
Abstract
The treatment of maxillofacial fractures can be done either by closed reduction or open reduction techniques. Pediatric fractures are usually managed by the relatively conservative closed method of treatment. Open reduction and internal fixation (ORIF) is usually reserved for severely displaced fractures difficult to manage conservatively. The ORIF using miniplates are technically challenging and have a negative impact on growth because of surgical trauma. The purpose of this article is to present a case successfully managed by the skeletal suspension technique.
Introduction
Injuries involving the maxillofacial region are quite common in pediatric patients. The management of fractures in pediatric patients presents a unique challenge to maxillofacial surgeons. The management of dental and facial fractures in children requires careful attention to the stage of development of the maxillofacial region. The routine method of management to reconstruct the fractured skeleton must be modified based on its effects on future growth and development. 1 We are presenting a case of maxillofacial fracture in a child patient managed by skeletal suspension wiring, with due attention to the growth and developmental stage.
Case Report
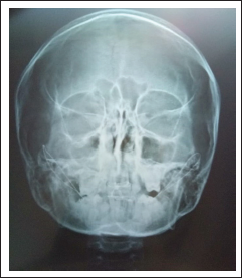
A child patient reported to the Department of Oral and Maxillofacial Surgery with the chief complaint of severe pain in their upper lip and upper jaw because of trauma. There was a history of trauma over the facial region because of the impact of a tyre which suddenly burst while filling air into it. There was no history of loss of consciousness, dizziness, seizure, nausea, or vomiting. On extraoral examination, there was a large laceration involving the right upper lip extending to the left side. The laceration was quite deep, leading to almost splitting of the upper lip (Figure 1). There was severe pain on palpation of the upper jaw. On intraoral examination, the occlusion was disturbed, and there was extensive laceration of palatal mucosa. On intraoral palpation, there was pain in relation to the upper jaw bilaterally. The maxilla was mobile with reference to pyriform aperture. The patient was advised to undergo routine preoperative blood investigations and a CT scan of the face. The radiographic examination revealed a break in the continuity of the maxilla bilaterally and comminution of the palate (Figure 2). Based on clinical and radiographic findings, diagnosis of Lefort-I fracture of the right maxilla and comminuted dentoalveolar fracture of the left side of the maxilla along with comminuted palatal fracture was made. Tentative suturing of the upper lip laceration was done under antibiotic coverage, and definitive management was done later on. The patient was operated on the next day under general anesthesia. The upper lip was re-sutured in layer-wise fashion after ruling out parotid duct injury (Figure 3). The palatal mucosa suturing was done followed by the maxillo-mandibular fixation (MMF) using the Ivy-Eyelet method of wiring. The fractured maxilla was suspended to the stable skeletal units by using the circum-zygomatic method of wiring bilaterally (Figure 4). The patient was examined regularly after a week’s interval. The sutures were removed after 7 days, after ensuring adequate healing (Figure 5). MMF and bilateral circum-zygomatic wires were removed after 3 weeks, after ensuring adequate healing and stability of fractured bones.
Preoperative Photograph Showing Deep Lacerated Wound Involving Upper Lip.

Preoperative CT-Scan Showing Fractured Maxilla.

Upper Lip Primary Closure.

Postoperative Radiograph Showing Bilateral Circum-Zygomatic Wiring.
Postoperative Photograph Showing Healed Upper Lip.

Discussion
The general principles of fracture management are recognition of fracture, alignment of fractured bones (reduction), and its stabilization and fixation. The management of dental and facial fractures in children requires careful attention to the stage of development of the maxillofacial region. The routine method of management to reconstruct the fractured skeleton must be modified based on its effects on future growth and development. Occasionally, confusion may arise while deciding the best method of fracture treatment in growing patients. The physiological functional stresses are essential for the growth of jaws. Although MMF immobilizes the jaws, the effects are quite reversible after removal of MMF and start of functioning. 2 Bone healing takes place quite fast in children because of high osteogenic potential, and thus minimizes the immobilization period. 3 We kept MMF for 3 weeks and there was adequate fracture healing during this period.
ORIF seems to be quite tempting an option as it may eliminate or reduce immobilization period. 4 However, this leads to surgical trauma to the growing skeleton. It invariably requires disruption of the periosteum and soft tissue for the placement of screws and plates. 5 In addition to this, ORIF requires careful attention to the position of developing permanent tooth buds. 6 The ORIF should be done by considering the risk–benefit ratio. In our case, we have done skeletal suspension wiring so as to avoid any drawbacks of ORIF.
Another disadvantage of ORIF using metallic plates is growth restriction and translocation if applied to a growing skeleton. 7 Bio-resorbable plates can be a solution for these problems as they get resorbed on their own over a period of time. We have not used these plates because of high cost and financial constraints. Although skeletal suspension wiring is an old technique, it still has an important role to play.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.