
Abstract
Abstract
Introduction: Mandibular angle fracture is a very common fracture of the mandible. These account for approximately 30% of all fractures. These fractures are treated by many techniques such as open reduction or maxilla-mandibular fixation. These fractures have high complication rate accounting for 0% to 32% postoperatively.
Material and Methods: This study was conducted on 50 patient reported in Institute of dental sciences, Bareilly and Rohilkhand medical college and hospital, Bareilly to evaluate the outcome of mandibular angle fracture in our institute.
Result: Out of 50 patients of mandibular angle fracture, 30 were treated surgically, 17 were treated conservatively, and 3 patients were not interested in any kind of treatment. Males are more commonly affected and road traffic accidents was a very common cause of angle fracture.
Introduction
The most common mandibular fracture is mandibular angle fractures (MAFs) which account for about 30% of all mandibular fractures. MAFs may be defined as a fracture line starting in the area where the anterior border of the mandibular ramus meets the body of the mandible, usually in the region of the third molar or distal to third molar. It has been compared to an archery bow, which is the strongest at its center and weakest at the end where it breaks often. MAFs may occur alone or in combination with other facial and skeletal bones. The etiology of mandibular fractures is road traffic accidents, accidental falls, assaults, industrial mishaps, sports injuries, and firearm injuries. 1
The ideal treatment of MAFs is still controversial as these fractures are prone to high complication rates, ranging from 0% to 32%. In the literature, there are various techniques defined for the treatment of MAFs, including close reduction; open reduction with nonrigid fixation by trans-osseous wires, circummandibular wiring technique, or small positional bone plates; AO reconstruction plates; dynamic compression plates; mini dynamic compression plates; lag screws; and noncompression plates. 2
Several investigations with miniplates were performed by Champy et al to validate the technique and to determine the “ideal lines of osteosynthesis” in the mandible where the bone plate should provide the most stable fixation to the bone. On the basis of their experiments and investigations, Champy et al recommended a single noncompression plate fixation at the superior border of the mandible for angle fractures. Since then, many clinical studies have proved the usefulness of this technique. 3
This study was done for the incidence of angle fracture, in the Institute of Dental Sciences, Bareilly, and the treatment options opted for angle fractures. Out of 50 patients with angle fracture, 30 were treated surgically, 17 were treated conservatively, and 3 patients were not interested in any kind of treatment.
Materials and Methods
Patients came in the Outpatient Department of Oral and Maxillofacial Surgery, Institute of Dental Science, Bareilly, and the Casualty Department of Casualty, Rohilkhand Medical College and Hospital, Bareilly.
Inclusion Criteria
Following are the criteria basis which patients were included in the study:
Patients with 15 to 65 years of age. Patients with angle fractures and other associated fractur es in the mandible. Patients in fairly good health (American Society of Anesthesiologists-I [ASA-I] and ASA-II) without any contraindication for surgery or anesthesia.
Exclusion Criteria
Following are the criteria basis which patients were excluded from the study:
Patients with preoperative infection. Patients with medically compromised conditions, preexisting neurologic or musculoskeletal diseases.
Result
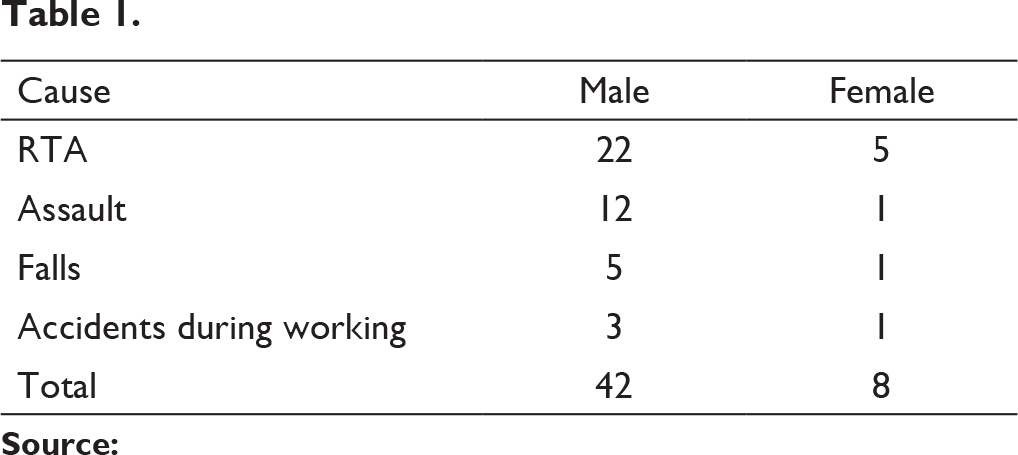
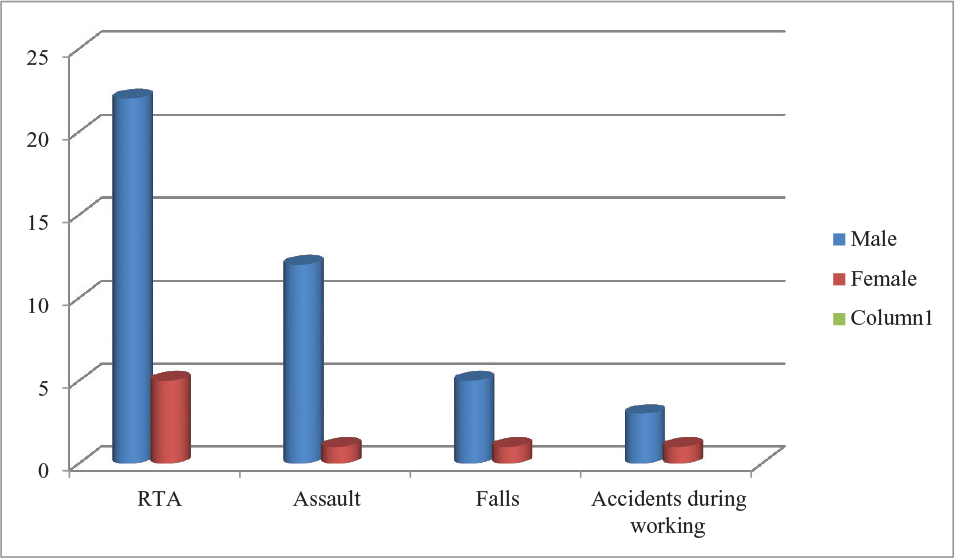
Out of 50 patients, 42 were males and 8 females as shown in figure 1. Most common cause was RTA followed by assault, fall during games, and accident during working as shown in table 1 and figure 2.
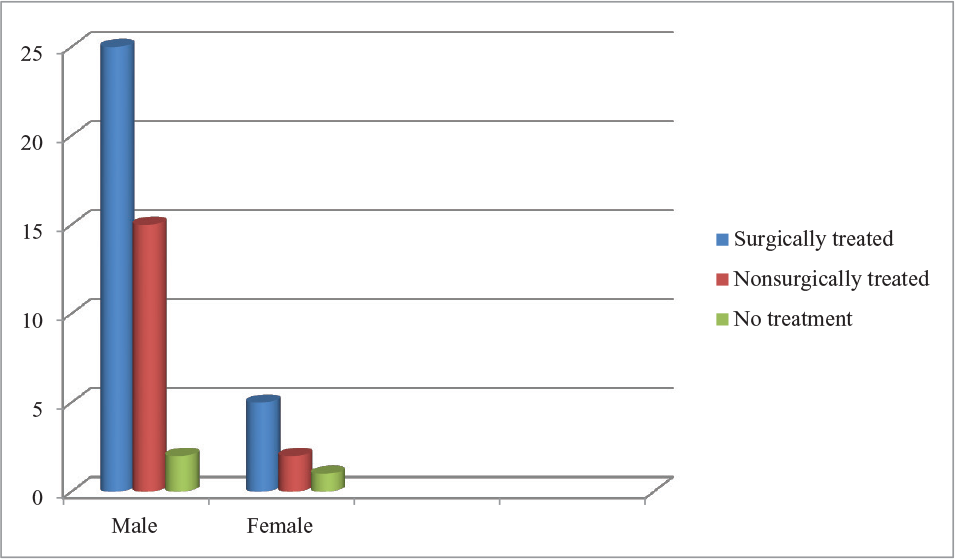
In total number of 50 patients, 30 were treated surgically, these 30 patients were divided into Group A and Group B. Group A was treated with single miniplate at superior border and Group B was treated with two miniplates, one at superior border and another at inferior border of angle of mandible. 17 patients were treated by inter-maxillary fixation for 6 weeks (figure 3 and table 2). In inter-maxillary fixation cases there was poor oral hygiene was recorded with great loss in patients weight on other hand there was good oral hygiene was maintained in patients who were surgically treated and minimum reduction in weight was observed.
Male and Female Patients
Causes of Injury
Causes of Injury
Treatment by Inter-maxillary Fixation
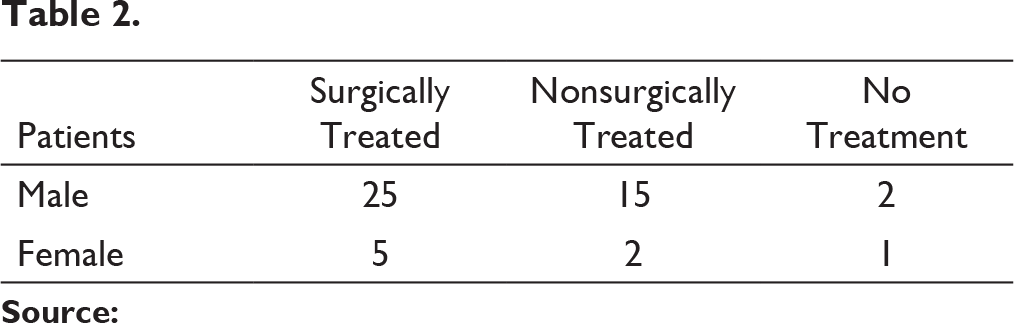
Treatment by Inter-Maxillary Fixation
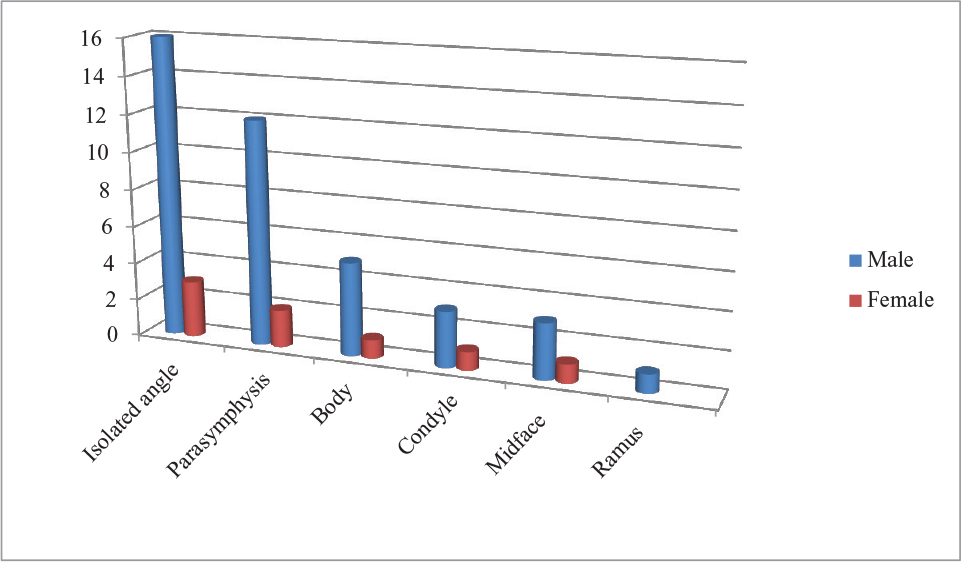
Most Common Associated Fractures
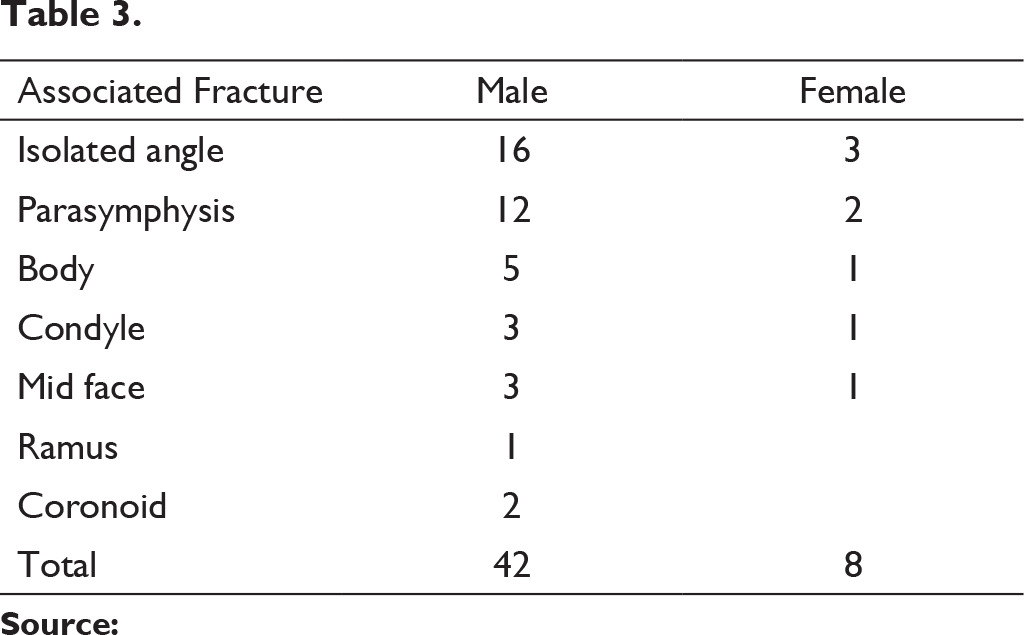
Most Common Associated Fractures
Discussion
MAFs represent 20% of all mandibular fractures in many studies. This outcome was explained by predisposing factors including the presence of third molars and thinner cross-sectional area present at angle when compared with body, symphysis, and parasymphysis regions. 4
One of the greatest shortcomings of most studies on treatment of MAFs is difficult due to unspecific anatomic sites. According to the classic report of Champy et al relating to 183 cases of mandibular fractures, there is almost 3.8% infection rate for all fractures of the mandible. 5
MAFs present with clinical challenge because their treatment is plagued with the highest postoperative complication rate (0%–32%) of all mandibular fractures, as stated by Ellis 6 and Lizuka et al. 7
A controversy, however, exists for the supplementation of miniplate fixation with maxillomandibular fixation 8 : Many surgeons still advice that miniplate fixation does not provide adequate stability and requires maxillomandibular fixation for additional security. In a retrospective study of 287 patients with 499 mandible fractures, Valentino and Marentette 9 compared 130 patients who underwent intraoral monocortical plating of MAFs and found that addition of maxillomandibular fixation does not significantly alter the complication rate. Prein et al 10 reported almost similar findings in their small prospective study of 32 patients combining the old AO technique with maxillomandibular fixation. The stability of single miniplate fixation for angle fractures was challenged by several authors and research studies based on 3-dimensional models. Kroon et al 11 and Choi et al 3 both reported with bony gaps at the inferior border of fracture, and this gap between fracture segments was thought to contribute to subsequent complications which include infection. A second plate was suggested to reduce anterior-posterior separation of the fracture segments as well as lateral displacement of bone, which can be frequently observed on postoperative radiographs. 12 Ensuing clinical studies were inconsistent, with an additional miniplate lowering, increasing, or not changing complication rates.13, 14 More recently, 3-dimensional-model studies have suggested that the torsional and rotational forces at the angle region are relatively weak. 15
Conclusion
According to this study, cases related to males were more common than females, and the most common etiology was road traffic accidents. Patients were more satisfied with surgical treatment. There were more periodontal complications present in respect to conservative treatment, while more paresthesia was recorded in surgical treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.