma is 1% to 1.3%. Therefore, aggressive surgery should be performed in benign lesions to prevent such transformations and residual tumors which might transform later.
AFS is a highly recurrent lesion and aggressive measures should be taken for management. Aggressive and radical surgery should be performed to prevent recurrences along with adjuvant chemoradiation to prolong the survival.
Regular follow-up should be done as the chances of recurrence are very high.
Although acanthomatous and desmoplastic variants of ameloblastomas are known to have malignant transformation potential, follicular variants are no exception.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.