
Abstract
Abstract
Introduction: Among condylar fractures, surgical treatment is most commonly done for subcondylar fractures. Although 2 plate system is most commonly recommended, specially designed delta plate or trapezoidal condylar single 3-dimensional plate have been found to provide early functional rehabilitation with similar stability. Though studied in vitro, not much in vivo study has been done in clinical scenario.
Aim and Objectives: Comparative assessment of functional and radiographic outcomes of patients who underwent subcondylar fracture fixation with trapezoidal and delta condylar plate.
Methods: 20 patients presenting with subcondylar fracture requiring open reduction and internal fixation were included in this 2-year study from 2014 to 2016. Patients were randomly assigned to either one of the groups, with 10 being treated by each plate. Patients were evaluated regularly during 3 months follow-up on clinical parameters, such as occlusion, mouth opening, range of jaw movements, and radiologic parameters, such as fracture alignment, plate fracture, plate bending, screw loosening, secondary displacement of condylar fragment and its direction, ramus height, and any deviation.
Results: In both groups, statistically significant improvement in occlusion seen from the third day to the third month (P value = .04). Postoperative mouth opening, right and left lateral movements, and protrusive movements were statistically nonsignificant in both group A and group B. But within a group, improvements in the results were variable with regard to all these parameters at different intervals. Clinical and radiographic complications were nonsignificant in both group A and group B.
Conclusion: This study is a preliminary effort to evaluate and compare different special plating systems in the management of condylar fractures with the new 3-dimensional trapezoidal and delta plating system, which gives excellent stability and rigidity.
Improvement in occlusion was found to be gradual in both the plating system over a period of 3 months. Delta plate showed significant improvement in mouth opening at all intervals in comparison to Trapezoidal plate. Improvement in protrusive movement was found to be gradual and better with delta plate. A trapezoidal condylar plate holds goods for low subcondylar fractures owing to its wider dimension, though delta plate is versatile for both high and low subcondylar fracture.
Keywords
Introduction
Initially proposed adaptation of single 4 hole miniplate did not provide dynamic osteosynthesis and resulted in fracture of the plate during function.1-3 As an alternative to the modified 2-miniplate technique, specially designed delta plate or trapezoidal condylar plates have been found to provide early functional rehabilitation with its 3-dimensional (3D) stability. Aim of this prospective study is to evaluate the role of especially designed 3D delta and trapezoidal condylar plates (individually and comparatively) in the management of mandibular subcondylar fractures. Though studied in vitro, not much in vivo study has been done in clinical scenario.
Material and Methods
A prospective study was undertaken comparing the results of patients who underwent open reduction and internal fixation of subcondylar fracture with delta and trapezoidal condylar plates in 20 randomly selected patients reporting to the Department of Oral and Maxillofacial Surgery of Punjab Government Dental College and Hospital, Amritsar, from 2014 to 2016. 20 patients with subcondylar fracture associated with or without fracture of other parts of mandible were selected at random irrespective of age, sex, caste, creed, and socioeconomic status.
Inclusion Criteria
Patients of age 15 years or more, who agreed to give consent for this study, were included in this study. Patient with Unilateral mandibular subcondylar fracture with or without associated mandibular fractures at other sites.
Exclusion Criteria
Patients with Bilateral condylar fractures in which either of the condyle were treated conservatively. Patients under 15 years of age, medically compromised patients who were not fit for surgery, and patients who did not give consent for this study were excluded.
Method
Patients were randomly divided into 2 groups. The patients had to give written informed consent for participation in this study. Patients were informed regarding the need for 3 months follow-up. The ethical clearance for conducting the study was obtained from the ethical committee of the institution.
Group A consisted of 10 patients, who were managed by using orthomax trapezoidal condylar plate that was 1.0 mm thick, 10 mm wide at the top, 16 mm wide at base, and 17 mm long (Orthomax, India). 2 holes form the 2 corners of upper arm and two more holes form the 2 corners of lower arm (Figures 1–4). Group B consisted of 10 patients, who were managed by using orthomax titanium delta-shaped condylar plate 1.0 mm thick, 20 mm long, 5 mm wide at top, and 14 mm wide at the base. At the top of the plate is an arm with 2 longitudinally arranged holes; two more holes form the 2 corners of the base of the plate (Figures 5–8). A 2 mm or 2.5 mm orthomax titanium miniplate was associated with fractures of mandible. Unilateral mandibular subcondylar fracture with or without associated mandibular fractures at other sites.
Trapezoidal Condylar Plate

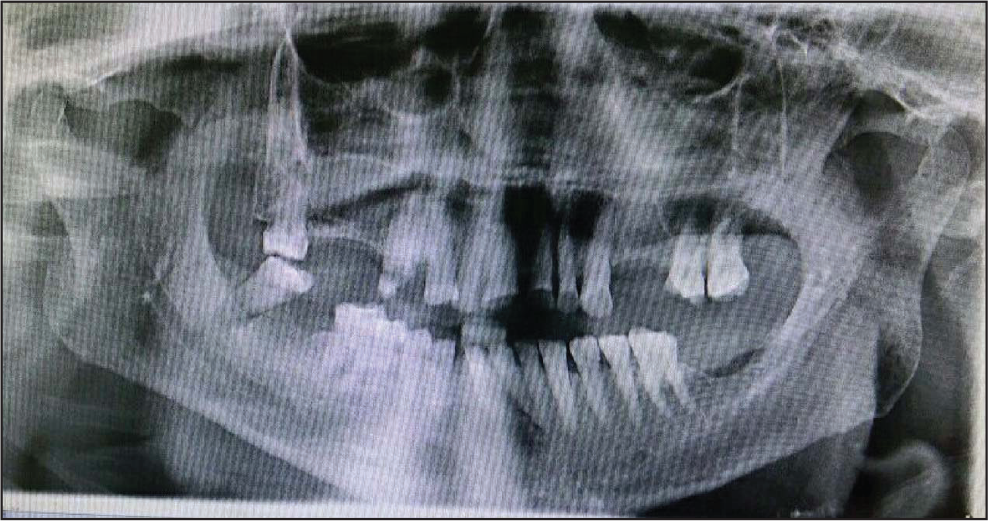
Preoperative Orthopantomogram (Group A)
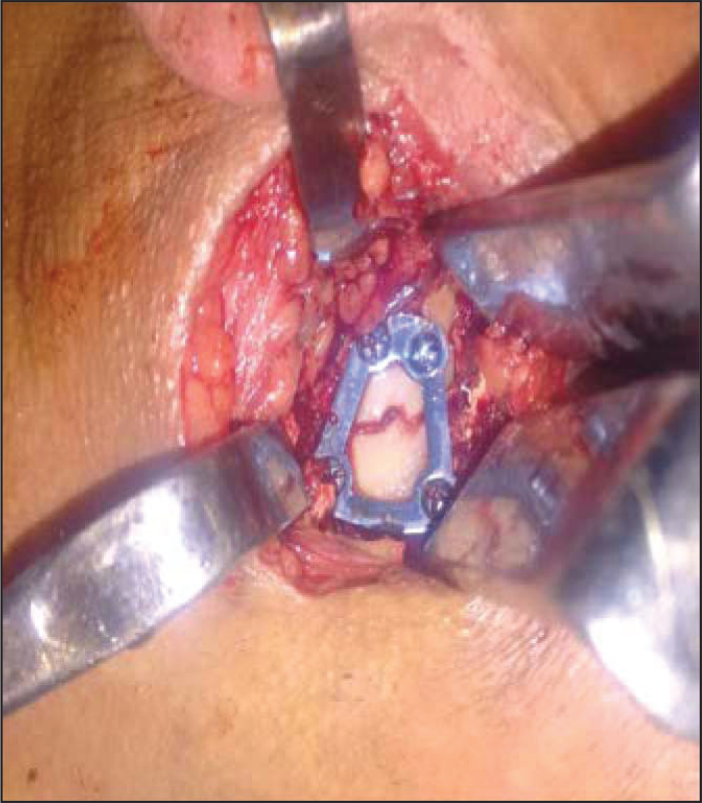
Open Reduction and Internal Fixation of Subcondylar Fracture With Trapezoidal Condylar Plate (Group A Patient)
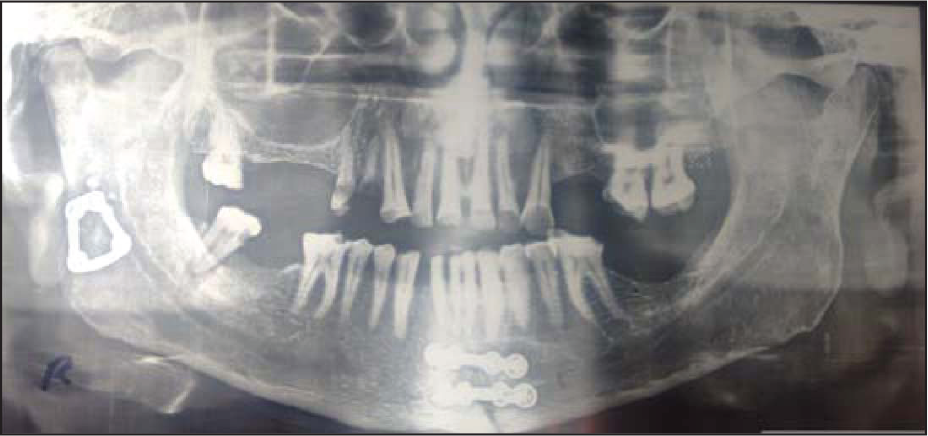
Orthopantomogram Taken on Third Month (Group A Patient)
Delta Condylar Plate

Preoperative Orthopantomogram (Group B)
Open Reduction and Internal Fixation of Subcondylar Fracture With Delta Condylar Plate (Group B Patient)

Orthopantomogram Taken on Third Month (Group B Patient)

Functional Parameters for Clinical Evaluation
Evaluation of Complications Encountered (If Any)
Radiographic Parameters for Evaluation
Results
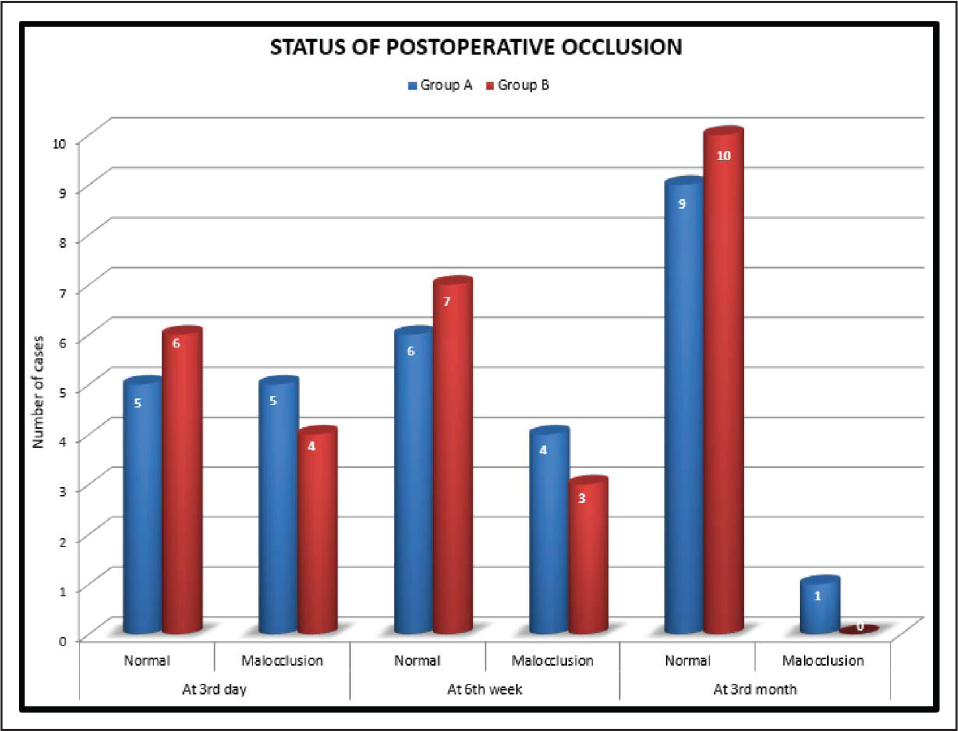
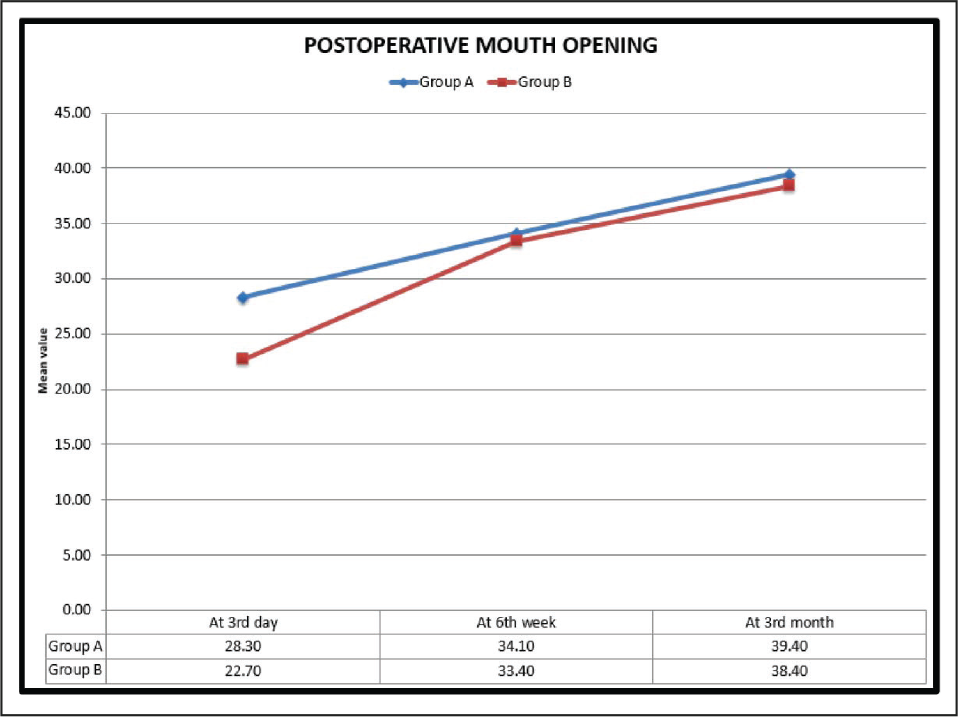
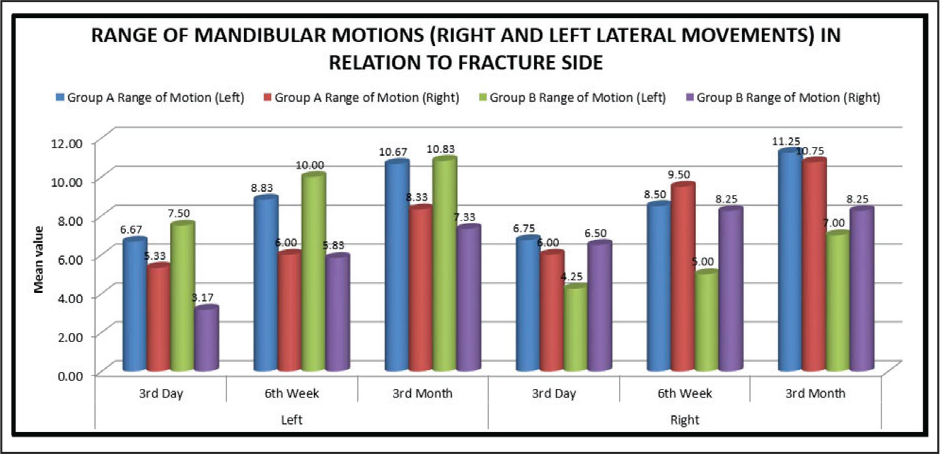
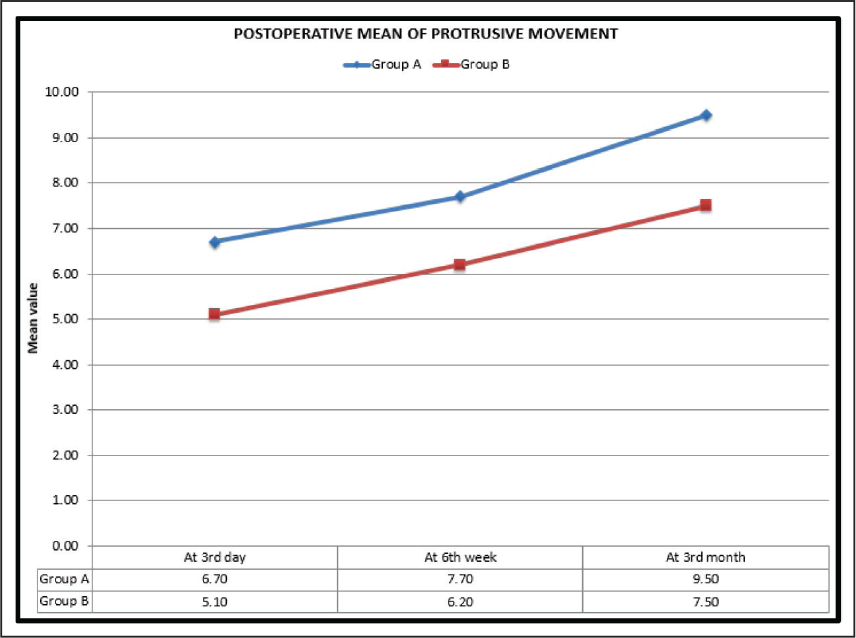
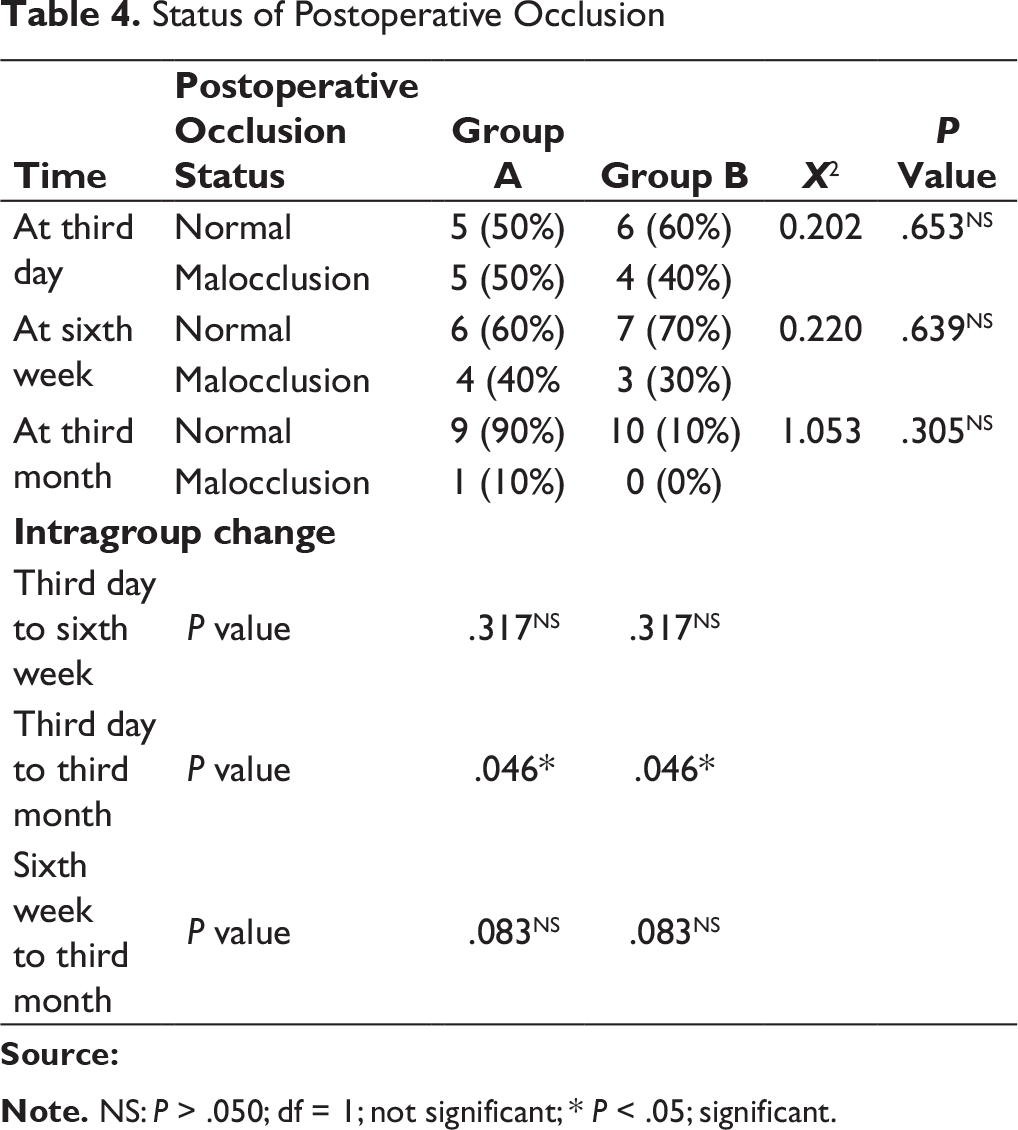
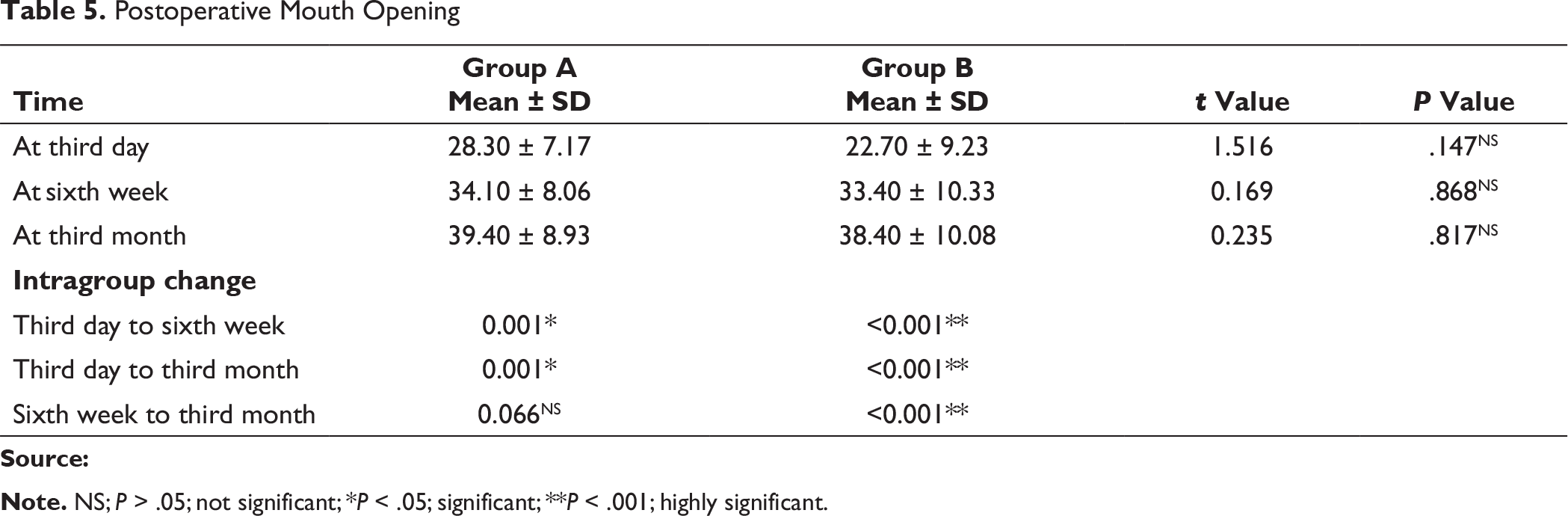
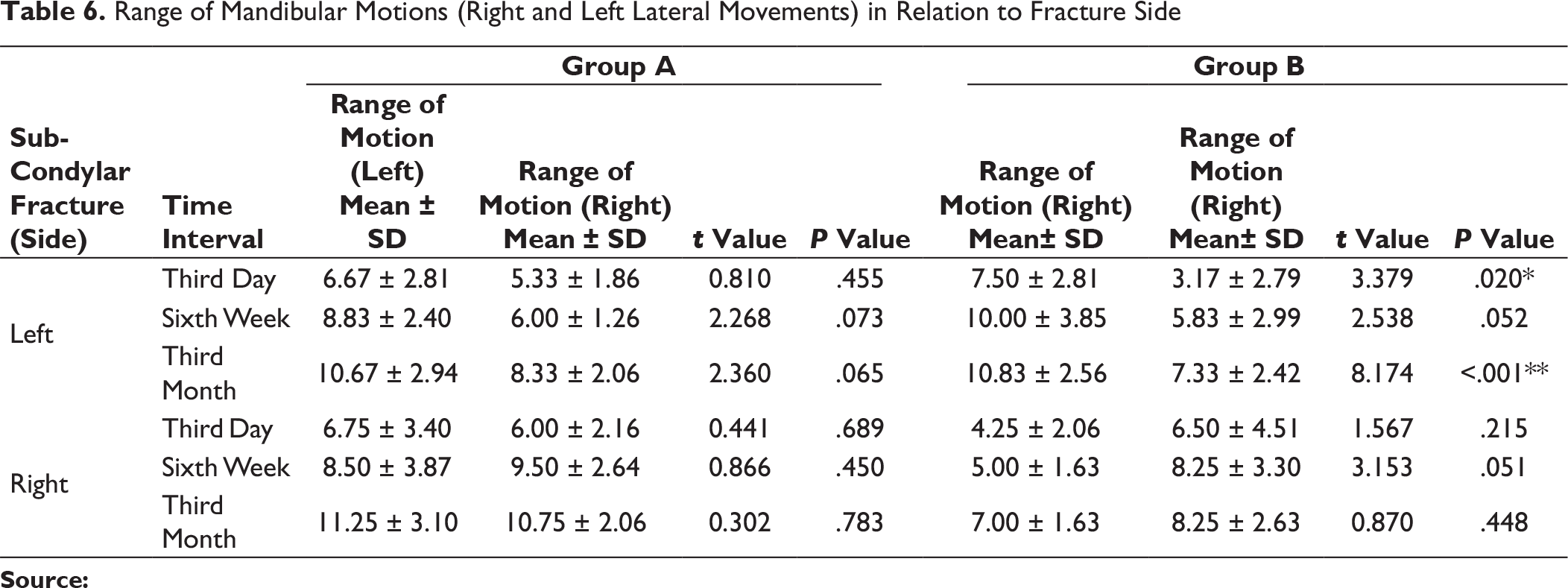
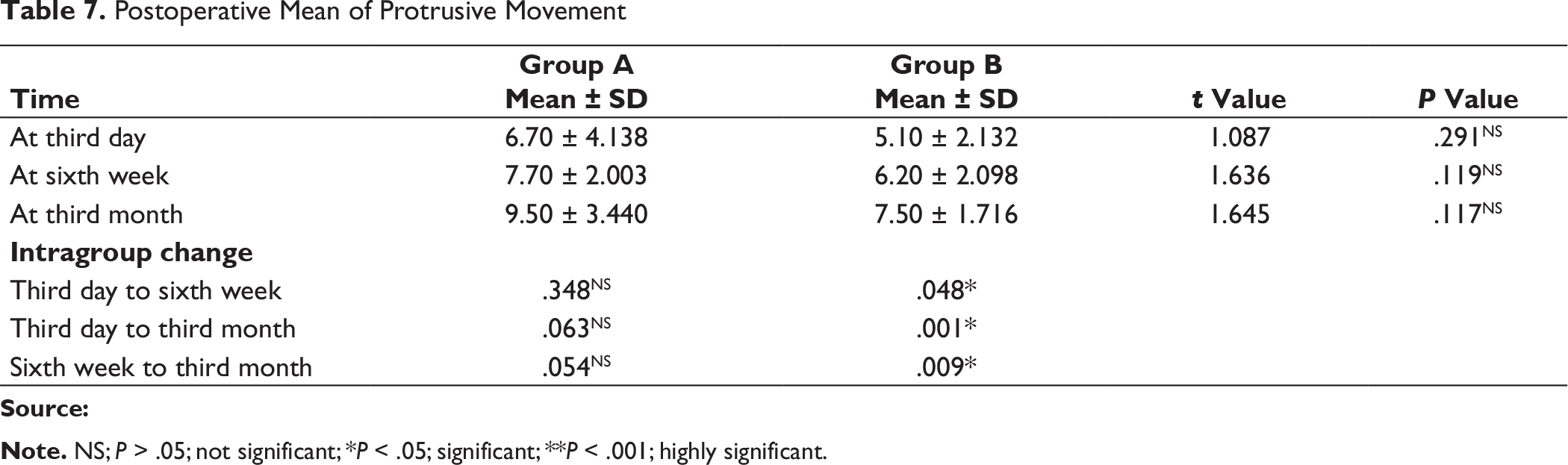
In this study, the number of male patients was higher, ie, 15 (75%), than the number of female patients. The major etiological factors in our study were road traffic accident (50%), followed by interpersonal fight (35%), and fall (10%). We found that the most common age group of patients affected with trauma was between 15 and 25 years (30%). Left subcondylar fracture was predominant (60%) in this study with most commonly associated fracture being right parasymphysis fracture (40%), fracture symphysis (20.0%). Postoperatively at 72 hours and at 6 weeks both groups had transient malocclusion. At the end of the third month postoperatively, all patients had satisfactory occlusion in both the groups except 1 patient (10%) in group A, who had dislocated condyle postoperatively (Table 4). In group A and group B, improvement in occlusion was statistically insignificant from the third day to the sixth week, and sixth weeks to third month (P value > .05), but statistically significant improvement in occlusion seen from third day to third month; Figure 9). Patients treated with delta plate showed significant improvement at all intervals in comparison to trapezoidal plate, which did not show significant improvement in mouth opening from six weeks to third month (Table 5 and Figure 10). In group A, for both left side and right side subcondylar fractures and in group B for right side subcondylar fracture improvement in right and left lateral movements were similar. In group B, movements toward right side were less as compared to left side in case of left side subcondylar fractures statistically significant on the third day and statistically highly significant on the third month (Table 6 and Figure 11). In group A, there was statistically no significant increase in the protrusive movement from the third day to six weeks (P value = .348), third day to third month (P value = .063) and six weeks to third month (P value = .054). In group B, there was statistically no significant increase in protrusive movement from the third day to six weeks (P value = .048) and highly statistically significant increase in protrusive movement third day to third month (P value = .001) and six weeks to third month (P value = .009), ie, initially there was no improvement; improvement in protrusion was noted late during follow-up and overall over a 3-month period (Table 7 and Figure 12). Improvement in protrusive movement was found to be gradual and better with delta plate while not much significant improvement was seen with trapezoidal condylar plate.
Comparison of Postoperative Occlusion at Different Intervals in Group A and Group B
Comparison of Mouth Opening at Different Intervals in Group A and Group B
Comparison of Range of Mandibular Motions (Right and Left Lateral) in Relation to Fracture Side in Group A and Group B
Comparison of Range of Mandibular Protrusive Motions at Different Interval in Group A and Group B
Status of Postoperative Occlusion
Postoperative Mouth Opening
Range of Mandibular Motions (Right and Left Lateral Movements) in Relation to Fracture Side
Postoperative Mean of Protrusive Movement
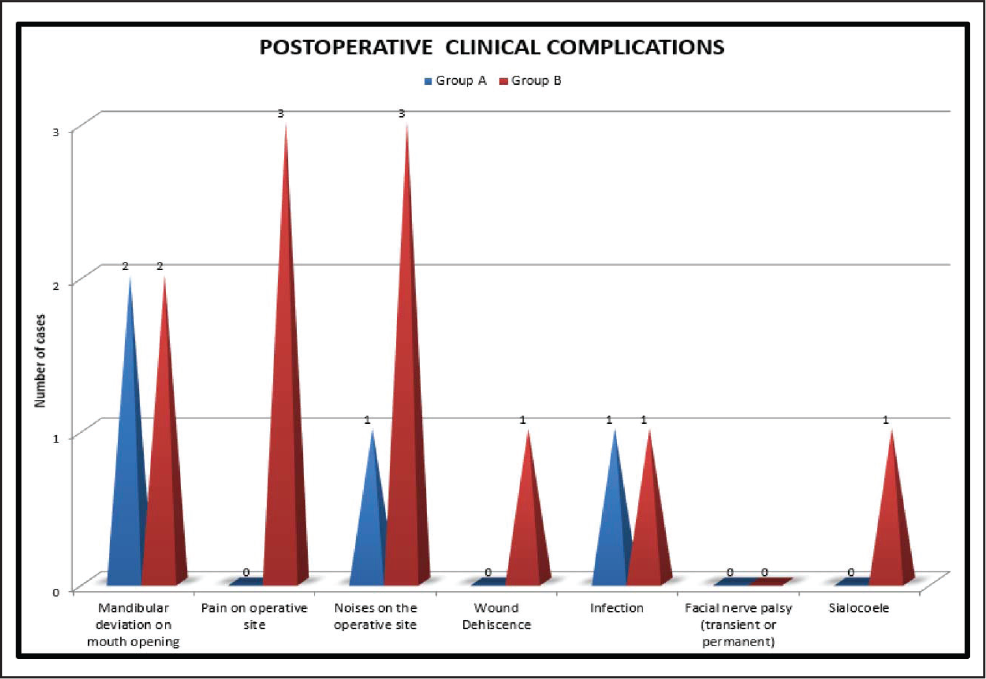
Deviation toward fractured side on mouth opening was present in 2 patients (20%) of both group A and group B. Noises at operated joints were present in 1 patient (10%) in group A and 3 patients (30%) in group B. In group A, no patient had pain on the operated joint at third month, but in group B, 3 patients (30%) had pain at joint on operated side. The difference in pain in two groups was found out to be statistically nonsignificant (P value = .06). We did not encounter any facial nerve palsy (transient or permanent) in any of our cases in both the study groups. Wound dehiscence along with infection was noticed in group B in one patient while in group A one patient had only stitch abscess. Sialocele was noticed in group B in 1 patient. 1 patient in group B had temporary paresthesia of ear lobule (greater auricular nerve) (Figure 7).
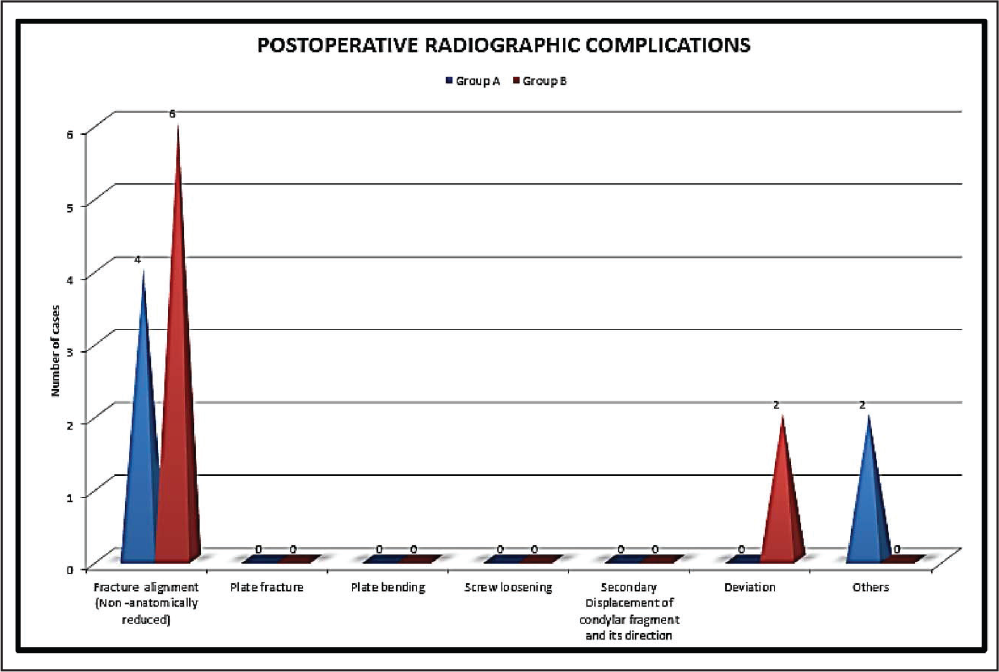
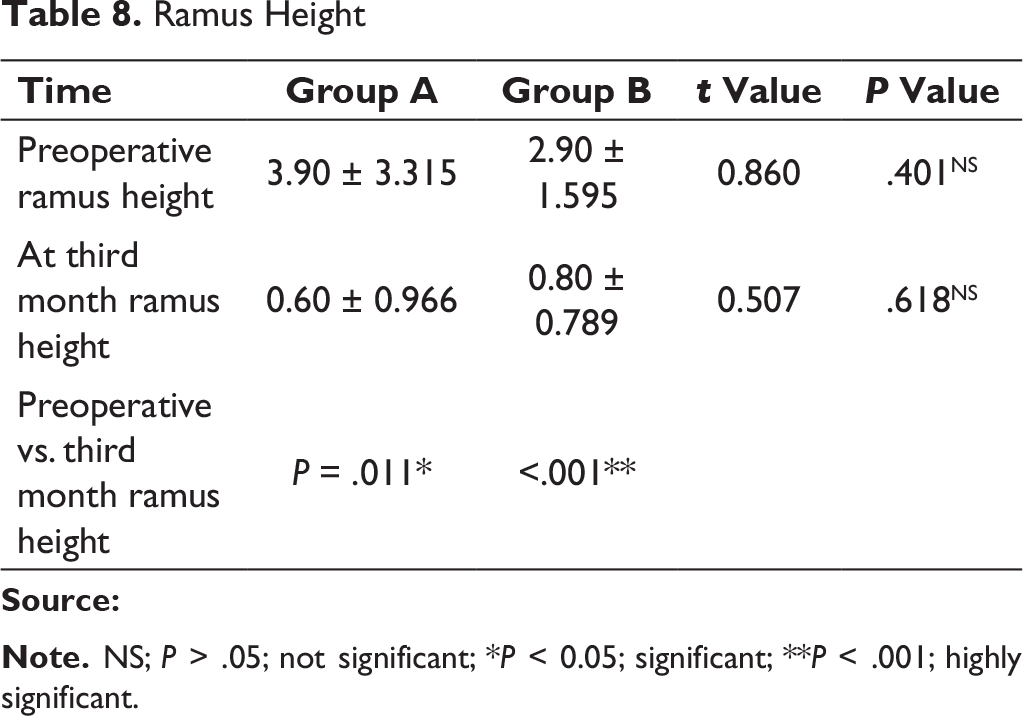
At the X-ray follow-up on the third postoperative day, ideal anatomical reduction was achieved in 6 patients (60%) in group A, and in group B, 4 patients (40%). Plate fracture, plate bending, screw loosening, and secondary displacement any of these complications were not encountered in our study. Radiographic deviation was not noted in group A, while 2 patients (20%) in a group B showed radiographic deviation which was found out to be statistically nonsignificant. The mean difference in posterior facial height between the fractured and nonfractured side preoperatively in group A was 3.90 mm and in group B was 2.90 mm, and postoperatively at the third month, the mean difference was found in a group A was 0.60 mm and that in group B was 0.80 mm (Figure 13). This difference was found out to be statistically nonsignificant in both the groups. P value for preoperative ramus height and third month ramus height in group A was .11 which is statistically significant and in group B was < .001 which is statistically highly significant (Table 8). The difference in ramus height was found out to be statistically nonsignificant in both the groups, ie, ramus height restored well with both plates.
Comparison of Clinical Complication Observed in Both the Groups
Comparison of Radiographic Complication Observed in Both the Groups
Ramus Height
Discussion
Two miniplates (double-plate technique) are considered to be most reliable because they neutralize tension and pressure forces best and produce greater stability in condylar fractures,4, 5 but fixation with two miniplates might be a more traumatic procedure than fixation with a single miniplate. This disadvantage was overcome by the decision of Meyer et al 6 to select a different design of trapezoidal- or delta-shaped plates, having taking into account the anatomical circumstances. 3D plates respect the principles of functionally stable osteosynthesis, and secondly, take advantage of the 3D characteristic of the plate, enhanced stability, less periosteal dissection, and possible osteosynthesis of small fragments 7 combined with the advantages of a smaller plate size and greater stiffness. 8
Although studied in vitro, not much in vivo study has been done on this in clinical scenario. The present study is one of the first that helps do in vivo comparison of both delta and trapezoidal condylar plate and assess functional and radiographic outcomes of patient who underwent subcondylar fracture fixation with trapezoidal and delta condylar plates.
Because of institutional restriction, infrastructure and not commonly available facility of general anesthesia, most of the cases (75%) were handled under local anesthesia. The retromandibular transparotid approach was found to be comfortable when undertaken with local anesthesia, as it offers the advantage of adequate exposure, and easy access for the reduction of displaced condylar fractures results in acceptable aesthetic outcomes as it does not involve any supplemental incision.
When comparing the handling properties of both the plates, it was found that delta plate was much easier to manage. We found trapezoidal condylar plate more suitable for low subcondylar fracture owing to its wider dimensions, and that delta plate is versatile in its use for both high and low subcondylar fractures. This was in accordance with Sikora et al. 9
In regard to occlusion, our results exhibited transient postoperative malocclusion; which were in accordance with Lauer et al 10 exhibited transient postoperative malocclusion, which disappeared after 2 to 5 weeks of functional therapy with elastics. The persistence of impaired dental occlusion appeared to be primarily associated with imperfect initial reduction (50%) and the occurrence of secondary displacement (25%). 6 However, in our study no such correlation is seen.
Mean mouth opening, right and left lateral and protrusive mandibular movements were found to be statistically nonsignificant between both the groups, but improvement is seen in both the groups at different time intervals. Our results regarding restoration of correct mandibular motions were in accordance with Meyer et al, 6 Sikora et al, 9 and Lauer et al. 10
Clinical Complications
Deviation was seen in in 2 patients (20%) of each group A and group B. These patients were advised physiotherapy. Our results are in accordance with those of Lauer et al, 10 who reported a slight lateral deviation on mouth opening to the fractured in 7 of the 16 patients with the use of delta plate in condylar neck fractures. Meyer et al 6 reported asymmetric movements in 5% patients and correlated it to contralateral unoperated head fractures (2 patients) and/or to poor initial reduction (2 patients). In our study, in group B, nonanatomical reduction was seen on the third day in these 2 patients, which probably may be the reason for deviation, but no such correlation was seen in group A as both subcondylar fractures were anatomically reduced.
In group A, no patient had pain in the operated joint in the third month, but in group B, 3 patients (30%) had pain in the joint on the operated side. 2 out of these 3 patients had pain in the sixth week. 1 patient who had pain at operated site in the third month had pain and pus discharge from ear. This patient was referred to an otorhinolaryngologist where he is still continuing with his treatment. Patient’s symptoms have been improved markedly but complete resolution of joint pain is not there even after 6 months of follow-up. The difference in pain in 2 groups was found out to be statistically nonsignificant (P value = .060). Earlier, the resolution of pain in our patients can be attributed to better stability of the fragments provided by trapezoidal and delta condylar plates. In contrast to our study, Chaudhary et al 11 and Meyer et al 12 reported that none of their patient had any pain at 3 and 6 months of follow-up, respectively.
Noises at operated joint were present in 1 patient (10%) in group A and 3 patients (30%) in group B. 1 patient in group A had clicking in the third month and 2 patients in group B had clicking sound on palpation, 1 in the sixth week and another in the third month (only subjective). The third patient in group B had both subjective and objective grating sensation on the operated joint in the sixth week and the third month follow-up. This patient had associated ear infection at the third month and hypoacusis. In contrast to our study, Meyer et al 12 reported that no patient complained about articular noises on the operated side sixth month follow-up in their study.
Wound dehiscence with pus discharge is another complication noticed in one of our patients in group B. Pus sample was taken and sent for culture and sensitivity. Patient was managed with drainage, irrigation, and appropriate antibiotics. In group A, postoperatively stitch abscess was present in 1 patient (10%) in the sixth week of follow-up, which was subsequently managed with normal saline irrigation and local antibiotics. This was due to presence of loose suture thread as pus discharge stopped after removing it. No infection was noted at subsequent follow-ups. Meyer et al 6 reported 1 patient to develop a postoperative wound infection that necessitated reoperation for drainage on the 15th day.
However, Hammer, Schier, and Prein 13 reported an infection rate in more than one-third (35%) of the group stabilized with a single adaptation miniplate. Thus, it can be presumed that stability in 3D is important for the prevention of infection, a criterion that both trapezoidal condylar plate and delta plate fulfill. Both plates provide stable osteosynthesis and minimize the rate of hardware failure and hence infection.
We did not encounter any facial nerve palsy (transient or permanent) in any of our cases. Our results were in accordance with those of Croce et al 14 who found none of the patients operated on by a transparotid approach to have this complication.
1 patient in group B had temporary paresthesia of ear lobule (greater auricular nerve). By the end of the third month, he/she had recovered pain sensation and even hyperesthesia of ear lobule was reported. Some branches of greater auricular nerve pass through the parotid gland and gives sensory innervation to the skin of a part of the outer ear (lobule) and a variably wide area in the mandibular angle. 15 This normal anatomical variation of the course of nerve might be the reason for transient paresthesia of great auricular nerve. In parallel with our findings Chossegros et al 16 reported two cases of temporary paresthesia in the distribution of the great auricular nerve which generally resolved within a few weeks. Manisali et al. 17 reported sensory deficit in the distribution of the great auricular nerve in 2 patients, but this recovered after a few weeks.
Sialocele was noticed in 1 patient (10%) in group B on the seventh day and it was aspirated and pressure dressing was done using adhesive dressing on follow-up visit. The patient was also put on antisialogogues and successfully managed within next 3 weeks. No sialocele occurred in group A. To prevent the formation of sialocele water, tight closure of parotidomasseteric fascia was done carefully and pressure dressing was given in rest of the cases in the study.
In the study conducted by Meeran and Selvakumar, 18 1 patient developed sialocele which was managed by compressive dressing and antibiotics, the parotid fascia must be sutured with meticulous care to attain water-tight closure. Manisali et al 17 reported 1 case of sialocele postoperatively following the retromandibular approach which required aspiration on 2 occasions before resolving.
Radiographic evaluation showed that the osteosynthesis is relatively stable. All the patients treated with trapezoidal and delta condylar plating system were functionally stable and well rehabilitated. At the X-ray follow-up on the third postoperative day, ideal anatomical reduction was achieved in 6 patients (60%) in group A, and in group B in 4 patients (40%). Minor deviations from the anatomically correct position have no impact on the function of the temporomandibular joint later. 19 We did not notice any correlation between the malocclusion and nonanatomical reduction of subcondylar fracture.
Plate fracture, plate bending, screw loosening, and secondary displacement are considered signs of either inadequate fracture stabilization or incorrect fracture reduction. We did not encounter any of these complications in our study.
Radiographic deviation was not noted in group A, while 2 patients (20%) in group B showed radiographic deviation, one in the sixth week and another in the third month of follow-up. Stability of delta plate cannot be questioned, since the difference in the incidences of radiographic deviation in both the groups was found out to be statistically nonsignificant.
Manual tracings were done for the evaluation of ramus height as suggested by Undt et al. 20 The results of this study clearly show that surgical reestablishment of vertical ramus height by open reduction and internal fixation of the condylar process fracture results in normal facial symmetry in most patients. Thus, ramus height seems to be restored to normal height in both the groups.
Conclusion
This study is a preliminary effort to evaluate and compare different special plating systems in the management of condylar fractures with the new 3D trapezoidal and delta-plating system, which gives excellent stability and rigidity. The study resulted in the following:
Improvement in occlusion was found to be gradual in both the plating systems over the period of 3 months. Improvement in mouth opening was rapid with trapezoidal condylar plate up to 6 weeks, after which improvement was not significant as seen with delta plate. Improvement in right and left lateral movements were equal with trapezoidal condylar plate irrespective of the side of fracture. Delta plate improvement in lateral movements was variable, ie, less on the right side for left subcondylar fracture. Improvement in protrusive movement was found to be gradual and better with delta plate while not much significant improvement was seen with trapezoidal condylar plate. As complications were found to be more in the group B which were not related to hardware, none of the two plates was found to be superior. Trapezoidal condylar plate holds goods for low subcondylar fracture owing to its wider dimension, though a delta plate is versatile for both high and low subcondylar fractures. It is relevant to comment that both the 3D condylar plates were found to be more economical than 2 miniplates used for condylar fracture reduction. However, a larger number of cases studied over a longer period of time would shed more light on results. More importantly, a multicenter study will help to correlate among these studies to authenticate our claims.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.