
Abstract
The nested subtype of urothelial carcinoma (NS-UC), a rare and aggressive bladder cancer, mimics benign bladder lesions but behaves like high-grade urothelial carcinomas. The author reported a rare case of NS-UC, initially presenting with inguinal lymph node metastasis. The tumor cells of NS-UC exhibit minimal cellular atypia, forming small nests, while the tumor cells of lymph node metastatic carcinoma show greater cellular atypia with diverse structures. Immunohistochemistry is helpful in determining the origin of lymph node metastatic carcinoma. NS-UC often presents morphologically similar to benign lesions, which should be given sufficient attention.
Keywords
Introduction
NS-UC is a uncommon bladder cancer characterized by a bland histomorphology that mimics benign urinary bladder lesions. However, it exhibits clinical behavior similar to high-grade conventional urothelial carcinomas. Studies indicate its association with advanced tumor stage and frequent nodal metastasis, possibly attributed to diagnostic delays. 1 Initially described in 1979 by Stern, 2 NS-UC gained recognition by the WHO only in 2004. The recent 2022 edition of WHO recognized the large and small nested variants as part of the nested subtype of urothelial carcinoma. 3 In this report, we present a case of advanced NS-UC, initially presenting as inguinal lymph node metastasis.
Case Presentation
A 54-year-old woman visited our hospital due to persistent and worsening left abdominal pain. A solid mass in left lower abdomen was identified through ultrasonography. Spiral CT revealed a high likelihood of lymph node metastasis on both sides of the clavicle, with multiple enlarged lymph nodes adjacent to the left iliac artery and retroperitoneum. Additionally, thickening and significant enhancement were observed in the left bladder wall. Next, the right inguinal lymph node biopsy was performed.
Pathologically, the lymph nodes exhibited infiltration and destruction by highly atypical neoplastic cells, arranged in solid, large-nested, small-nested, and single-cell patterns. Tumor cells featured large nuclei of varying sizes, prominent nucleoli, and abundant eosinophilic cytoplasm. Note that the cellular atypia observed within the focal region is of a relatively mild nature (Figure 1). Immunohistochemical staining revealed positive results for Ki67 (70%), P53 (70%, moderately to strongly), CK (AE1/AE3), GATA3, CK7, CK5/6, and p63. Conversely, CK20, Villin, SATB2, PAX8 were negative. Based on histomorphology and immunohistochemical expression, lymph node metastasis was supported, and suspected from bladder urothelial carcinoma (Figure 2).
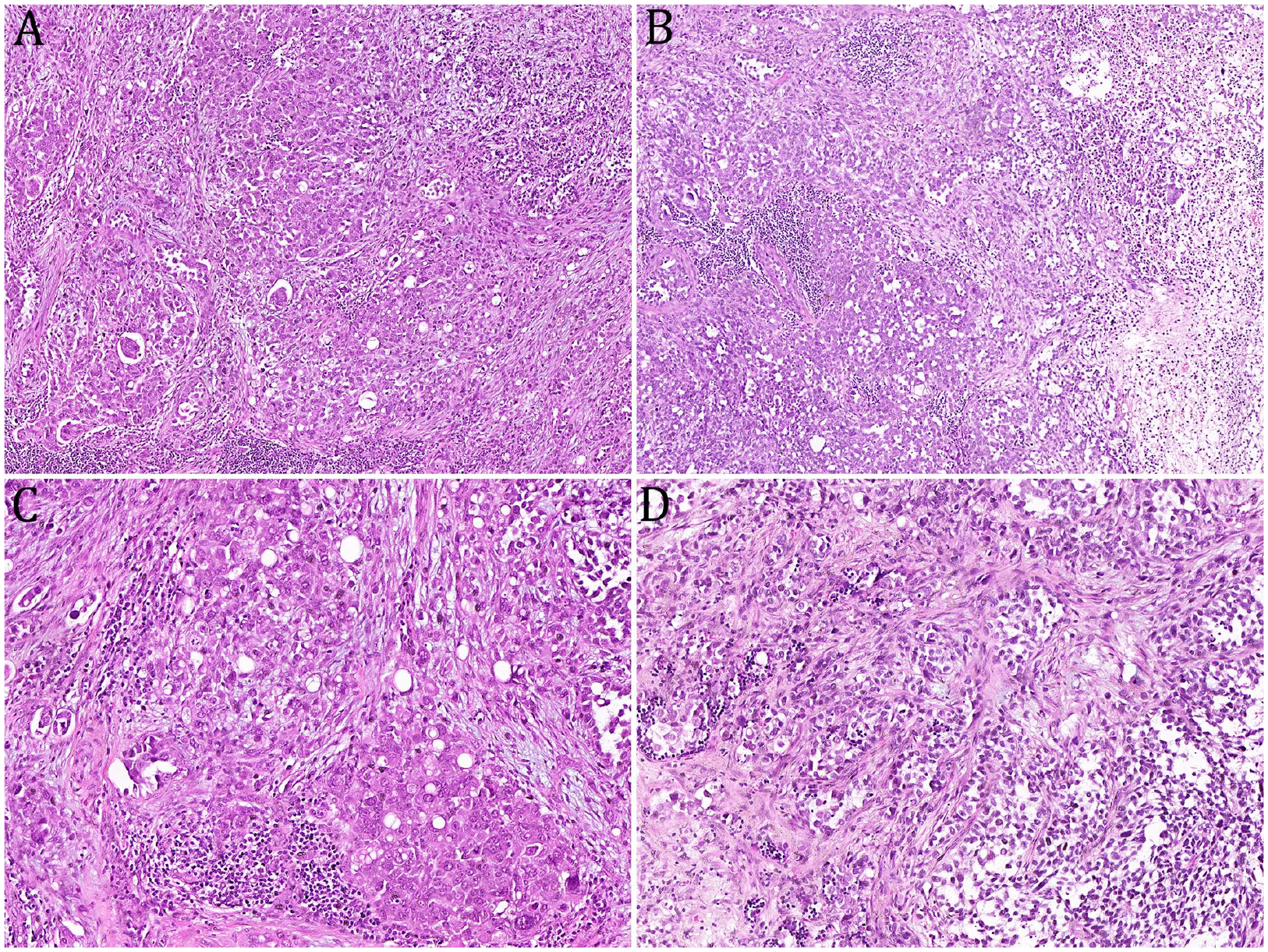
The lymph nodes exhibited infiltration and destruction by highly atypical neoplastic cells, arranged in solid, large-nested, small-nested, and single-cell patterns, accompanied by evident fibrous reaction and focal necrosis (A, B). Tumor cells featured large nuclei of varying sizes, prominent nucleoli, and abundant eosinophilic cytoplasm (C). Note that the cellular atypia observed within the focal region is of a relatively mild nature (D).
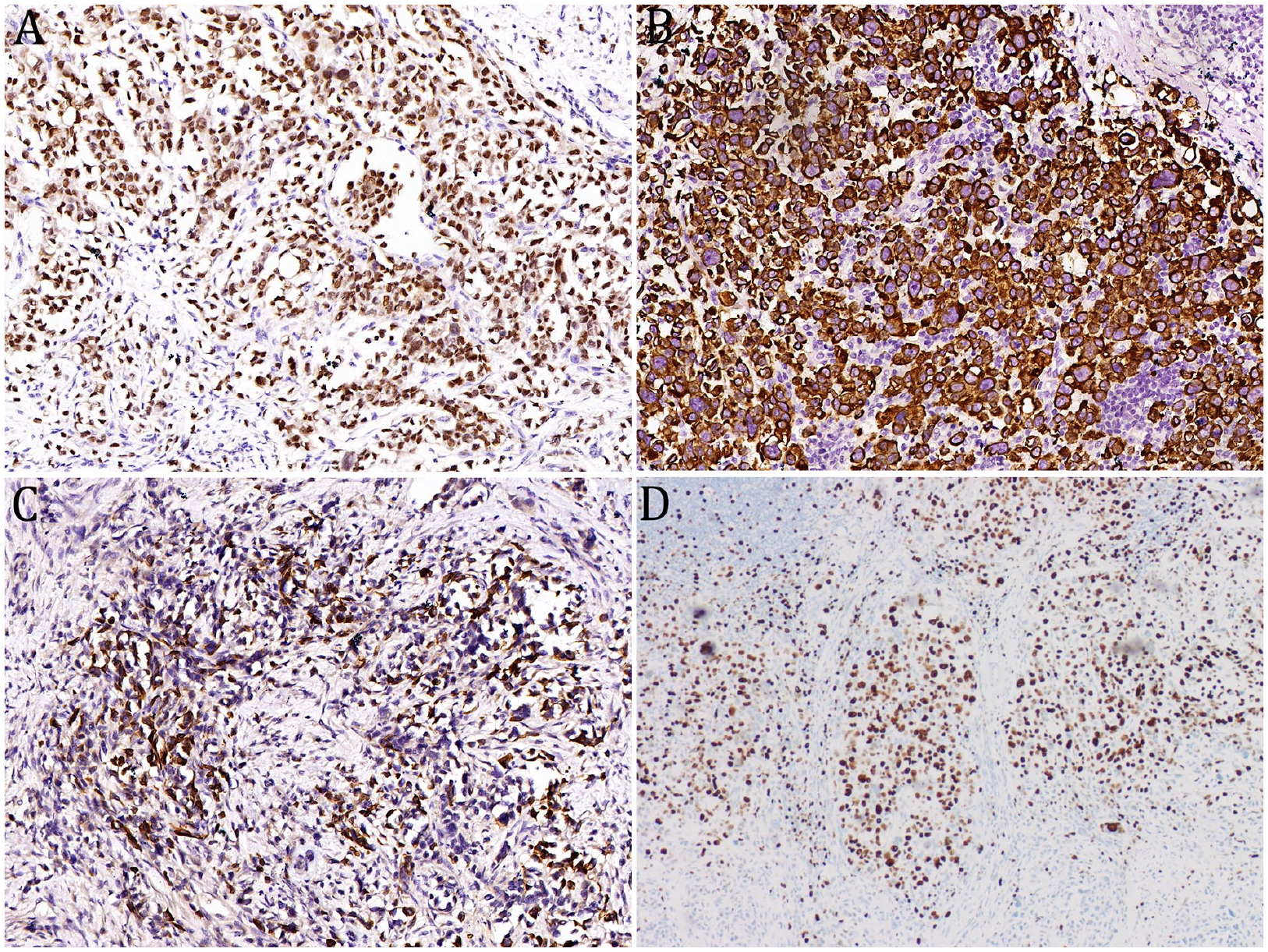
Immunohistochemical staining of inguinal lymph node metastatic carcinoma for GATA3 (A), CK7 (B), CK5/6 (C), and Ki-67 (D).
Cystoscopy revealed nodular protrusions in the bladder wall mucosa. Biopsy was obtained from the protuberant and triangular areas of the left bladder wall. Pathological examination revealed a polypoid mass, characterized by small, closely packed nests, with mild cell atypia and rare mitotic count. The stroma contained increased fibrous tissue, with no evidence of muscularis propria infiltration (Figure 3). The tumor displayed similarities to inverted papilloma but was different from tumor cells in inguinal lymph nodes. Immunohistochemical staining results indicated positive expression for Ki67 (10%), P53 (90%, strongly), GATA3, CK7, and CK5/6, while CK20, CD56, Syn, and CgA were negative (Figure 4). After the consultation of superior experts, the final pathological diagnosis was nested subtype of urothelial carcinoma (NS-UC).
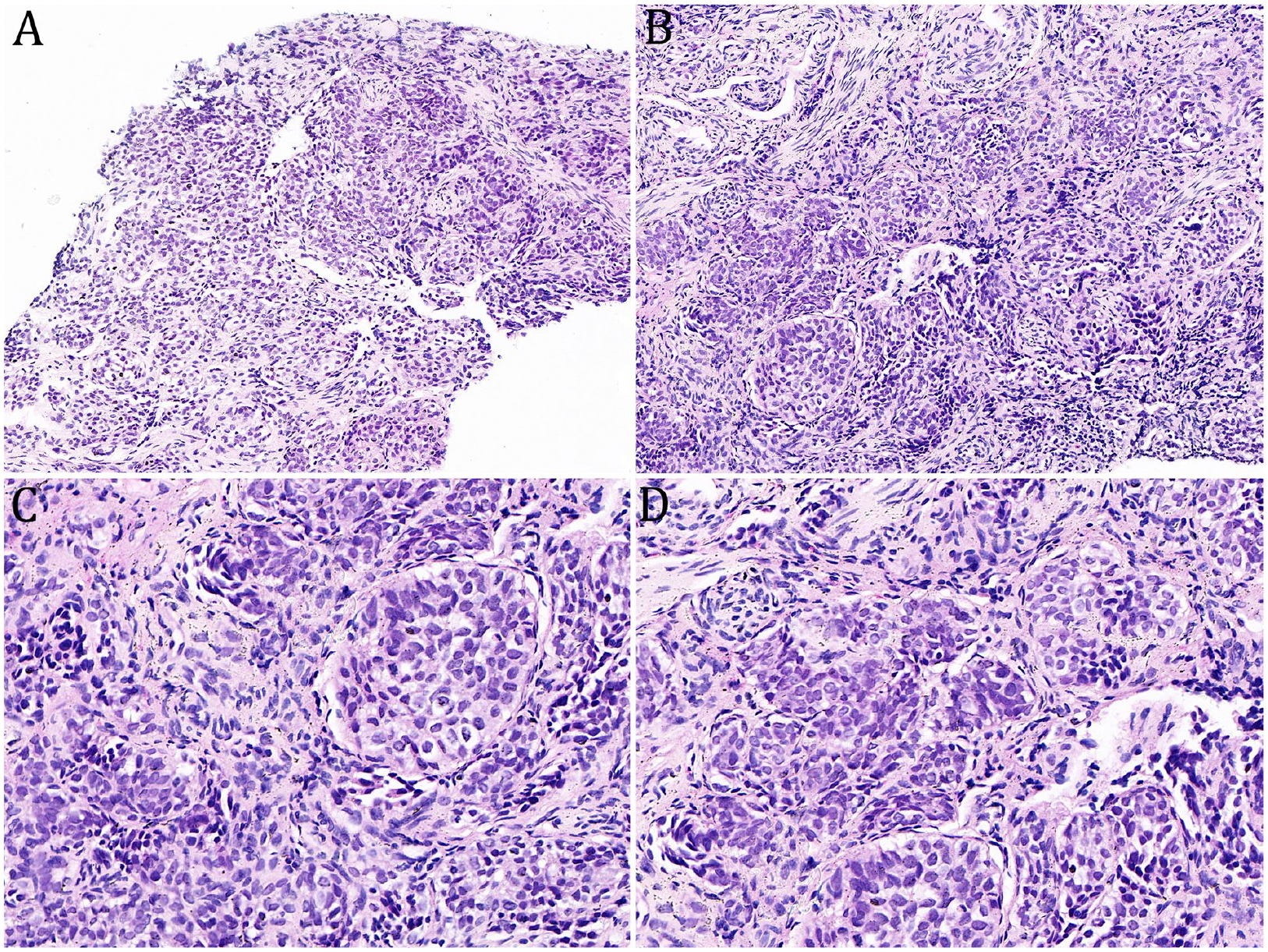
A nodular mass was identified, characterized by significant urothelial nest hyperplasia (A, B). The epithelial nests were small, closely packed, and exhibited mild cell atypia, with rare mitotic count. The stroma contained increased fibrous tissue and vascular proliferation, with no evidence of muscularis propria infiltration (C, D).

Immunohistochemical staining of bladder tumor for GATA3 (A), CK7 (B), CK5/6 (C), and Ki-67 (D).
Subsequently, the surgeon’s treatment recommendations for the patient were radical cystectomy and chemotherapy. Unfortunately, the patient declined further intervention and was subsequently discharged directly. Approximately 2 months later, the patient only sought pain relief through outpatient clinic visits and then discontinued follow-up. The current status of the patient, whether alive or deceased, cannot be determined.
Discussion
NS-UC is characterized by infiltrative nests of cytologically bland urothelial cells. Due to the bland features, a correct diagnosis can be delayed, particularly in superficial biopsy specimens. In our patient, no symptoms associated with bladder disease were observed, leading to a delayed diagnosis. While NS-UC primarily occurs in the bladder, recent reports indicate occurrences in the upper urethra, including the renal pelvis and ureter.4,5 In bladder cases, tumors are often located near the trigone and ureteral orifices. 6 Similarly, our case involved the bladder triangle and the left wall of the bladder.
Histologically, NS-UC has a deceptively bland appearance, consisting of small nests, single cells, and abortive tubules made of urothelial cells. The neoplastic cells infiltrate the lamina propria, often reaching the muscularis propria without involving the surface epithelium. These urothelial cells exhibit mild pleomorphism, a slightly increased nuclear/cytoplasmic ratio, and occasionally prominent nucleoli. 7 Features of malignancy such as mitotic activity, vascular invasion, and necrosis are not readily identified. 8 The nesting pattern is retained in lymph node metastases. 6 In our case, the mucosal layer of the bladder reveals a nodular mass. Microscopically, the mass is composed of numerous dense, small, irregular nests, with no fibrous tissue reaction. The neoplastic cells exhibit mild atypia, with a low count of mitotic. Due to the mild morphology of the tumor cells, an initial diagnosis of cancer could not be definitively made. Additionally, the morphology of the bladder tumor did not correspond to that of lymph node metastatic cancer, which typically demonstrates higher atypia, though some of tumor cells have mild dysplasia. Due to the presence of nest-like tumor cells with mild atypia and the generally similar immunohistochemical expression patterns (GATA3, CK7, ck5/6, p63, p53, etc.) observed in both specimens, it is reasonable to postulate that they are homologous tumors. The potential explanation for their morphological disparities lies in the fact that metastatic tumor cells may exhibit heterogeneity and transform into more divergent cellular phenotypes.
Due to histologic overlap, several benign entities, including von Brunn nests, nephrogenic adenoma, paraganglioma, and inverted papilloma, must be considered in the differential diagnosis when evaluating bladder lesions with nested-like morphology. 9 Von Brunn’s nests are clusters of urothelial cells within the lamina propria detached from the overlying epithelium. It is crucial to differentiate usual urothelial carcinoma involving von Brunn’s nests from NS-UC. Inverted papilloma consists of thin, anastomizing cords and nests of normal urothelium, with peripheral palisading of basal cells and central streaming. 10 Paraganglioma exhibits a cell-ball pattern with nests of tumor cells separated by narrow fibrovascular septa, and its exclusion can be confirmed by the absence of CgA and NSE reactivity. 11 In small superficial tissue samples, NS-UC with tubular formation can closely mimic nephrogenic adenoma. Immunohistochemistry shows that PAX8 is consistently expressed in nephrogenic adenomas, but in US-UC, it is only presented as focal positive.
Despite its bland histomorphology, NS-UC was associated with poor outcomes.12,13 It often presented at an advanced stage, displaying recurrence rates and survival similar to high-grade conventional urothelial carcinoma. 14 Linder et al demonstrated that approximately 69% of cases were in advanced stages (pT3/4) at the time of diagnosis, with 19% showing nodal involvement. 13 Our patient, in line with this trend, presented with initial lymph node metastasis. Given its aggressive nature, NS-UC should be approached clinically as a high-risk disease, and early cystectomy should be considered. Unfortunately, our patient declined further treatment and was subsequently discharged.
Conclusions
The diagnosis and treatment of NS-UC pose challenges due to its bland cytologic appearance and low incidence. Recognition of the nested subtype of urothelial carcinoma is crucial, as it is an aggressive tumor. This case, involving NS-UC with lymph node metastasis, contributes to raising awareness of this condition. Immunohistochemistry is helpful in determining the origin of lymph node metastatic carcinoma.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangxi Health Commission Fund (grant number Z-B20231374).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
NS-UC nested subtype of urothelial carcinoma; CT computed tomography.
Author Contributions
Ethical Approval
The studies were approved by the Ethics Review Committee of the Liuzhou Worker’s Hospital (Ethics Certificate No. KY2023101). Written informed consent was obtained from the patient for the publication of the case report.