
Abstract
A Becker’s nevus typically appears as a single unilateral, well-demarcated, hyperpigmented patch over the upper trunk during adolescence. It uncommonly presents as multiple and bilateral patches and rarely involves a lower extremity. We describe the unusual case of a child with multiple, bilateral Becker’s nevi of the trunk and lower extremities present since birth.
Introduction
Becker’s nevus (BN) is a cutaneous hamartoma, occurring in approximately 0.5% of the population. 1 It typically presents as a single unilateral, well-demarcated, hyperpigmented patch that usually presents on the trunk.1,2 Affected skin has increased androgen receptor density and sensitivity and becomes more prominent following puberty due to development of hypertrichosis and increased pigmentation. 3 Consequently, the majority of BN lesions are reported during adolescence and may go unnoticed prior to puberty. 2 Lesions are benign but may cause associated pruritus. An optional treatment option includes laser hair removal. Typically, patients present with a single lesion of the trunk; however, we present the case of an adolescent girl with an unusual presentation of multiple Becker’s nevi expanding to the lower extremities.
Case report
A 9-year-old healthy girl presented for evaluation of congenital skin lesions. While the lesions remained stable and asymptomatic throughout childhood, she reported increased hair growth and darkening of the lesions in the previous 6 months prior to presentation. There was no family history of similar lesions. Review of systems was unremarkable. Clinical examination was significant for multiple, well-demarcated hyperpigmented patches with irregular borders that had a “splashed on” appearance (Figure 1(a) and (b)) and some areas of hypertrichosis (Figure 2(a) and (b)) on the trunk and bilateral lower extremities, extending below the knee. A 4-mm punch biopsy from the right posterior hip over a hyperpigmented patch showed epidermal acanthosis, regular elongation of the rete ridges, hyperpigmentation of the basal layer, and an increase in the number of arrector pili muscles (Figure 3). The patient was diagnosed with multiple Becker’s nevi based on the clinical presentation and histologic findings.

Brown patches involving the right abdomen, bilateral thighs, and right lower leg: (a) anterior view and (b) posterior view.
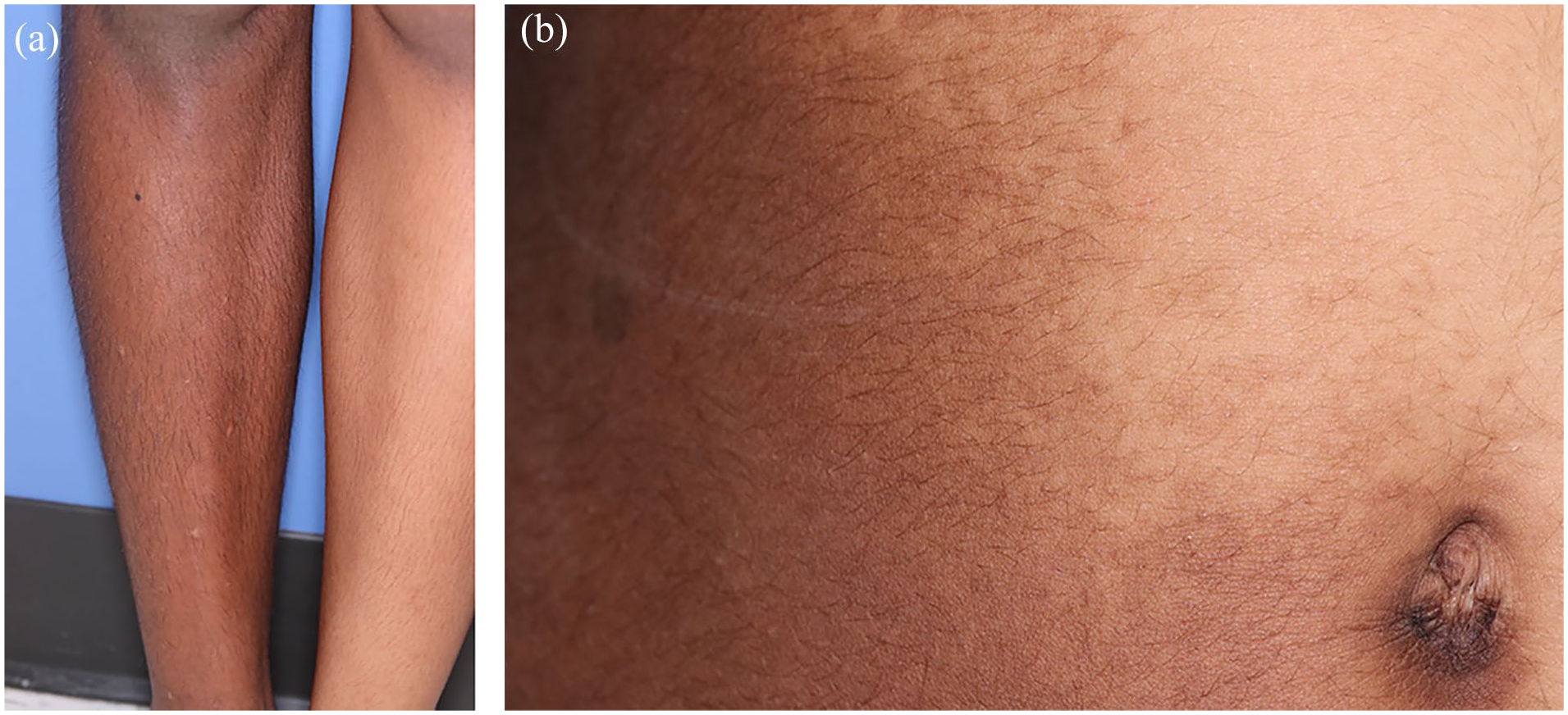
Close examination shows hypertrichosis over hyperpigmented patches: (a) lower leg and (b) abdomen.

Punch biopsy (H&E) showing epidermal acanthosis, regular elongation of the rete ridges, hyperpigmentation of the basal layer, and an increase in the number of arrector pili muscles.
Case discussion
A BN is characterized by a large, hyperpigmented patch that is often associated with hypertrichosis. Irregular borders with hyperpigmented macules at the periphery may give it a “splashed on” appearance. The lesion typically presents on the trunk during adolescence, buy may less often be congenital. Epidermal acanthosis, a hyperpigmented basal layer, and increased dermal smooth muscle bundles are seen on histology. The clinical differential diagnoses include a congenital nevus, café-au-lait macule (idiopathic, associated with neurofibromatosis or Legius syndrome, or associated with the McCune–Albright syndrome), and pigmentary mosaicism. A congenital nevus is typically brown and may have overlying hypertrichosis but can be distinguished by congenital onset, well-demarcated borders, a melanocytic pattern on dermoscopy, and histology showing melanocytic nests. A café-au-lait macule is usually smaller than a BN and can be associated with other café-au-lait macules. These lesions are characterized by hyperpigmented macules or patches or both without overlying hypertrichosis and, in contrast to BN, have smooth, well-demarcated borders. Histology shows a hyperpigmented basal layer without melanocytic nests or increased smooth muscle bundles. Idiopathic, non-syndromic café-au-lait macules and those associated with neurofibromatosis and Legius syndrome have smooth borders and are usually not biopsied as the diagnosis is clinical. A syndromic association should be suspected if there are more than six lesions and a family history or other clinical exam or personal history findings suspicious for a syndromic association. Café-au-lait macules may also be associated with the McCune Albright syndrome, however, in contrast to those previously mentioned, usually presents as large patches on the trunk that have “Coast of Maine” irregular borders. Although a biopsy is not necessary for the diagnosis, the histology would be the same as seen in the more classic café-au-lait macules. Finally, pigmentary mosaicism alone would include a single or multiple hyperpigmented or hypopigmented macule(s) or patch(es) without overlying hypertrichosis. The diagnosis is made clinically but histology would show hyperpigmentation of the basal layer only. These lesions are seen at birth and follow the patterns of cutaneous mosaicism. As first described by Happle, patterns of cutaneous mosaicism include checkerboard, following the lines of Blaschko, phylloid, large patches which cross the midline, lateralized, and sash-like. Although BN can have a checkerboard-like pattern, it can be distinguished from pigmentary mosaicism by the other distinguishing features described above. 4
Hypertrichosis in BN can be subtle, which is why biopsy was helpful in the diagnosis of our case. In fact, Rasi et al. found that only 17% of 47 patients with BN demonstrated hypertrichosis. 5 Our case represents unusual findings associated with BN, as our patient is female, has multiple nevi, and the nevi are present below the knee. BN has classically been considered to be more common in males; however, it tends to be less conspicuous in females with less hyperpigmentation and with no or subtle hypertrichosis. Thus, the true sex ratio may actually be 1:1. 3 While a BN typically appears on the chest, scapular region, or the upper arm, any area of the body may be affected and about 12% are reported on the lower extremities.2,3 On the lower extremities, it is rare for BN to present below the knee in children. 6 Multiple and bilateral BNs have been rarely reported. In a review of the literature, Antunes-Duarte et al. identified only 26 cases with multiple or bilateral BN. 1 Eleven of these had multiple bilateral BN in an asymmetric distribution, similar to our case, and only one of these patients had a congenital presentation. The genetic basis of BN was recently elucidated and found to be caused by mutations in the ACTB gene which encodes for beta-actin, a protein responsible for cell migration, proliferation, signaling, and gene expression, and may play a role in the Hedgehog pathway. 7 Cai and colleagues examined skin samples from individuals with BN and found that ACTB pathologic variants occurred only in pilar muscle. Variants were seen in only 61% of Becker’s nevi. 7 It is thought that if ACTB mutations occur early in post-zygotic development, then they will affect multiple cell lineages and give rise to a constellation of musculoskeletal findings leading to the diagnosis of BN syndrome. Whereas, when the ACTB mutations arise later in post-zygotic development, they will give rise to an isolated BN or nevi.1,7 BN is likely only seen in the mosaic form as a sporadic mutation, as it is thought to be lethal in utero when present in the zygote. 4 Pathologic ACTB variants are also implicated in Baraitser–Winter syndrome, juvenile-onset dystonia, and neutrophil dysfunction. 7
Our patient did not display features of BN syndrome, as review of systems and physical exam were negative for further abnormal cutaneous findings or musculoskeletal abnormalities. However, clinicians should be aware of syndromic associations, including ipsilateral breast hypoplasia (most common), subcutaneous fat hypoplasia, supernumerary nipples, absent or underdeveloped ipsilateral shoulder girdle musculature, scoliosis, thoracic skeletal anomalies, dental dysplasia, cardiomyopathy, and developmental delay.1,4,7 Although considered benign, there are rare reports of tumors occurring within BN, including basal cell carcinoma and desmoid tumor.8,9 BN treatment is optional and dictated by symptoms or cosmetic concerns. A combination of lasers with different wavelengths appears to provide the best results. 10 Our patient declined any treatments for her asymptomatic BN.
Footnotes
Acknowledgements
The authors thank the patient and parent for granting permission to publish this information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for patient information and images to be published was obtained from the parent and patient.