
Abstract
Brown tumors are seldom encountered in oral and maxillofacial practice. It is not a neoplasm but can cause considerable bone resorption and occasionally pathological fracture. The treatment is to deal with the diseased parathyroid gland which interferes with the normal calcium metabolism. In this article, we are presenting a case report of a 16-year-old female patient who came with a chief complain of swellings in the maxillary region who turned out to be a case of primary hyperparathyroidism and the primary treatment was done by focus parathyroidectomy.
Introduction
Brown tumor is not a true neoplasm but often impersonates a true neoplasm of the bone. 1 It is regarded as a nonodontogenic central giant cell granuloma which arises as a result of an imbalance between osteoclastic-osteoblastic homeostasis and calcium-phosphate regulation, leading to bone resorption with fibrous replacement of the marrow and thinning of the cortex in patients suffering from hyperparathyroidism. 2
Brown tumors most commonly involve mandible while maxillary involvement is less common. 3
Primary hyperparathyroidism occurs when there is a change in the normal mechanism of calcium homeostasis as a result of increased secretion of parathyroid hormone (PTH) from one or more parathyroid (PT) gland, in cases of PT adenoma. In secondary hyperparathyroidism, increased secretion of PTH is a result of low ionized calcium mostly seen in renal disease patient. 4 In tertiary hyperparathyroidism, increased secretion of hormone is a result of chronic renal disease which leads to over activity of PT gland independent of the underlying disease. Any of the above forms of hyperparathyroidism if not controlled and treated on time may result in brown tumor. Hyperparathyroidism can be triggered by PT adenoma, hereditary factors, PT carcinoma, or renal osteodystrophy. 5
In this article, we report a rare case of primary hyperparathyroidism, presenting as an asymptomatic brown tumor of mandible and both femur. The pattern of regression and the management will be addressed in this study.
Case Report
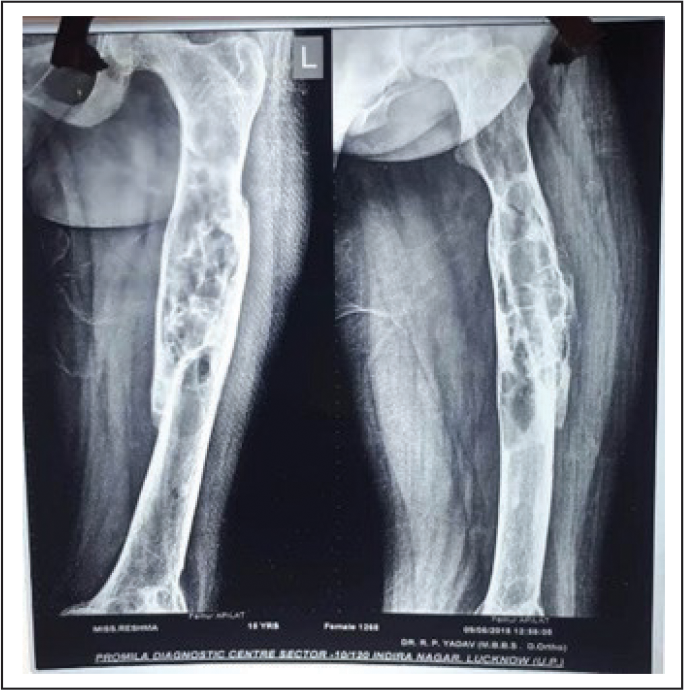
A 16-year-old female patient of Indian origin residing in Uttar Pradesh reported to the Department Of OMFS at our institute with a chief complaint of swelling in the left palate and on the buccal vestibule adjacent to 26 and 27 as shown in Figure 1. There was also swelling on the right lower border of mandible 1 cm anterior from the angle region and on the menton region. All the swellings were slowly growing, bony hard in consistency and not associated with any symptoms, nontender, and not mobile. There was also asymmetry of the face for 4 years. Patient also gave history of fracture of the left femur 3 year back while coming downstairs which was almost a result of normal body movement. There were no neurosensory deficits or cervical lymphadenopathy evident. Mouth opening was normal with full complement of teeth present except third molars. Diffuse obliteration of right mandibular buccal vestibule, retromolar trigone, and expansion of lingual cortex distal to mandibular right second molar was evident. On dental cone beam computed tomography, multiple radiolucency were observed along the mandible on both left and right side with bony overgrowth on the lower border of mandible. On ultrasonography, a well-defined isoechoic lesion measuring approx. 19×14×11 mm was seen attached to inferior pole of right thyroid gland. Sestamibi scan revealed hyperactivity of the right PT gland. Lesion showed less vascularity as compared to thyroid and was separate from thyroid gland, which gave the impression of PT adenoma. Hormone assay revealed the primary hyperparathyroid level is 1,132.00 pg/mL (11.1-79.5). Serum calcium level was 12.60 mg/dL (8.4-11.0). Alkaline phosphatase level was 968.9IU (35-105). Her femur radiograph revealed generalized decrease in bone density with multiple areas of bone resorption and improper trabecular bone formation as shown in Figure 2. Based on the medical history, clinical manifestations, and laboratory tests, the final diagnosis was brown tumor with hyperparathyroidism (HPT).
Image Showing Swelling in Left Buccal Vestibule.

Radiograph of Femur Showing Multiple Areas of Bone Resorption.
In our case, focused approach was taken at the level of inferior border of thyroid gland. Horizontal incision was given and subplatysmal flap was raised. Then layer-wise dissection was done and right inferior PT gland was exposed. Gland was separated from the surrounding tissues and capsule and then gland was excised in toto. Intraoperative blood sample was taken and postoperative (15 min after gland removal) to evaluate the hyper PTH level. Both the results were compared and a marked decrease (50%) in the postoperative hormone level was observed, then the layer-wise closure was done.
Discussion
The PT glands, situated behind the thyroid, are not regulated by the pituitary gland, but respond directly to changes in serum ionized calcium concentrations. 6
PTH plays a central role in regulating calcium homeostasis. The initial effect of PTH on bone is to stimulate osteolysis, returning calcium from bone to extracellular fluid. Prolonged exposure of bone to PTH is associated with increased osteoclastic activity, extensive bone remodeling, and osteoblastic repair.
Brown tumor is a result of metabolic disorder that can affect the entire skeleton. Hyperparathyroidism, the third-most common endocrine disorder, is the cause of such bone tumors named as brown tumor for its brownish pigmentation from hemosiderin. It was first recognized by Von Recklinghausen (Buchanan et al., 1981) almost 115 years ago, although the first example of this condition was reported by William Hunter and described by Gerhard Engel in 1864. 7 PTH releases in response to decreased level of serum calcium causing efflux of calcium from the bony skeleton. 8
Surgical treatment is focused parathyroidectomy (minimally invasive approach) where the affected gland is removed. Traditional open parathyroidectomy is where bilateral exploration is dine and the affected gland is explored and removed. It is a more invasive procedure and used where the gland anatomy is difficult to assess preoperatively. Minimally invasive video-assisted parathyroidectomy is a procedure which utilizes a 30-degree endoscope to visualize the gland and remove it by observing it in a monitor. It is different from the normal endoscopic approach as it only uses one small hole of 2.5 cm. 9 Other approaches include minimally invasive radionucleotide-guided parathyroidectomy approach for mediastinal ectopic PT tumors and thoracoscopic excision of mediastinal PT tumors.
Conclusion
Browns tumor is a rare clinical feature of a hormonal pathology and most of the patients are diagnosed accidently. Even though mortality is rare, the morbidity can scar the patient for the rest of their life.
As discussed earlier, hyperfunctioning of the PT gland is the primary cause. Patients may also seem to suffer from osteoporosis, which results in pathologic fracture as observed in our case. Tumors are often seen to involve multiple facial bones causing facial deformity, vitamin D deficiency in end-stage renal disease often worsens the condition.
The treatment options are varied but the basic concept is to tackle the cause and it can only be achieved by surgical removal of the diseased gland. An oral surgeon will treat any swelling in the oral cavity as a primary lesion but knowing certain systemic condition might prove helpful and may reduce the chances of unnecessary surgery.
A clinician should have all the tools in their bag. Otherwise, if you only have a hammer, you will see every problem as a nail.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.