
Abstract
Ameloblastomas with multiple histologic variants are rare odontogenic neoplasm of mandible and maxilla, and have high recurrence rates if improperly treated. They are histologically benign, slow growing, and invasive tumors. These tumors are asymptomatic in nature, unless they attain a large size to cause expansion and perforation of adjacent tissues, for which patient might seek treatment. Due to their aggressive nature and high recurrence rate, treatment remains a matter of debate. Complete excision of lesion with least morbidity would be the therapeutic challenge. However, there is an increased risk of recurrence due to local treatment. Here in, we present a large multicystic recurrent ameloblastoma on right-body-ramus region of mandible in a 45-year-old woman who was managed by hemimandibulectomy.
Introduction
Ameloblastoma, a benign locally invasive odontogenic tumor, on long term has high recurrence rate. It accounts for 1% of tumors of jaws and 11% of odontogenic tumors. 1 The first case of an “ameloblastoma like” tumor in the jaw was reported by Guzack back in the year 1826. However, the first thorough description of the tumor was given by Falkson in the year 1879. The term ameloblastoma was coined by Churchill in the year 1923. 1 Ameloblastomas, as their name implies, are true neoplasms of enamel-organ-type tissue that does not undergo differentiation to the point of enamel formation. The tumor may be derived from remnants of dental lamina, Hertwig’s sheath, or cell rests of Malassez or from the heterotrophic epithelium. As rightly described by Robinson, ameloblastoma are “unicentric, non-functional intermittent in growth, anatomically benign and clinically persistent.”1,2 They are characterized by their higher recurrence rate due to their local invasive nature, which requires an exact diagnosis and surgical treatment. However, the treatment modalities have not been clearly defined. 2 Although conservative treatment (marsupialization, enucleation, and curettage) preserves integrity of the bone, there are high chances of recurrence rate ranging from 55% and 90%, while radical treatment can leave major cosmetic and functional squeal and may require free-flap reconstruction. The recurrence rate of ameloblastoma after segmental resection was 4.5% and after marginal resection was 11.6%. 2 To prevent local recurrence, wide resection along with healthy margin bone is preferred. Therefore, the choice between these two treatment modalities seems to be an essential issue in management. This article reports the case of recurrent follicular ameloblastoma where hemimandibulectomy was done.
Case report
A 45-year-old female patient reported in August 2017 to the department of Oral Medicine and Radiology, with a chief complaint of pain and swelling on right side of her face since 1 year and numbness of her lip on the affected side. She gives a previous history of similar swelling on the same site 8 years back for which she was operated (enucleation) under general anesthesia. However, she noticed recurrence of the swelling since 1 year and complains of paresthesia, and difficulty in mouth opening and swallowing in the same since 1 year. There was no significant medical and family history. On extra oral examination, there was difference in relationship of two sides of face due to swelling noted on right side, which was measuring approximately 4 cm × 9 cm in diameter, extending superiorly from zygomatic arch and infra orbital margin inferiorly to lower border of mandible (Figure 1). The skin over swelling was stretched with no signs of inflammation. Inspectory findings were confirmed on palpation. Swelling was tender, firm in nature, with diffuse margins, and there is no rise of temperature. On intraoral examination, entire mandibular teeth were missing, soft tissue swelling was seen on the right buccal vestibule, obliterating the vestibule, and no signs of pus discharge and inflammatory component were noted. Buccal and lingual cortical plates were expanded on palpation with perforation of lingual cortical plate in lower first molar region (region 46). Based on patient’s history, and on general examination, a provisional diagnosis of recurrent ameloblastoma was given with a differential diagnosis of ameloblastic carcinoma, calcifying epithelial odontogenic tumor an odontogenic keratocyst. The patient was advised for further investigations like panoramic radiograph, computed tomography (CT), and biopsy. A multilocular pattern was seen on panoramic radiograph extending from right mandibular symphysis to the right condylar region, and there was a loss of continuity in lower border of mandible suggestive of pathological fracture (Figure 2). Axial CT section showed opacification of entire mandible on right side with destruction of condyle and lower border of mandible (Figure 3). An incisional biopsy of section showed islands of ameloblastic epithelial cells with long columnar and stellate reticulum cells with reversal polarity in the nest suggestive of follicular ameloblastoma (Figure 4). Treatment was scheduled for surgical resection under general anesthesia with right hemimandibulectomy (Figure 5). Final histopathological examination reports of excised tumor mass confirmed to be follicular ameloblastoma (Figure 6). Further investigation revealed involvement of cervical and lung lymph nodes suggestive of metastasis.

Extra oral photograph.

Panoramic radiograph.

CT of axial section.
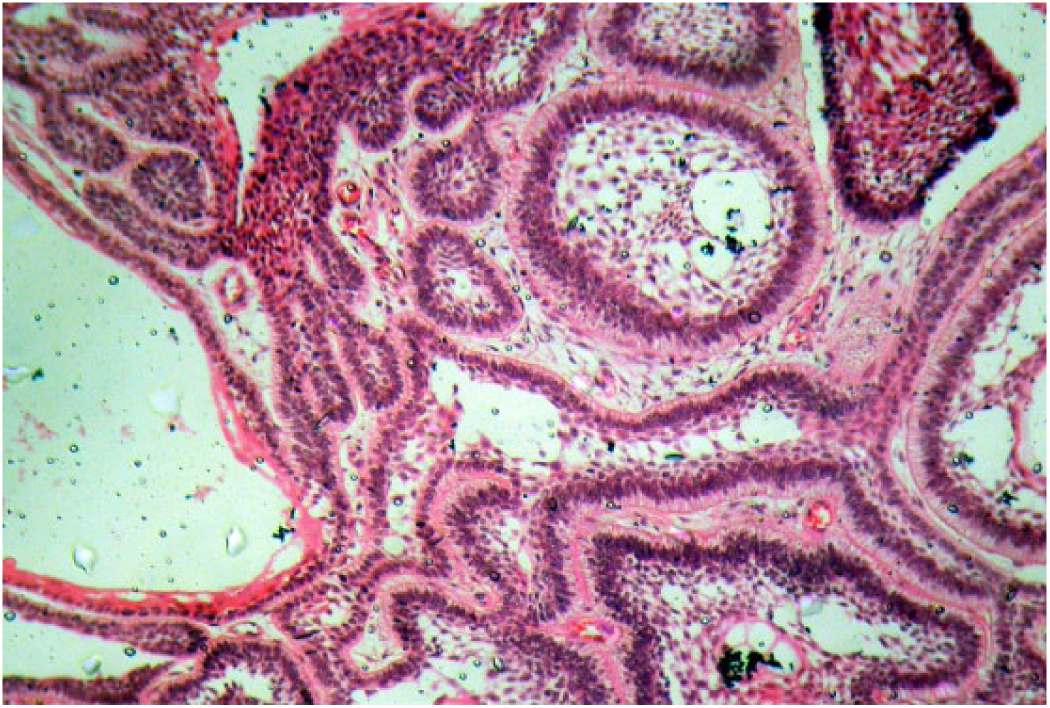
Histological picture.

Hemimandibulectomy.

Excised tissue.
Discussion
Ameloblastomas, an enigmatic group of benign odontogenic tumors, frequently invade and sometimes metastasize. They are persistent and slow growing, which spread into the marrow spaces with pseudopods, without causing resorption of the trabecular bone. 3 Due to which, margins of the tumors on radiograph and during operation are not clearly evident. Consequently, lesion recurs frequently due to left-out daughter or micro-cyst after inadequate surgical removal, demonstrating a locally malignant pattern. 4 Ameloblastoma of lower jaw can progress to variable sizes (1–16 cm) leading to deformity, mal alignment of teeth, loss of occlusion, and pathological fractures. Similarly, in our patient, clinical examination revealed a large hard swelling on right side of face leading to asymmetry of face, and expansion of buccal and lingual cortical plate with numbness of lower lip suggestive of deeper invasion of the tumor. Becelli et al. 5 observed that, in mandibular ameloblastoma, half of the patients presented with swelling of the affected region (38.3%), paresthesia of the innervated region of the mandibular nerve (13.3%), and altered occlusion of teeth (10%). Most cases of ameloblastoma in Saudi population were seen during second and third decades of life, more prevalent in males (M:F ratio of 2:1). The most common location being the posterior mandibular region. 6 Radiographically, they appear as soap bubble or have a multilocular appearance. 7 Due to its unique nature, management has been debatable. 8 The tumor cells infiltrate between the bony trabeculae of cancellous bone leaving them intact, and infiltration extends beyond radiological margin, which leads to incomplete removal of the tumor. For large ameloblastomas, in order to ensure the removal of micro-cyst and daughter cyst, resection of jaw should be done approximately 1.5–2 cm beyond the radiological limit. 9 In our case, marginal clearance of 2 cm was also achieved due to micro-cyst and daughter cyst. Histopathology of specimen revealed it to be follicular variety. To overcome the defect of mandibular arch, mandibular reconstruction is advised. The reconstruction of mandible involves the use of non-vascularized bone grafts with restoration of lost teeth using implants and supported prostheses. However, esthetics of patient was affected as there was no reconstructive surgery carried out, as the patient did not report for follow-up. Some authors recommend a follow-up period of 10 years. Others recommend initial annual follow-up of 5 years, later every 2 years for at least 25 years.10,11 However, the patient did not continue her follow-up, possibly she died because of the disease.
Conclusion
Ameloblastoma has high recurrence rate if they are not treated properly. At least 1 cm of healthy bone should be removed during surgical procedure beyond radiographically visible margins. In our patient, though radical surgery eliminated a large possibility of recurrence, patient was left with a stigma of deformity, difficulty in swallowing, and abnormal jaw movement. No reconstructive surgery was done as the patient failed to report for follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.