
Abstract
Introduction
A late mandibular fracture after third molar extractions is a very rare complication. The main etiological factors of it are considered to be age greater than 40, male patients, tooth position, and trauma to the mandible. The main features commonly described by the patients are occurrence after few days of extraction with history of crackling due to fracture of mandible and pain on chewing.
Material and Method
We retrospectively review the treatment chart of mandibular trauma patients and observe cases of fracture mandible angle after third molar surgery. Five patients who reported late mandibular fracture after a third molar extraction were treated either by maxillomandibular fixation (MMF) or by open reduction and internal fixation (ORIF) studied.
Results
Out of the 5 patients, 3 were treated with ORIF and 2 were treated with MMF. After maximum follow-ups, all healed well without any complications.
Conclusion
It is observed that all the causative factors should be assessed before any third molar surgery, and that this rare complication should be explained to the patients and written consent should be taken before undergoing any difficult surgical extractions.
Introduction
A third molar surgery is the most common surgical procedure done by oral surgeons worldwide, with a frequency of complications that may range from 1% to 6 %. 1 Fracture of the mandible during removal of an impacted tooth is a recognized complication and is thought to occur because of improper instruments or the use of undue force. Late mandibular fracture is an uncommon complication of removal of the impacted mandibular third molar.2, 3 The incidence rate is given as approximately 0.0046% to 0.0075% in different studies.2, 4 Late mandibular fractures usually occur about 1 to 3 weeks after the extraction, predominantly in male patients over 40 years of age with full dentition.4, 5 The purpose of this case series is to describe the clinical and radiological features of 5 cases of postoperative late mandible fractures treated in our unit and to discuss the risk factors and treatment options to deal with this complication.
Clinical Presentations of all Cases
Case 1
A 26-year-old healthy young female reported to the unit of oral and maxillofacial surgery with a history of severe pain when chewing and speaking after the surgical extraction of her left lower third molar 13 days earlier by a private practitioner. On examination, she was found to have trismus and swelling with tenderness and step defect at the left angle region of the mandible. Occlusion was normal, but the patient was unable to open her mouth properly. On bimanual palpation, there was mobility of fracture fragment distal to the second molar. An orthopantamogram (OPG) revealed a fracture line running from the extraction socket to the lower border of the mandible. A posteroanterior (PA) view of the mandible was taken and a displaced fracture angle was diagnosed. An open reduction and fixation was planned at the superior border. A 4-hole miniplate with monocortical screws was fixed after a reduction of the fracture intraorally under general anesthesia. Postoperative recovery was uneventful without any complication after 8 months of follow-up.
Case 2
A 32-year-old young male patient reported with a chief complaint of pain in his right lower third molar after recurrent pericoronitis. On intraoral examination, his lower right third molar tooth partially erupted, with swelling of the overlying soft tissue. An OPG was advised, which showed a vertically impacted third molar with a distal pocket. A surgical extraction with osteotomy and luxation of the tooth with elevator under local anesthesia was done by a senior resident. After thorough irrigation with normal saline, suturing was done, and the patient was discharged after prescribing anti-inflammatory medication and antibiotics for 5 days. On the 15th day, the patient complained of swelling on his right angle region, severe pain while chewing, and a history of some crackling sound at the back of the mouth one day while chewing. On examination, there was tenderness in the right angle region. The mouth opening was reduced and a slight mobility of fragment distal to the second molar was felt on bimanual palpation. An OPG showed an undisplaced right angle fracture. An MMF was done with ivy’s eyelet wiring for 3 weeks. Recovery was uneventful after 3 months of follow-up.
Case 3
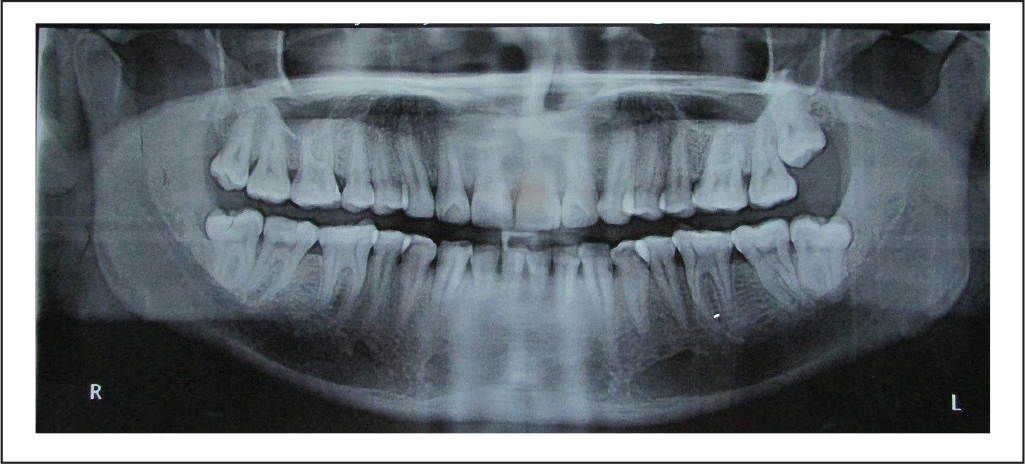
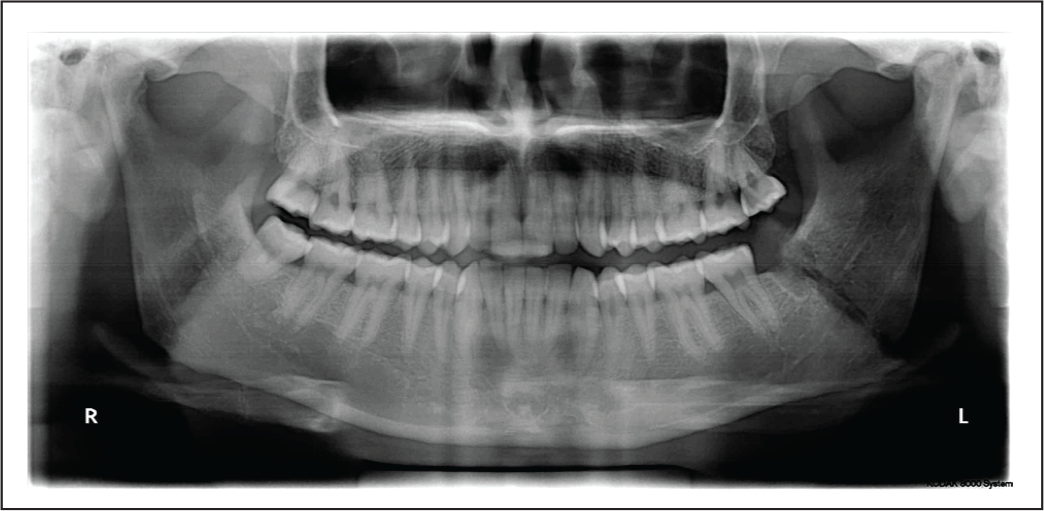
A 42-year-old army soldier was referred by his dentist for extraction of his lower right third molar because of caries in the second molar. His plan was to do a root canal treatment in the second molar and preparation of the crown. An OPG was taken and surgical extraction of a distoangular impacted third molar was done after an osteotomy on the buccal and distal side and a luxation of the tooth with elevator under local anesthesia (Figure 1). He was discharged after getting a prescription of antibiotics and anti-inflammatory medication. He then started his treatment for the second molar from his dentist. On the 10th day, he reported to our unit with swelling over the right angle region and severe pain after chewing some hard food. On asking, the patient stated that he heard some crackling sound while chewing the previous night. On local examination, there was severe tenderness at the angle region, mouth opening was reduced, and slight mobility was felt distal to the second molar. An OPG was done and a fracture line running from the extraction socket toward the lower border was seen (Figure 2). An MMF was done using Erich arch bar for 4 weeks. Recovery was uneventful (Figure 3).
Pre-extraction Position of Tooth on OPG.
Fracture Line Running From Socket to Lower Border.

Healing of Fracture Site After MMF for 4 Weeks.

Case 4
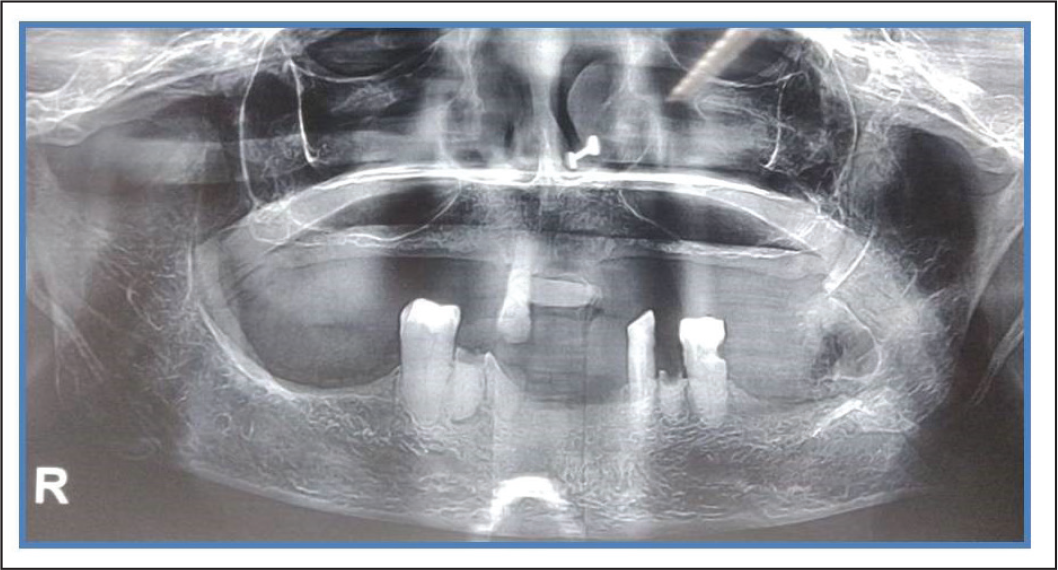
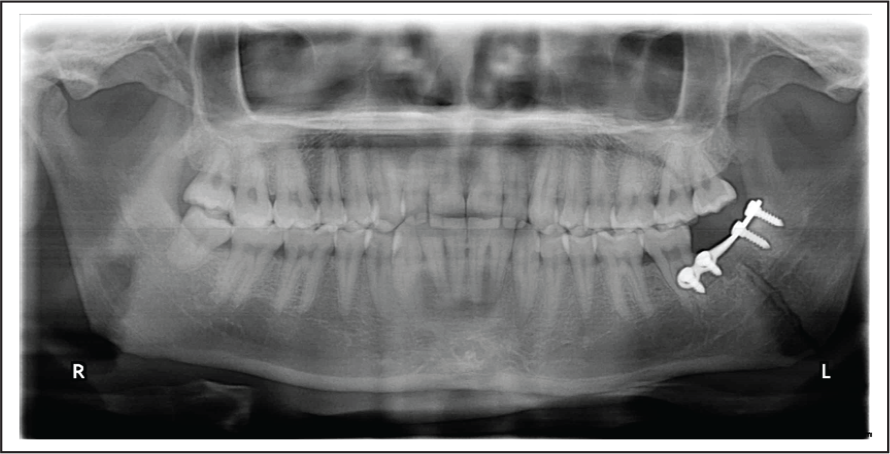
A 24-year-old male patient complained of pain while chewing and painful movements of his lower jaw with a history of surgical extraction of his left mandibular impacted third molar 24 days earlier from an oral surgeon. On clinical examination, there was swelling in the angle region. On palpation, mobility of fragment distal to the second molar was felt. An OPG was taken, which showed a displaced fracture running from the distal to the second molar toward the lower border near the angle region (Figure 4). A treatment plan was discussed with the patient and an open reduction and internal fixation (ORIF) was done intraorally with a single 4-hole miniplate at the superior border. The fracture healed satisfactorily without any relevant complication after the follow-up of 3 months (Figure 5).
Fracture in Extracton Site.
Single 4 Hole Miniplate Used for Fixation Intraorally.
Case 5
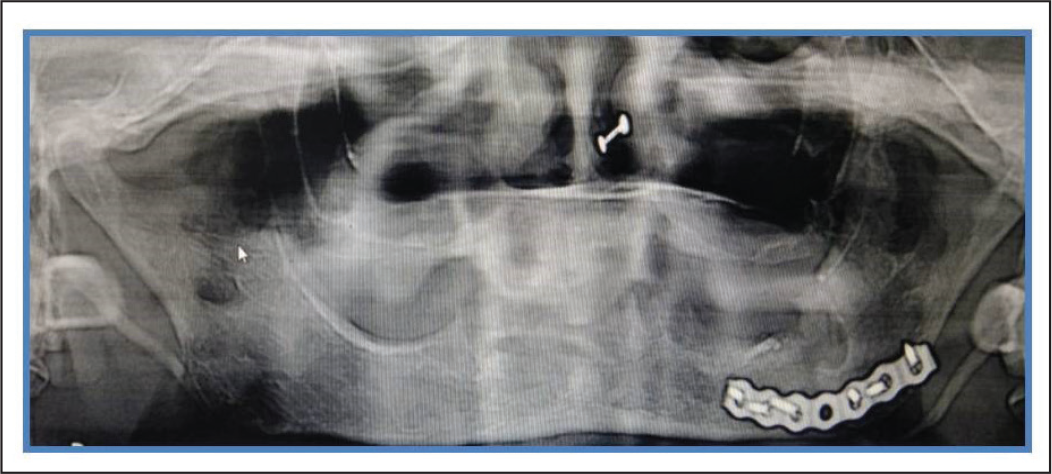
Displaced Fracture After 22 days of Extraction.
Extraoral Exposure and Fixation With Strong Plate.

OPG Showing Reduction After Fixation in Angle Region.
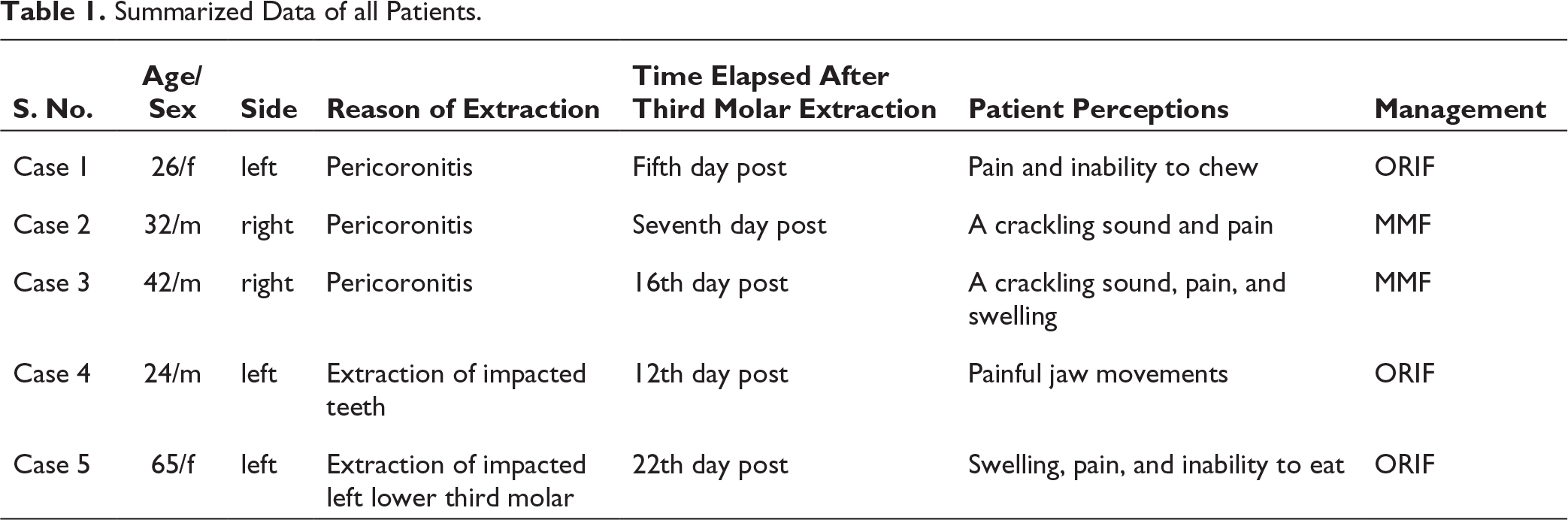
Summarized Data of all Patients.
Discussion
A late mandibular fracture associated with the removal of impacted teeth is an uncommon complication. Nearly 200 cases of late mandible fractures have been reported in the literature published in English and other languages from 1953 to 2019.2, 4 It may occur as an immediate complication during a minor surgery or a late complication within the first 4 to 6 weeks postoperatively. Ethunandan et al, in their study of 130 cases, found that late fractures are more common than intraoperative fractures in the ratio of 2.7:1. Libersa et al reported 37 fractures in 7.50.000 extractions. 6 Perry and Goldenberg 7 also reported only 28 cases in 6,11,000 extractions, and Krimmel et al, in their retrospective study of 917 third molar extractions, reported only 6 cases of late mandible fractures. 8 Prompt treatment is needed to avoid serious complications. The various associated risk factors such as include age, sex, systemic disease, medication, preoperative infection and cystic lesions, type of impaction, surgeon’s experience, and the interrelationship of the third molar to the inferior alveolar nerve should be considered before surgical extraction.2, 4, 7
The age range has been documented in the literature as being from 20 to 80 years, with an average age of >40 years for late fractures.2, 3, 4 But in one study, it was considered that intraoperative fractures are more common in the third and fifth decades of life, and late mandible fractures are more common in the fourth to sixth decades of life. 4 Manclus et al, in their retrospective study of 11 cases, found the mean age of patients to be 42.7 years. 9 According to Perry and Goldberg’s study, the mean age was 39 years. 7 In our case series, 3 of the patients were young, one was middle-aged, and one was an older patient. The reason for fracture in older age may be alterations in bone density, the narrowing of the periodontal ligament, and the presence of systemic diseases or use of drugs. In older individuals, an ankylosed impacted tooth may need more bone removal, further weakening the mandible.8, 9 Young patients with full dentition have more chances of fractures as they can produce more force than patients with partial dentate.
The sex of the patient is also considered to be associated with this complication as its prevalence is more in males as compared to females, as in our cases also where there were 3 male and 2 female patients. The reason for this may be that men are more involved in outdoor activities such as contact supports, have an increased chance of having accidents, or appear to apply greater masticatory force.2, 4, 9, 10
The location, angulation, and position of the molar are considered to be causative factors for this complication; in one of our cases, the first, second, and third molars were deeply impacted near the lower border of the mandible.2, 11 Bony impacted teeth needed more removal of bone associated with increased osteotomy during surgery, result in smaller or weaker strut or cortical shell of bone. 9 According to Pell and Gregory, classification class B/C and position II/III have greater chances of fracture because of extensive bone removal.2, 7 The area of the mandible occupied by the tooth and its tooth-to-jaw ratio accessed from the OPG and CT-scan also play a role. Wagner et al in their 17 case series found that ratio to be 62%, and Iizuka stated that in 13 cases it varied from 44% to 84%. 12 Krimmer and colleagues in their single case reported a ratio of 44% on OPG. 8 Horizontal and vertical impacted teeth are more associated with a fracture of the mandible, as are in our cases as well.2, 7, 9 In another study of 101 cases, the fractures were most common in the mesioangular group (37%) and least common in the distoangular group (12%). 4
The relation of the inferior alveolar canal and molar root is also considered a causative factor. Iizuka et al identified the association between the mandibular fracture and the relation of impacted molar to the inferior alveolar canal because the canal can be identified as an anatomic reference of the meager remnant bone thickness beneath the inferior alveolar nerve canal. 3 A close approximation between the inferior alveolar nerve and the mandibular molar means that a more extensive bone removal may be required. Manclus et al. in 4 late mandible fracture cases revealed that mandibular molar and inferior canal are in juxtaposition to each other. 9
The time interval for fractures is usually between 2 and 4 weeks, but immediate fractures at the time of surgery have also been reported.2, 4, 7, 13 Ethunandan et al in their review noted 43% as intraoperative fractures. 4 Some studies have also reported fractures after 6 weeks of surgical extraction. 12 This also defines the period of transition from granulation tissue to connective tissue in the extraction site; therefore, a heightened risk of fracture is also expected. In addition, patients start using the extraction side for chewing as the discomfort related to surgery has subsided in this period, and a minor trauma to the weakened mandible by being hit with some object may be the cause of a fracture.10, 13 In our cases, all the fractures occurred between the first and third week.
The experience of surgeons was also studied in the literature. Many studies showed that general practitioners and surgeons with less experience have a higher chance of experiencing this complication. In our cases, 1 case was done by a general practitioner and 3 by surgeons with <3 years of experience. This coincides with the results of a study done by Perry and Goldberg 9 in which 4 out of 28 fractures occurred in surgeries that were done by surgeons with <5 years of experience. In another study, in 8 out of 11 cases of late fracture, the mean experience of the surgeons was only 22.9 months with an average of 3 to 48 months. 9 But Sicks and Bonder 2 did not find any significant difference, and they found an increased rate of other complications such as dry socket, swelling, and nerve injuries when the surgery was done by junior residents as compared to senior surgeons. 14 The treatment objective in these cases should be to restore the bony continuity, proper occlusion, and temporomandibular joint functions properly.2, 4, 9, 15 The goal of treatment should be immobilization and fixation after adequate bone reduction. Most of these fractures are not displaced, so MMF for 3 to 4 weeks is sufficient for healing. In our cases, 3 patients were treated with MMF,2, 4 If fracture fragments are displaced, then an ORIF should be done. A miniplate with monocortical screws at external oblique ridge intraorally is the treatment of choice, as was done in one of our cases. 9 If less bone is left or due to osteoporosis we are not able to fix two miniplates, we have to go for regid fixation, as is done in sixth case.
Conclusion and Recommendations
Before the surgical removal of mandibular third molars, factors leading to mandibular fractures should be carefully assessed. Positive factors include men over 40 years of age, having a meager distance between the apex of the socket and the inferior border of the mandible, a period of edentulousness, and any pathology or bone-related systemic conditions that decrease bone strength. The first 2 to 4 weeks are very crucial for the healing of the tooth socket. The patient should be instructed to follow a soft diet and to avoid any accidental contact over the face to avoid this inadvertent complication. In the case of late mandibular fracture, standard management of angle fracture, that is, MMF or ORIF with bone plates. In the end, we recommend that the bone should be preserved and the patient should be warned of late fractures in the high-risk group.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.